

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Since the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was first identified, the virus has had a tremendous impact worldwide. The Republic of Korea, one of the countries with a high cumulative number of confirmed coronavirus disease 2019 (COVID-19) cases, also experienced a series of peaks and troughs in the disease outbreak and faced public health emergencies.1 However, the Republic of Korea has maintained a relatively low fatality rate compared with other countries. COVID-19 treatment has a wide spectrum because the disease varies from self-limiting to life-threatening cases.234 Therefore, the current COVID-19 treatment guidelines classify patients according to severity and recommend appropriate treatment for each patient.5 Patients with mild illness are defined as individuals who have any symptoms of COVID-19 but who do not show evidence of lower respiratory disease, and patients with moderate illness show signs and symptoms of lower respiratory disease and SpO2 ≥ 94% on room air at sea level. Patients in severe illness category have SpO2 < 94% on room air at sea level, a ratio of arterial partial pressure of oxygen to fraction of inspired oxygen < 300 mmHg, a respiratory rate > 30 breaths/min, or lung infiltrates > 50%. Critically ill patients with COVID-19 have respiratory failure, septic shock or multiple organ dysfunction.6 In patients with mild symptoms, symptomatic treatment is sufficient as it is for the common cold; however, various treatments for suppressing the proliferation of the virus or reducing the inflammatory response to prevent disease progression are being prescribed and studied for severe cases.7 Since the treatment of severe to critically ill patients with COVID-19 has changed with the accumulation of clinical and research experience after many trials and errors, we have reviewed and summarized the changes in guidelines and treatment experiences for severe to critically ill patients with COVID-19 in the Republic of Korea.
Go to : 
TIMELINES OF KOREAN COVID-19 TREATMENT GUIDELINES
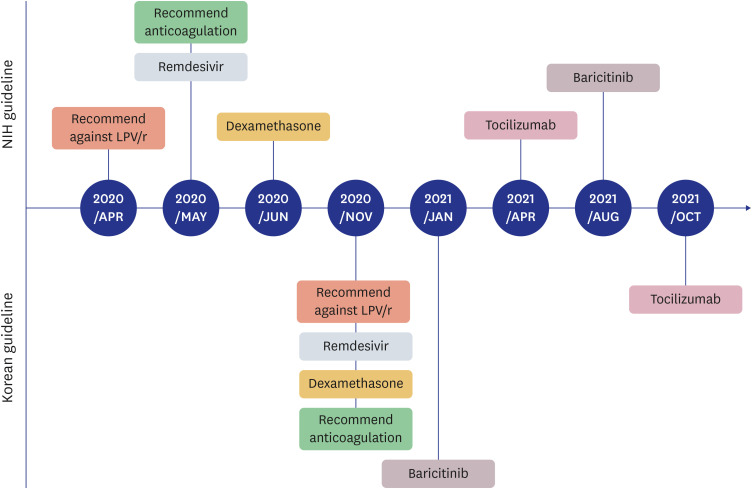
In the Republic of Korea, a number of related societies such as the National Medical Center – Office for the Central Infectious Disease Hospital – National Institute of Infectious Diseases, National Evidence based Healthcare Collaborating Agency – Korean Academy of Medical Sciences, and the Korean Society of Infectious Diseases have released guidelines to provide medical staff with information about evidence-based, standardized treatment for COVID-19.89101112 Among them, the first has been released and continuously updated since the beginning of the COVID-19 epidemic, so we would like to introduce those Korean COVID-19 treatment guidelines. This guideline was first released in November 2020 and has been updated in January 2021, October 2021, and February 2022 to reach the current guidelines. Although the lists of drugs recommended for or against each guideline are slightly different, the treatment of severe to critically ill patients with COVID-19 can be classified by antiviral drugs, immunomodulators, and adjunctive therapies such as anticoagulation and intensive care including mechanical ventilation and extracorporeal membrane oxygenation (ECMO). We have summarized the changes in the Korean guidelines for COVID-19 treatment in terms of antiviral drugs, immunomodulators, and anticoagulation and compared them with the National Institutes of Health (NIH) guidelines, which is a reference for treatment guidelines worldwide.5 The changes in the Korean guidelines and the comparison with NIH guidelines are shown in Figs. 1 and 2 respectively.
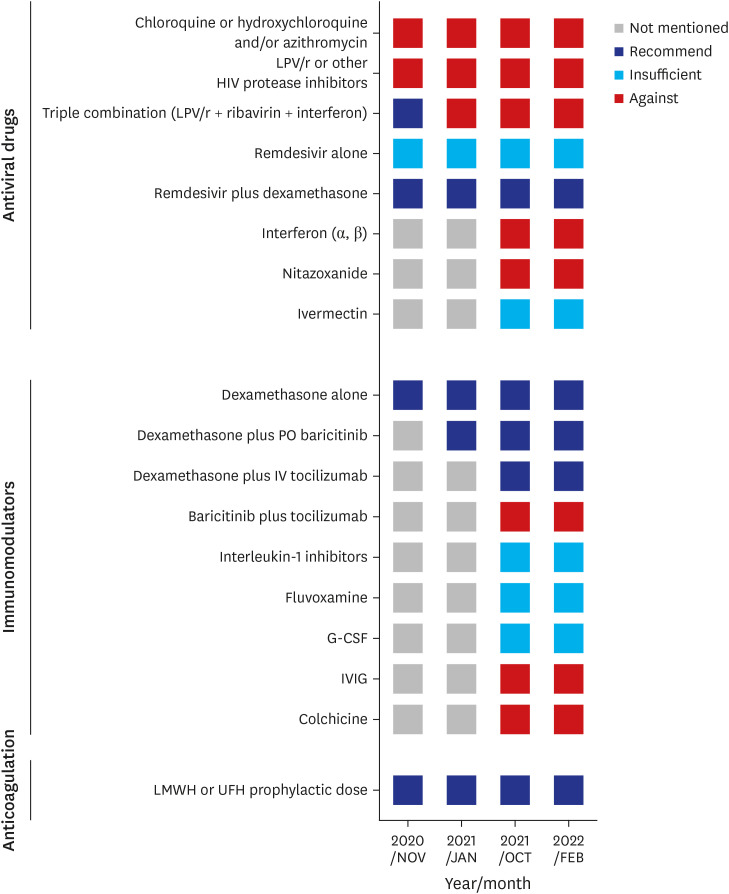 | Fig. 1Timelines of recommended treatments for severe to critically ill patients with coronavirus disease 2019 according to Korean guidelines.LPV/r = lopinavir/ritonavir, PO = taken by mouth, IV = intravenous, G-CSF = granulocyte colony stimulating factor, IVIG = intravenous immunoglobulin, LMWH = low-molecular–weight heparin, UFH = unfractionated heparin.
|
Antiviral drugs
Chloroquine and hydroxychloroquine have been used to treat malaria and intracellular bacterial infections and were used for COVID-19 treatment during the early pandemic because they were found to have anti-SARS-CoV activity in in vitro studies.13 However, they were not recommended for treatment in the first released guideline, regardless of patient severity because they were later proven to have no effect on COVID-19 through comparative clinical studies or meta-analyses.141516
Lopinavir/ritonavir (LPV/r) was also prescribed to patients with COVID-19 due to its potential antiviral effects. As numerous studies have shown that LPV/r do not demonstrate a clinical benefit among hospitalized patients with COVID-19,17 the NIH guidelines have recommended against the use of LPV/r monotherapy since May 2020; later the Korean guidelines followed later in November 2020. Notably, Korean guidelines suggested that if remdesivir is not available, a triple combination (LPV/r + ribavirin + interferon) can be administered early to patients who are likely to develop severe disease. However, subsequent guidelines withdrew this suggestion due to the lack of evidence.
Remdesivir is a nucleotide prodrug known to be effective against coronaviruses, including SARS-CoV and Middle East respiratory syndrome coronavirus.18 According to clinical trial data,19202122 the NIH guidelines began to recommend the use of remdesivir in the midst of a pandemic without any other drugs with evidence for their effectiveness. It was first available through the Food and Drug Administration (FDA) Emergency Use Authorization (EUA) and was later approved in October 2020. In the Republic of Korea, according to the announcement of the NIH guidelines, the government carried out special import (emergency introduction) of remdesivir, and in November 2020, the Korean guidelines began to recommend remdesivir for patients with COVID-19 in a hospital setting who had an SpO2 ≤ 94%. Due to the limitation of drug supplies and the lack of evidence, patients with high flow, non-invasive/invasive mechanical ventilation, or ECMO are considered the next priority. However, clinicians can consider remdesivir in combination with steroids in severely ill patients, and continue remdesivir therapy even if patients’ oxygen demand have aggravated under the remdesivir use.
Other antiviral drugs, such as interferon, nitazoxanide, and ivermectin, are not recommended in both the NIH and Korean guidelines. Anti-SARS-CoV-2 monoclonal antibodies including regdanvimab, are not recommended for patients with a high oxygen demand. In the cases with COVID-19 convalescent plasma, NIH guidelines and Korean guidelines both recommend against using convalescent plasma; although some studies have reported the possibility of the effectiveness of convalescent plasma.232425
Immunomodulator
Dexamethasone is a drug that has significant therapeutic effects on COVID-19. Many studies including the Randomised Evaluation of COVID-19 Therapy (RECOVERY) trial indicate that systemic corticosteroid therapy improves clinical outcomes and reduces mortality in hospitalized patients with COVID-19 who require supplemental oxygen.26 According to these results, the NIH guidelines recommend dexamethasone 6 mg daily for patients with oxygen demand and mechanical ventilation. The Korean guidelines have also recommended dexamethasone administration since November 2020. Dexamethasone is recommended for up to 10 days and can be replaced by equivalent doses of other corticosteroids.
Tocilizumab (anti-interleukin-6 receptor monoclonal antibody) is used because the systemic inflammatory response and respiratory failure observed severely ill patients with COVID-19 are associated with increases in proinflammatory cytokines. A number of randomized control trials have shown that tocilizumab is effective for COVID-19,2728 and the FDA approved tocilizumab under the EUA in combination with dexamethasone for hospitalized patients in April 2021. The indications were recently hospitalized patients who had been admitted to the intensive care unit (ICU) within prior 24 hours and who required mechanical ventilation or high-flow nasal cannula (HFNC) oxygen or recently hospitalized patients not admitted to the ICU who had rapidly increasing oxygen needs and required noninvasive ventilation or HFNC oxygen and who had significantly increased markers of inflammation. In the Korean guidelines, tocilizumab with steroids has been recommended since October 2021 for patients with the same indications.
Baricitinib (Janus kinase inhibitor) has been proposed as a treatment for COVID-19 because it can prevent the phosphorylation of key proteins involved in signal transduction that leads to immune activation and inflammation. Baricitinib had the clinical effectiveness in combination with remdesivir and dexamethasone, or with remdesivir according to the study Adaptive COVID-19 Treatment Trial.29 The NIH guidelines allowed the administration of baricitinib plus remdesivir for rare circumstances in which corticosteroids are contraindicated, but recommend against the use of a combination of baricitinib, dexamethasone, and remdesivir. Later, the guideline changed for patients who were recently hospitalized with rapidly increasing oxygen needs and systemic inflammation; baricitinib can be added to dexamethasone or dexamethasone plus remdesivir in August 2021. However, a combination of remdesivir plus dexamethasone with baricitinib (or remdesivir plus baricitinib when corticosteroids are contraindicated) has been recommended earlier in Korean guidelines since January 2021.
Other immunomodulators such as anakinra (interleukin-1 inhibitors), fluvoaxamine, granulocyte colony stimulating factor (G-CSF), intravenous immunoglobulin, and colchicine are not recommended, and further research is needed to obtain more evidence for both guidelines.
Anticoagulation
COVID-19 infection has been associated with a prothrombotic state with an increase in fibrin, and a number of studies have reported increased incidences of venous thromboembolism (VTE) in patients with COVID-19.30 Therefore, the NIH and Korean guidelines both recommend VTE prophylaxis in patients with oxygen demand. It is recommended that severely ill patients with COVID-19 receive subcutaneous or intravenous injections of low-dose, low-molecular-weight heparin or unfractionated heparin rather than oral anticoagulants.
Go to :
CLINICAL EXPERIENCES AND PRACTICES FOR COVID-19 TREATMENT IN SEOUL NATIONAL UNIVERSITY HOSPITAL (SNUH)
Antiviral drugs
At SNUH, prior to the introduction of remdesivir, hydroxychloroquine or lopinavir/ritonavir was usually prescribed to COVID-19 patients with oxygen demand (Fig. 3). If these patients worsened and needed to mechanical ventilation, the medical staff tended to maintain antiviral drugs because there were no other treatment options. However, since March 2020, when remdesivir became widely used in the SNUH, hydroxychloroquine and lopinavir/ritonavir were no longer prescribed.
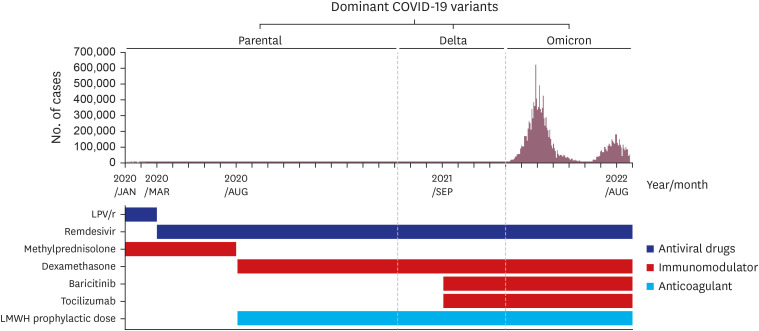
Since March 2020, remdesivir has been used for emergency use in patients who required oxygen treatment according to the NIH guidelines. As the SNUH is a government-designated referral medical center for patients with severe or critical COVID-19, many patients with HFNC, mechanical ventilation or ECMO were referred. For such patients, remdesivir was not initiated according to the guidelines. However, if the oxygen demand of a patient who was prescribed remdesivir deteriorated, medical staff maintained remdesivir for up to 10 days.
Interferon was not administered, except for the purpose of research during the early pandemic,31 and other antiviral drugs, including nitazonaxide and ivermectin, were not administered.
Immunomodulator
Before recommending dexamethasone, in the cases of patients with COVID-19 receiving mechanical ventilation, 1 mg/kg methylprednisolone was prescribed according to the treatment guidelines for acute respiratory distress syndrome (ARDS).32 Since dexamethasone was recommended in the NIH guidelines, dexamethasone (6 mg/day) has been administered in severely ill patients with COVID-19. If critically ill patients with COVID-19 admitted to the ICU are eligible for ARDS criteria, the medical staff prescribed 20 mg dose of dexamethasone according to the ARDS research.33
Baricitinib 4 mg/day for up to 14 days or until discharge has been prescribed to patients with HFNC who require rapidly increasing oxygen supplementation. Tocilizumab was more selectively prescribed in the patient whose oxygen demand suddenly increased.34 Routine use of baricitinib or tocilizumab in severe patients was hampered by concern about additional immunosuppression to that by dexamethasone, although baricitinib or tocilizumab was used more frequently in an ICU.
In some cases, immunoglobulin was administered, but it was not used for COVID-19 treatment, and other immunomodulators such as anakinra, fluvoxamine, or G-CSF were not used.
Anticoagulation
Initially, VTE prophylaxis was administered according to the general principles of intensive care.35 Depending on the patients’ bleeding tendency, a low-molecular-weight heparin prophylaxis dose was administered or intermittent pneumatic compression was applied, and heparinization was performed patients with ECMO. VTE prophylaxis was administered according to the individual situations of each patient. Since the need for anticoagulation emerged in the guidelines, VTE prophylaxis with usual prophylactic dose of low-molecular-weight heparin has been started in all patients whose movement has been restricted due to high-flow application in general isolation wards, even if the patients were not entering the ICU.
Go to :
CONCLUSION
In response to the unprecedented spread of infectious diseases and the emergence of mutations, numerous studies have been conducted to discover treatments for urgent needs. During the course of the pandemic, some studies showed conflicting results and some widely used drugs are no longer recommended. Even in this difficult situation, several guidelines for COVID-19 treatment based on clinical research and scientific evidence have been released and revised.36 These guidelines have helped medical staff respond effectively to patients with COVID-19. The guidelines have been established after several changes after the accumulated research and clinical experience. Currently, dexamethasone administration is one of the treatments proven to be effective in severe to critically ill patients with COVID-19, and remdesivir, baricitinib, and tocilizumab can be added depending on a patient’s situation. In addition, VTE prophylaxis is considered an indispensable treatment for patients with severe COVID-19.
Recently, the axis of COVID-19 research has changed from the discovery of treatments to the development of vaccines; however, several studies of COVID-19 treatment are still ongoing. COVID-19 is a newly emerging disease and a new field that requires much research. Therefore, it is necessary to regard the research and establish evidence-based guidelines.
Go to :
 XML Download
XML Download