

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) first emerged in late 2019 in patients presenting with pneumonia of unknown etiology, which was later named coronavirus disease 2019 (COVID-19). Soon after its discovery, the first case of COVID-19 in South Korea was confirmed in January 20, 2020.1 In less than 100 days, the World Health Organization (WHO) declared the COVID-19 pandemic.2 As of September 27, 2022, this zoonotic virus has infected more than 616 million people and claimed more than 6.5 million lives worldwide, both figures likely being vastly underestimated.3 People over 60 and people with chronic medical conditions are disproportionally affected by severe infections.45678
To mitigate the pandemic, interpersonal pathogen transmission must be halted by weakening viral replication. This is particularly challenging in the case of SARS-CoV-2 since asymptomatic persons, who constitute a considerable proportion of those infected, can still spread the virus. Universal masking and social distancing, especially the latter, are not sustainable because of long-term public fatigue. Antiviral drugs were unavailable at an early stage of the pandemic and would only become useful after infection. Therefore, safe and effective vaccines are the best measures to limit viral transmission.
The rapid development of highly effective and safe vaccines has exemplified the power of science during the COVID-19 pandemic. Notwithstanding, the pandemic also revealed darker aspects of modern society, such as the politicization of the pandemic response, health inequities, vaccine nationalism, and widespread misinformation. As a result, severe infections and deaths continue to occur, even with the availability of effective vaccines. Lingering disabling symptoms, collectively known as “long COVID,” also significantly compound the social burdens.910
Here, we review vaccine technologies that have been widely adopted during the current pandemic, as well as studies on COVID-19 vaccination in Korea. We also describe how mass vaccination has unfolded thus far and how we may respond to this pandemic in the future.
Go to : 
COVID-19 VACCINE PLATFORMS
Six COVID-19 vaccines have been authorized in Korea, including two messenger ribonucleic acid (mRNA) vaccines, two adenoviral vector vaccines, and two recombinant nanoparticle vaccines. ChAdOx1 nCoV-19 (Covishield™, Oxford-AstraZeneca) was first authorized on February 10, 2021, followed by BNT162b2 (Comirnaty™, Pfizer-BioNTech; March 5, 2021), Ad26.COV2.S (Jcovden™, Janssen; April 7, 2021), mRNA-1273 (Spikevax™, Moderna; May 21, 2021), NVX-CoV2373 (Nuvaxoid™, Novavax; January 12, 2022), and GBP510 (SKYCovione™, SK Bioscience; June 29, 2022) (Table 1). As of September 25, 2022, 128,710,064 doses of COVID-19 vaccines were administered: BNT162b2 (62.9%), mRNA-1273 (19.5%), ChAdOx1 (15.8%), Ad26.COV2.S (1.2%), NVX-CoV2373 (0.6%) and GBP510 (< 0.1%).11 The characteristics of each vaccine platform are summarized in Table 2.
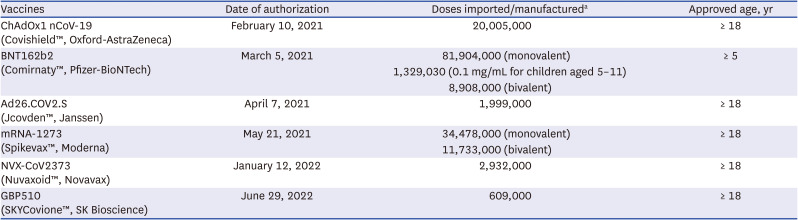
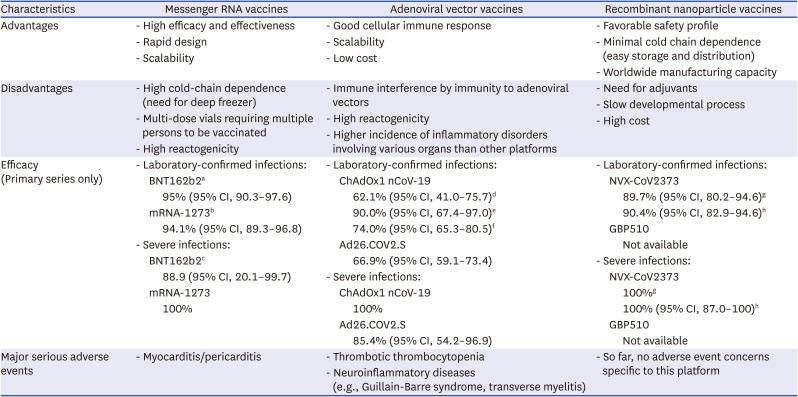
Table 1
Six coronavirus disease 2019 vaccines that have been authorized in Korea
aReported by Ministry of Food and Drug Safety, as of November 14, 2022.110
![]()
Table 2
Overview of the coronavirus disease 2019 vaccine platform
CI = confidence interval.
aCases were counted from seven days after the second dose; bCases were counted from 14 days after the second dose; cAll who received at least one dose were included in the analysis; dEfficacy in those who were primed by standard dose; eEfficacy in those who were primed by half dose; fEfficacy in the American trial111; gEfficacy in the UK trial29; hEfficacy in the American trial.28
![]()
mRNA vaccines were first commercialized during the COVID-19 pandemic. They contain mRNA encoding the peptide sequence of the SARS-CoV-2 spike protein (the main antigen) which is packed in lipid nanoparticles and delivered into cells, where it is translated as a whole or a specific portion of the antigen. mRNA vaccines have gained popularity because of their high efficacy and rapid production potential (Table 1).12 Their efficacy is the highest among the available COVID-19 vaccines, with 94–95% protection against laboratory-confirmed infections.1314 Moreover, the mRNA cannot integrate into the human genome because it does not enter the cell nucleus, averting concerns of acquired genetic diseases such as cancer and autoimmune diseases. On the other hand, mRNA vaccines have notable limitations such as restrictive storage conditions (notably in deep freeze due to mRNA instability) and multi-dose vial formulation.15 A noteworthy adverse event (AE) of mRNA vaccines against COVID-19 is myocarditis/pericarditis. COVID-19 mRNA vaccine-related myocarditis may be caused by autoimmunity (through mimicry between the spike protein and cardiac self-antigens) and hypersensitivity reactions.1617 Although the vast majority of myocarditis/pericarditis cases were mild, they contribute to vaccine hesitancy among young people.18
Adenoviral vector vaccines are not entirely new; based on this platform, an authorized vaccine against the Ebola virus disease (Ad26.ZEBOV and MVA-BN-Filo) had already been administered to over 20,000 individuals by April 2020.1920 However, due to the rarity of the Ebola virus disease outside of endemic regions, it was largely an unknown form of vaccine. An adenovirus vector is a replication-incompetent adenovirus that carries the genetic sequence of an antigen within its gene. When injected into the body, the vector enters the cell and releases its genome inside the nucleus. The genetic sequence is transcribed and translated to produce the antigen. Adenoviral vector vaccines have a notable advantage of inducing strong cellular immune responses.21 In addition, adenoviral vector vaccines are more stable than mRNA vaccines, forgoing the need for storage in extremely cold temperatures. They are not mutagenic because the DNA within the adenoviral vector is modified so that it does not integrate into the human genome. However, pre-existing immunity against vectors may reduce their immunogenicity.22 Despite the use of adenoviruses with low human seroprevalence (such as the chimpanzee adenovirus or human adenovirus type 26), adenoviral vector vaccines are generally less immunogenic and less effective compared to the mRNA vaccines.232425 In the ChAdOx1 nCoV-19 and Ad26.COV2.S trials, vaccine efficacy was in the range of 60–90%. In addition, there are concerns of rare but serious AEs, including vaccine-induced thrombosis with thrombocytopenia (VITT, approximately 10 per million doses) and Guillain-Barre syndrome (GBS, approximately 1 per million doses). While, after receiving an mRNA vaccine, only a small fraction of myocarditis/pericarditis cases were critical, VITT cases experienced a much higher fatality (22%) in a national cohort.1826
Recombinant nanoparticle vaccines could contribute to alleviating vaccine inequity with its scalable production and minimal cold chain dependence. Although they are classified as protein subunit vaccines, they differ in that the protein molecules are embedded in nanoparticles. These nanoparticle scaffolds enhance immunogenicity and protect protein molecules from proteases in the blood. A key strength of these vaccines is their favorable safety profile, as experienced in various kinds of infectious disease vaccines.27 However, protein subunit vaccines have a weakness to induce insufficient immune response, which can be strengthened by the addition of an adjuvant. Recombinant nanoparticle vaccines against COVID-19 were available later due to a slower developmental process than the other vaccines mentioned above, which is another weakness of protein-based vaccines. Two recombinant nanoparticle vaccines are available with domestic approval: NVX-CoV2373 and GBP510. NVX-CoV2373 is composed of stabilized and full-length recombinant SARS-CoV-2 spike protein trimers, which are assembled into nanoparticles and adjuvanted with Matrix-M.28 In the United Kingdom (UK) and the United States (US), NVX-CoV2373 was approximately 90% effective against laboratory-confirmed infections.2829 GBP510 is a self-assembling, two-component nanoparticle that is adjuvanted with AS03. The nanoparticle displays multiple conformational and conserved neutralizing epitopes of the SARS-CoV-2 receptor-binding domain. GBP510 was approved by a non-inferiority trial compared to ChAdOx1 nCoV-19, the first authorized vaccine in Korea. In the phase 3 clinical trial, the geometric mean titer ratio of the neutralizing antibody (NAb) was 2.93 (GBP 510 vs. ChAdOx1 nCoV-19) after two-dose primary series vaccination, satisfying the superior immunogenicity criteria.30
Go to :
STUDIES ON THE IMMUNOGENICITY OF COVID-19 VACCINES IN KOREA
There are several studies on the immunogenicity of the primary vaccination series in Korean adults.31323334 In all but one of the studies on the Ad26.COV2.S vaccine cohort, BNT162b2 was given three weeks apart and ChAdOx1 nCoV-19 was given 12 weeks apart. Participants who received BNT162b2 sustained higher NAb levels throughout the study period than ChAdOx1 nCoV-19 recipients. In all studies, antibody levels waned several months after the completion of the primary series, and the decline was faster in older participants.
A considerable number of healthcare workers (HCWs) received heterologous primary series vaccination (with ChAdOx1 nCoV-19 as the first dose and an mRNA vaccine as the second dose) because of the introduction of age restriction for receiving ChAdOx1 nCoV-19 due to concerns of VITT. Bae et al. recruited 199 HCWs who received 2 doses of ChAdOx1 nCoV-19 12 weeks apart (ChAd-ChAd group), 200 HCWs who received 2 doses of BNT162b2 3 weeks apart (BNT-BNT group), and 100 HCWs who received ChAdOx1 nCoV-19 as the first dose and BNT162b2 as the second dose 12 weeks apart (ChAd-BNT group). The study measured NAb levels using the plaque reduction neutralization test.35 The 50% neutralization dose of the BNT-BNT group (2,119, 95% confidence interval [CI], 1,756–2,556) and the ChAd-BNT group (2,367, 95% CI, 1,970–2,846) were similar, while also being significantly higher than that of the ChAd-ChAd group (392, 95% CI, 326–471). Non-Korean studies also reported that heterologous vaccination, with an adenoviral vector vaccine and an mRNA vaccine, was just as immunogenic as homologous vaccination with an mRNA vaccine. In terms of immunogenicity, it was also superior to homologous vaccination with an adenoviral vector vaccine, without significant differences in the AE profile.2336
Two studies on the immunogenicity of a fourth dose were identified.3738 In one, the National Institute of Infectious Diseases of Korea obtained blood samples 4 weeks apart from 74 residents in 2 long-term care facilities, in order to measure NAb levels.38 The NAb titer was 2–2.5 times higher at 2 weeks after the fourth vaccination than at 4 months after the third vaccination. There was another 6.4-to 7.4-fold increase in NAb titers at 4 weeks compared to 2 weeks after the fourth dose.
Hybrid immunity by natural SARS-CoV-2 infection and vaccination was also studied.394041 In a study by Noh et al.,41 a robust NAb immune response was induced even with a single-dose of COVID-19 vaccination, when vaccinated at long intervals (more than 12 months) after SARS-CoV-2 infection. However, remarkable ceiling effects were observed with repeated vaccinations. In a study by Kang et al.,39 similar NAb titers were induced between uninfected individuals who received two-dose mRNA vaccines and prior-infected individuals who received single-dose mRNA vaccine. Among prior-infected individuals, Nab titers were significantly higher in vaccine recipients at around 18 months compared to those vaccinated within six months after SARS-CoV-2 infection. Consistent with the study by Noh et al.,41 vaccinating twice after SARS-CoV-2 infection did not raise NAb titers further. In prior-infected individuals, Choi et al.40 reported higher NAb levels and a broader neuralization spectrum induced by a fourth vaccination with NVX-CoV2373, compared to those in uninfected counterparts. Although limited by small sample sizes, these findings are consistent with non-Korean studies and suggest important considerations in establishing vaccination policies for people who had COVID-19.4243
Go to :
REAL-WORLD EFFECTIVENESS OF COVID-19 VACCINES IN KOREA
Two studies on primary series vaccine effectiveness (VE) in adults were identified (Fig. 1, Table 3).4445 In one, the incidence of laboratory-confirmed SARS-CoV-2 infection of any severity and severe infection was compared between unvaccinated people and those vaccinated at least once from March 13, 2021, to October 21, 2021.44 Among unvaccinated individuals, the age-adjusted incidence of infection of any severity (5.69 per 100,000 person-days) was 1.9 times higher than that among partially vaccinated individuals (3.05 per 100,000 person-days) and 2.7 times higher than that among fully vaccinated individuals (2.13 per 100,000 person-days). This translated into an overall VE of 63%. The age-adjusted incidence of severe infection in unvaccinated individuals was 0.16 per 100,000 person-days, compared to 0.02 per 100,000 person-days in people vaccinated at least once, resulting in a VE of 93%.
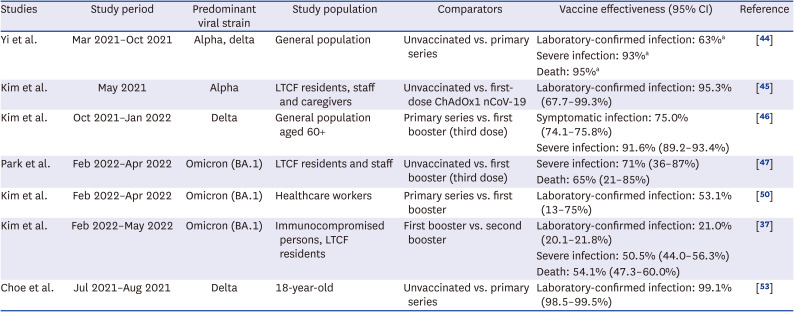
 | Fig. 1Vaccine effectiveness against laboratory-confirmed coronavirus disease 2019 across severe acute respiratory syndrome coronavirus 2 variants and study population. The numbers displayed at the top right of each item in superscript refer to the citation number.
|
Table 3
Summary of studies on coronavirus disease 2019 vaccine effectiveness in Korea
| Studies | Study period | Predominant viral strain | Study population | Comparators | Vaccine effectiveness (95% CI) | Reference |
|---|---|---|---|---|---|---|
| Yi et al. | Mar 2021–Oct 2021 | Alpha, delta | General population | Unvaccinated vs. primary series | Laboratory-confirmed infection: 63%a | [44] |
| Severe infection: 93%a | ||||||
| Death: 95%a | ||||||
| Kim et al. | May 2021 | Alpha | LTCF residents, staff and caregivers | Unvaccinated vs. first-dose ChAdOx1 nCoV-19 | Laboratory-confirmed infection: 95.3% (67.7–99.3%) | [45] |
| Kim et al. | Oct 2021–Jan 2022 | Delta | General population aged 60+ | Primary series vs. first booster (third dose) | Symptomatic infection: 75.0% (74.1–75.8%) | [46] |
| Severe infection: 91.6% (89.2–93.4%) | ||||||
| Park et al. | Feb 2022–Apr 2022 | Omicron (BA.1) | LTCF residents and staff | Unvaccinated vs. first booster (third dose) | Severe infection: 71% (36–87%) | [47] |
| Death: 65% (21–85%) | ||||||
| Kim et al. | Feb 2022–Apr 2022 | Omicron (BA.1) | Healthcare workers | Primary series vs. first booster | Laboratory-confirmed infection: 53.1% (13–75%) | [50] |
| Kim et al. | Feb 2022–May 2022 | Omicron (BA.1) | Immunocompromised persons, LTCF residents | First booster vs. second booster | Laboratory-confirmed infection: 21.0% (20.1–21.8%) | [37] |
| Severe infection: 50.5% (44.0–56.3%) | ||||||
| Death: 54.1% (47.3–60.0%) | ||||||
| Choe et al. | Jul 2021–Aug 2021 | Delta | 18-year-old | Unvaccinated vs. primary series | Laboratory-confirmed infection: 99.1% (98.5–99.5%) | [53] |
![]()
There are some VE studies on booster doses as well. The Korean Disease Control and Prevention Agency (KDCA) collected data from 10,999,292 Koreans aged 60 years or older and compared the rates of symptomatic SARS-CoV-2 infection, severe infection, and mortality between individuals who received only 2-doses of COVID-19 vaccine and those who received 3-doses.46 The study period was from October 2021 to January 2022, during which the delta variant (B.1.617.2) was predominant. The adjusted VE of a third dose was 75.0% (95% CI, 74.1–75.8%) for symptomatic infections, 91.6% (95% CI, 89.2–93.4%) for severe infections, and 92.3% (95% CI, 88.7–94.8%) for death. The KDCA also investigated VE in 2,241 patients and HCWs in 5 long-term care facilities from February 6, 2022, to April 2, 2022, when the omicron variant (BA.1) was predominant.47 People over 60 years old accounted for 67.6% and those over 75 years accounted for 38.3%. Compared to unvaccinated individuals, those who received only 2-doses had a VE of 54% (95% CI, −19 to 82%) for severe COVID-19 and 53% (95% CI, −29 to 83%) for death, adjusted for age, sex, and antiviral drug use. The adjusted VE was higher in people who received booster doses (a third dose): 71% (95% CI, 36–87%) for severe COVID-19 and 65% (95% CI, 21–85%) for death. Although the studies were not directly comparable due to differences in the study population, vaccine administration, and study design, the findings summarized above nonetheless support the conclusions of non-Korean studies.4849 In a retrospective single-center study, Kim et al.50 compared primary series vaccinations (2 doses) and booster vaccinations (a third dose) in terms of prevention of laboratory-confirmed SARS-CoV-2 infection in February 2022. The adjusted VE of the third vaccination was 53.1% (95% CI, 13–75%). However, when the time elapsed after vaccination was included in the multivariable analysis, the statistical significance of VE disappeared (29%; 95% CI, −50 to 66%), suggesting that the time since the last vaccination may be more important than having the third dose itself.
Additionally, KDCA investigated the VE of a fourth dose in immunocompromised people and residents of long-term care facilities.37 From February 16, 2022, to April 30, 2022, a total of 1,509,970 individuals who received a third dose more than 4 months ago were included. Fourteen days after vaccination, the VE of the fourth dose was 21.0% against laboratory-confirmed infection, 50.5% against severe COVID-19, and 54.1% against death. Thirty days after the fourth dose, the VE against infection decreased to 8.9%. While there was a remarkable increase in NAb levels 4 weeks after the fourth dose in the previous study, this might have been inadequate to protect against the omicron variant.38 Canadian and Swedish studies on fourth doses in high-risk individuals reported similar values.5152
To date, only one large-scale VE study is available in the pediatric population because of the low vaccine uptake rate, especially in younger children.53 In 2021, high school students (aged 18 years old) were required to be vaccinated before the national college entrance exam. Of 454,876 students, 95.4% completed the primary series. Choe et al. combined COVID-19 case reports from the Ministry of Education and data from the national immunization registry to estimate the VE among students. They found that the VE against laboratory-confirmed SARS-CoV-2 infection was 99.1% (95% CI, 98.5–99.5%) at 14 days after the first dose vaccination.
Go to :
VACCINE EFFECTIVENESS AGAINST THE OMICRON BA.4/5 SUBVARIANTS
Since the omicron has become the dominant variant, it has not been replaced by an entirely new variant as before, but rather by its own subvariants. As of November, 2022, BA.4 and BA.5 (collectively called BA.4/5) are the most frequently encountered variants in Korea. These variants can evade immunity more effectively than BA.1/2, which are earlier subvariants which already had significant immune-evading capabilities.54 Up until mid-November, 2022, there has been no Korean study on the VE against omicron BA.4/5, and it has to be extrapolated from non-Korean studies. The largest study (n = 123,236) analyzed the VE of 3- and 4-doses of mRNA-1273 against BA.4/5-related hospitalization using the US Kaiser Permanente healthcare system data.55 The VE of mRNA-1273 against hospitalization was 72.4% for 3-doses and 88.5% for 4-doses. Studies in the US and UK also showed significant VE (60–70%) against BA.4/5-related hospitalization within 3–5 months after the last vaccination (third or fourth dose of the mRNA vaccine).565758 However, a study reported that significant VE could not be expected 6 months after the third dose or 3 months after the fourth dose of BNT162b2.58 A study in South Africa conducted an elapsed time-stratified analysis for VE after the third dose of BNT162b2 against BA.4/5-related hospitalization, which showed a decrease in VE over time: 47.7% 3–4 months after the second dose, 26.3% 5–6 months after the second dose, 68.8% 1–2 months after the third dose, and 46.8% 3–4 months after the third dose.59 The VE against omicron BA.4/5-related hospitalization declined rapidly after the first or second booster, suggesting a limited role of the original SARS-CoV-2-based vaccines.5558
To maintain VE against the omicron subvariants, the two most widely used mRNA vaccines have been modified to include mRNA of the original SARS-CoV-2 and omicron subvariants (BA.1 or BA.4/5). These “bivalent” vaccines reportedly boost NAb titers, comparable to those induced by the original boosters, against the original SARS-CoV-2, while achieving superior titers against the omicron subvariants.6061 While the BA.1-modified bivalent vaccine induces NAb against BA.4/5, the increment is smaller (about 30%) than that against BA.1.60616263 To maximize protection against the currently dominant variant, BA.4/5-modified bivalent vaccines have been developed. In a phase 2/3 study, including 511 participants (aged 19–89), Moderna’s BA.4/5-modified bivalent vaccine (mRNA-1273.222) demonstrated superior NAb titers over mRNA-1273 with comparable safety profiles.61 The geometric mean titer ratio was 5.11 (95% CI 4.10–6.36) for those with prior SARS-CoV-2 infection, and 6.29 (95% CI 5.27–7.51) for those without. An exploratory analysis (n=40) revealed a robust neutralizing activity against BQ.1.1, a subvariant that has been on the rise since this fall, despite an approximately five-fold drop in titers compared to against BA.4/5.61 In contrast, a small-sized real-world study demonstrated no significant difference in NAb titers against BA.5 between BA.4/5-modified bivalent (n = 18) and original monovalent booster recipients (n = 15); a modest nonsignificant trend favoring the bivalent booster by a factor of 1.3 was seen.64 The bivalent BA.4/5-modified VE might vary depending upon the recipient's past vaccination status and history of prior SARS-CoV-2 infection (elapsed time from past infection and variants). Actually, according to a recent report by US Centers for Disease Control and Prevention, the real-world VE of BA.4/5-modified bivalent vaccine against symptomatic SARS-CoV-2 infection was variable by age and the elapsed time since the last monovalent dose.65 When administered at 2–3 months and ≥ 8 months after the last monovalent dose, the relative VE (compared to those who did not receive a bivalent booster) of a booster dose of BA.4/5-modified bivalent vaccine among ≥ 2 dose monovalent vaccine recipients was 30% and 56% for individuals aged 18–49 years, 31% and 48% for individuals aged 50–64 years, and 28% and 43% for individuals aged ≥ 65 years, respectively. Relative VE increased with time since the most recent monovalent vaccine dose. Compared to unvaccinated individuals, the absolute VE of a booster dose of BA.4/5-modified bivalent vaccine among persons who had received ≥ 2 monovalent doses was 43% (95% CI, 39–46%) for adults aged 18–49 years, 28% (95% CI, 22–33%) for adults aged 50–64 years, and 22% (95% CI, 15–29%) for the elderly aged ≥ 65 years, respectively.
Go to :
ADVERSE EVENTS OF COVID-19 VACCINES IN KOREA
As COVID-19 vaccine rollout progressed across the country, a wide range of AEs were reported.66676869 Aside from solicited AEs, the vast majority of them, especially serious AEs, were unlikely to be caused by vaccines. Investigations on AEs so far are reassuring, without significantly abnormal signals. Even so, the AEs provoked public backlash and became a major reason behind vaccine hesitancy.
According to the latest KDCA biweekly report, 3.72 cases of AEs were reported for every 1,000 vaccine doses, 3.6% of which were serious AEs.11 People who received Ad26.COV2.S (5.88 per 1,000 doses) reported AEs the most often, followed by ChAdOx1 nCoV-19 (5.42 per 1,000 doses), mRNA-1273 (4.49 per 1,000 doses), BNT162b2 (3.03 per 1,000 doses), and NVX-CoV2373 (1.39 per 1,000 doses). Vaccine recipients in their 30s reported more cases of AEs (4.93 per 1,000 doses), and those over 80 had reported the least number of cases (1.98 per 1,000 doses). Women (4.71 per 1,000 doses) reported more AEs than did men (2.70 per 1,000 doses). Furthermore, the number of AE reports decreased with repeated vaccinations (first dose, 5.37 per 1,000 doses; second dose, 4.11 per 1,000 doses; third dose, 1.68 per 1,000 doses; fourth dose, 0.66 per 1,000 doses). The 3 most common AEs were headaches, myalgia, and dizziness, similar to clinical trial results.131470 During the first 8 months of national immunization, only 2 out of 835 deaths that occurred after vaccination had a causal relationship with vaccination.71 The incidence of anaphylaxis was 5.8 per million doses, which is similar to the US and European Union statistics.72
Several hospitals analyzed vaccine AEs reported by their employees, who were largely young females.7374757677 All studies found that AEs were more commonly reported by females than males and by younger individuals than older individuals. Among 4,699 vaccinated HCWs in the studies which included AE severity data, only one person experienced serious AE.7577
Children and adolescents reported fewer AEs than adults (5–11-year-olds, 0.79 per 1,000 doses; 12–18-year-olds, 3.20 per 1,000 doses).11 KDCA reviewed AEs in adolescents aged 12–17 reported through February 2022.78 Out of 12,216 AEs, there were 85 suspected cases of anaphylaxis, 74 suspected cases of myocarditis/pericarditis, 2 cases of suspected multisystem inflammatory syndrome, and 2 deaths. The KDCA concluded that the deaths were unrelated to vaccination. Similar to data in adults, the most commonly reported AEs were injection site pain, headaches, fatigue, and myalgia, consistent with the results from a clinical trial and a US surveillance study.7980
However, the AE patterns of adolescents differed from those of the adults. Lee et al.81 analyzed data from the Korean vaccine AE reporting system to compare the risk and types of AEs in adolescents (aged 12–15) with those in adults. Compared to adults, adolescents had a higher incidence of encephalitis/myelitis, convulsions, GBS, myocarditis/pericarditis, lymphadenopathy, lymphopenia, and multisystem inflammatory syndrome. Among these, the relative risk was highest for multisystem inflammatory syndrome (244.3, 95% CI, 31.27–1,908.38).
Neuroinflammatory diseases, such as GBS, have long been associated with vaccination, despite no clear evidence of a causal relationship outside of influenza vaccines.8283 The KDCA reviewed 101 alleged GBS cases reported up to August 19, 2022, and concluded that 22 of them were likely GBS, though there was insufficient evidence that vaccines were responsible. Two out of 22 cases occurred after Ad26.COV2.S vaccination, and the rest occurred after receiving ChAdOx1 nCoV-19.
Some serious AEs deserve closer scrutiny for each vaccine product. Drawing particular attention were VITT and myocarditis/pericarditis after receiving adenoviral vector vaccines and mRNA vaccines, respectively. As of August 19, 2022, 4 out of 213 suspected VITT cases were causally related to vaccination, which translates to 9.74 cases per million doses of the adenoviral vector vaccine.11 This number is lower than in the UK (15.8 per million doses) and Canadian (23 per million doses) statistics.8485 All 4 cases occurred after receiving ChAdOx1 nCoV-19: 3 after the first dose and 1 after the second dose. As of September 22, 2022, 749 cases (7.08 per million doses) of myocarditis/pericarditis have been identified after receiving an mRNA vaccine.11 For comparison, the incidence was 4.6 per million doses in the US, 10–18 per million doses in the UK, and 11–17 per million doses in Canada.848586 To a lesser extent, these conditions also occurred in those who received adenoviral vector vaccines (28 cases; 1.28 per million doses) or recombinant nanoparticle vaccines (3 cases; 3.96 per million doses).11 In these cases, the diagnosis of myocarditis/pericarditis was verified by KDCA but were not necessarily proven to be caused by vaccination.
As described so far, COVID-19 vaccines are safe and effective in both children and adults, justifying mass vaccination during the pandemic. Nevertheless, the National Vaccine Injury Compensation Program was launched to guarantee vaccine safety and to support people who experience rare AEs. HCWs or patients can report AEs online or via text messages and file a petition at the community health center. This is subsequently reviewed by the KDCA, Vaccine Injury Compensation Committee (composed of 15 members, including medical and legal experts), or local government within 12 weeks.8788 On July 19, 2022, a department dedicated to vaccine injury compensation was established.89 Additionally, the maximum subsidy for COVID-19 vaccination-related AEs was raised from 30 million Korean Won (KRW) to KRW 50 million (approximately USD 37,800, as of November 15, 2022); for mortality, it was raised from KRW 50 million to KRW 100 million.89 Also, patients with AEs without a clear causal relationship to vaccination (i.e. temporal association with vaccination, but insufficient causality data) can be compensated up to KRW 30 million since May 17, 2022.87 As of August, 2022, 20,801 patients (15.9 per 100,000 vaccinations) have been compensated under the program.88
Go to :
MASS VACCINATION AND THE MITIGATION OF PANDEMIC WAVES
The mass vaccination timeline through October 2, 2022, including cumulative vaccination rate, vaccine eligibility, case incidence, and excess mortality, is presented in Fig. 2. Shortly following the emergency approval of ChAdOx1 nCoV-19, the national immunization program began on February 26, 2021. Patients and HCWs in long-term care facilities and HCWs who directly provided care for COVID-19 patients were prioritized for vaccination.90 Due to supply shortages, the ChAdOx1 nCoV-19 vaccine was administered at longer intervals (3 months) than tested in clinical trials to vaccinate a maximal number of people at least once. On April 8, 2021, ChAdOx1 nCoV-19 vaccinations were paused due to concerns over VITT. ChAdOx1 nCoV-19 vaccinations then resumed a few days later for individuals over 30 years old, due to concerns of a higher risk for VITT in younger people.9192 The age limit was revised to 50 years-old or above in July 2021.
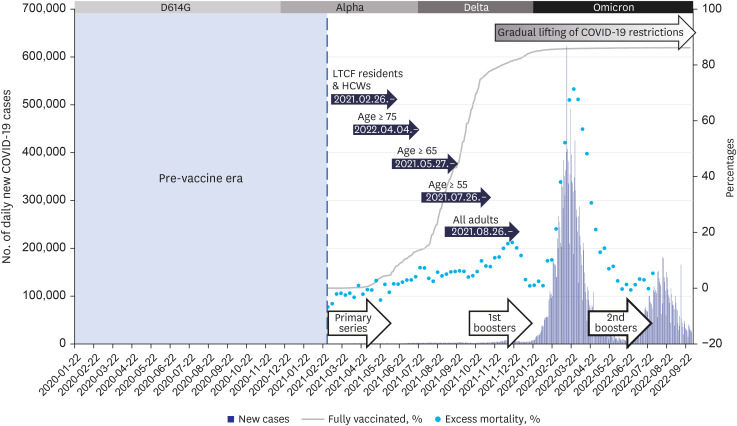 | Fig. 2Timeline of mass vaccination against COVID-19 in Korea. The blue vertical bars represent the number of daily new COVID-19 cases, the light blue dots represent weekly excess mortality (%), the grey curve represents the cumulative percentage of fully vaccinated individuals (i.e., completed primary series vaccination), and the dark blue arrows represent when each group became eligible for COVID-19 vaccines.COVID-19 = coronavirus disease 2019, LTCF = long-term care facilities, HCWs = healthcare workers.
|
During the summer pandemic wave of 2021, led by the delta variant, the number of unvaccinated middle-aged patients overtook older patients in the COVID-19 wards and critical care units. Many of them had comorbidities such as obesity and diabetes.93 Several months later, as the percentage of older patients rose again due to waning vaccine-induce immunity, KDCA distributed “booster shots,” a third vaccine dose, to those who completed the primary series at least 4 months ago. After the intensive delivery of booster shots in December 2021, the number of cases and deaths declined again in January 2022.
Despite these efforts, the number of cases drastically rose since February 2022 as the notoriously immune-evading omicron variant became predominant.94 In mid-April 2022, South Korea became the country with the second highest cumulative number of confirmed cases per capita among the G20 nations.95 While case-fatality rates remained lower than in the previous pandemic waves, suppressed by vaccine-induced immunity, excess mortality rates were much higher, likely due to the sheer volume of COVID-19 cases overwhelming healthcare systems.96
It became obvious that vaccine-induced protection against symptomatic infection wanes within months. Since April 2022, people over 60, who accounted for the majority of severe infections and deaths, are encouraged to receive a booster.38 As of September 29, 2022, 43.7% of people over 60 have received a fourth shot.97 In late August 2022, the KDCA recommended the bivalent boosters, prioritizing high-risk individuals for the coming fall and winter.98
Go to :
THE WAY FORWARD
Although the worst phase of the pandemic seems to be behind us, much work remains to be done. First, the need for additional vaccinations should be clarified. The target population and time interval between doses should also be addressed. Through repeated vaccination and past natural infections, long-lasting memory B cells and T cells may have already been induced in most people. When exposed to SARS-CoV-2, memory B cells can react immediately to produce NAbs against the virus. Moreover, through germinal center reaction, memory B cells and long-lived plasma cells further mature to generate NAbs with high affinity and diversity. These antibodies could better cross-neutralize variant viruses.99 Additionally, T-cell immunity is more cross-reactive and longer sustained than humoral immunity, providing protection against severe SARS-CoV-2 infection for over a year.100 Thus, it is unclear whether annual revaccination is necessary for the general population. Nonetheless, given that humoral immunity declines faster in older adults and chronically ill patients, repeated booster administration would be reasonable for populations at higher risk of morbidity and mortality.101 Most probably, 1 or 2 boosters would be needed annually, depending on the accompanying medical conditions of the individual.
Second, the approval process for new COVID-19 vaccines, which are developed by replacing viral antigens of an approved vaccine platform should be simplified. The US Food and Drug Administration’s emergency-use approval of BA.4/5-modified bivalent vaccine was based on preclinical data in the absence of clinical trials. This was possible due to the experience when developing beta-variant-modified and BA.1-modified bivalent vaccines; there was a high correlation between the clinical trial results and preclinical research with similar safety profiles. Such a review/approval system is based on preclinical data, including toxicity and immunogenicity, and has been applied to influenza vaccines for years.
Third, it is uncertain whether we need multivalent vaccines that contain several different SARS-CoV-2 variant antigens, as in the case of the influenza vaccine. It is difficult to predict because the COVID-19 pandemic is ongoing; however, unlike influenza, in which four types of viruses (A/H1N1, A/H3N3, B/Yamagata, and B/Victoria) are concurrently prevalent in each season, several SARS-CoV-2 variants might circulate at different times, which diminishes the usefulness of the multivalent vaccine. Nevertheless, given the frequent appearance of new SARS-CoV-2 variants, a multivalent vaccine could still be beneficial at increasing cross-reactive immunity. The usefulness of the multivalent vaccine will be further revealed through the upcoming adoption and subsequent evaluation of bivalent vaccines, as well as the monitoring of variant emergence frequencies in the course of transitioning to endemicity.
Fourth, effective communication is crucial to a pandemic response.102 Even the best, groundbreaking research is useless if communicated poorly or left unapplied to the real world. Although anti-vaccine sentiment and vaccine hesitancy have always been present, they have risen to prominence in this once-in-a-century global disaster. Serious but rare AEs provoked fear, and breakthrough infections undermined public trust in vaccines, even while such infections were accounted for and the benefits of vaccination still far outweighed the risks.103 Of particular concern are patients with comorbidities who are reluctant to get vaccinated against COVID-19, despite the recommendations of health authorities worldwide.104 Additionally, while vaccines are the key component of a successful pandemic response, they alone can fail without non-pharmaceutical interventions like appropriate masking and social distancing. Reflecting on the surge of the omicron variant in early 2022 and the subsequent rise in excess mortality to levels higher than the pre-vaccine era, the government had seemingly failed to deliver this message. On the other hand, authorities should also use caution when implementing coercive measures such as the Vaccine Pass. Communicating accessibly and reliably with the public, decoupling vaccines from politics, and delegating decisions to health experts will together help us respond to this and the next pandemics.
Finally, in preparation for the next pandemic, it is essential to make strategic and sufficient investments in vaccine research and development. In the absence of domestic vaccine development in the first half of 2021, South Korea had experienced delayed COVID-19 vaccine delivery, which could have led to preventable morbidity, mortality, economic loss, and a delayed return to normalcy. Up until August 2022, 10 vaccine candidates developed by 7 domestic companies have been approved to undergo clinical trial.105 These include 3 mRNA vaccines, 1 DNA vaccine, 2 viral vector vaccines, and 4 recombinant vaccines. Only one recombinant nanoparticle vaccine out of the 10 candidates was approved in mid-2022, far behind the global competition. The rapid development of COVID-19 vaccines in the US and UK was facilitated by access to multiple vaccine platform technologies, experienced vaccine developers, and regulatory agencies that oversaw non-clinical to phase 1 clinical trials of numerous vaccines against various infectious diseases. However, South Korea’s potential is now being recognized internationally. SK bioscience and Samsung Biologics are producing NVX-CoV2373 and mRNA-1273, respectively, as contract manufacturing organizations.106107 In February, 2022, the WHO designated South Korea as a new global biomanufacturing training hub to provide technical and hands-on experience to professionals from low- and middle-income countries.108 A research ecosystem that connects clinical needs-based vaccine development to nonclinical and clinical trials should be established for continued progress.109 This should occur alongside the promotion of ample investment in research and development. These lessons must be heeded, lest the same mistakes be repeated when the next pandemic strikes.
Go to :
CONCLUSION
The COVID-19 pandemic has tested the healthcare system and the pandemic preparedness of South Korea. When the next pandemic arrives, we should be better at doing risk communications, vaccine development and distribution, while maintaining high adherence to vigilant surveillance, social distancing, and vaccination.
Go to :
 XML Download
XML Download