

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
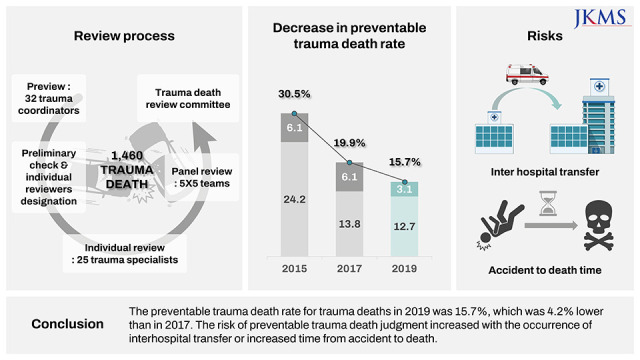
Trauma, both in Korea and globally, is a major cause of death in populations aged 39 years or younger. Unlike cancer and cardiovascular diseases, most nations treat trauma as an important public health issue, since it causes deaths and disabilities in the socioeconomically active age groups of the population.1234 To reduce the massive socioeconomic losses caused by trauma, trauma care quality must be strictly managed at the national level.5 Expert panel review of trauma deaths is a traditional method of quality management for trauma treatment, both for evaluating its quality and for identifying issues in the treatment.16 Despite many limitations, this method of evaluation remains critical for the intuitive verification of a nation’s competency for treating traumatic injuries. The preventable trauma death rate (PTDR), which is derived from the method mentioned above, is defined as the ratio of patients who have died from injuries they could have survived had they received appropriate treatment after being quickly transported to a suitable hospital within an acceptable time frame.7 In Korea, PTDR has been recorded periodically, starting from the late 1990s. Korea’s PTDR, which was alarmingly high at 40.5% when first measured in 1997, started to decrease with the establishment of the national trauma treatment system (e.g. establishment of the first regional trauma center [RTC] in 2012).891011 PTDR had decreased significantly to 30.5% in 2015, and was reportedly 19.9% in the 2017 mortality statistics: this was the lowest reported value compared to previous studies conducted in Korea.121314 The current study was conducted as a follow-up study of the national survey of trauma deaths, with the goal of establishing a reliable metric for preventable death rates based on the 2019 trauma mortality statistics, and securing foundational data that could be used to design enhancements for the quality management of trauma treatment, by analyzing issues related to preventable death rates.
METHODS
Study population
The current study was conducted using data from patients who had died from traumatic injuries after visiting emergency centers between January 1, 2019 and December 31, 2019. The definition of trauma patients was the presence of one or more S or T codes according to the seventh edition of the Korean Standard Classification of Diseases.15 However, cases were excluded if the only trauma-related code was due to nonspecific influence of external factors (e.g. frostbite, poisoning, intoxication, drowning, first-degree burns, and others) or complications related to surgery and other medical reasons. As of December 31, 2019, 8,482 trauma-related deaths occurred in 363 of 402 emergency medicine institutions throughout Korea. Among these deaths, 1,675 patients had died on arrival (DOA) in the first facility, 508 patients died in the emergency department (ED) in the first facility, 4,067 patients died after hospital admission in the first facility, and 2,232 patients died after transfer to a second facility.
Sampling
The Korean National Emergency Department Information System (NEDIS)16 was used as a sampling framework for the mortality statistics of trauma patients. The NEDIS is a national database that includes clinical and administrative data of all patients who visit the ED. To create an unbiased sample that reflects the population characteristics, a stratified two-stage cluster sampling method was used, with a double layer design for stratification. The variables used for the first stratification were region (Seoul, Gyeonggi/Incheon, Daejeon/Sejong/Chungcheong, Gangwon, Gwangju/Jeolla, Busan/Daegu/Ulsan/Gyeongsang, Jeju), type of hospital (RTC, regional emergency medical center, local emergency medical center, and local emergency medical institution), and number of deaths (≥ 100, 50–99, 30–49, 10–29, and < 10). Then, for the second stratification, the variables of time of death (DOA in the first facility, death in the ED in the first facility, death after hospital admission in the first facility, death after inter-hospital transfer) and patient age (≤ 14 years, 15–54 years, ≥ 55 years) were used. All patients under 14 years of age were included in the sample, even though they could have been excluded due to the small number of deaths. Also, for accurate identification of the process and reasons for death, all patients who died at RTCs and regional emergency medical centers, which are mainly responsible for the treatment of patients with severe trauma, were included in the sample.
Data collection and data type
The patient's medical records were collected from 279 facilities, those that provided treatment for patients who died from trauma and were included in the sample. The corresponding hospitals were asked to provide the necessary medical records in cooperation with the Ministry of Health and Welfare, according to the “Emergency Medical Service Act” and the “Medical Service Act.” Key imaging data were saved in CDs before being mailed. The purpose was to ensure that the copy of the mandatory records included records of the initial visit to the ED, progress notes, nursing care chart, official imaging reading paper, blood test results and discharge records. If additional data was needed during the panel review, the facility was asked for records from hospitals involved in the transfer process; 119 Emergency Medical Service records were also collected.
Multi-staged and multidisciplinary mortality case review
For reviewing medical records, we used a structured review form with an audit filter included (Supplementary Data 1). This form was developed based on the data sheet suggested by the World Health Organization (WHO) guidelines for trauma quality improvement programs.1 Trauma coordinators (total 32), working in RTCs, were tasked with the initial review of mandatory records, after they completed the course of study for investigators working on cases of death, provided by the National Medical Center (NMC). The coordinators organized the information needed by the expert panel to determine the “preventability of trauma death,” such as the general characteristics of the patients, information related to transfer events, and information related to the transfer and treatment of patients. To review and determine death cases, 25 doctors who work at RTCs and specialize in treating trauma patients were selected for the panel. They are case investigation experts currently in charge of independent panel investigations on the preventable trauma deaths in the centers they are currently working at and have all completed the related coursework provided by the NMC. They were divided into five teams, each comprising two general surgeons, one thoraco-vascular surgeon, one neurosurgeon, and one emergency physician. Furthermore, the Trauma Death Review Committee (TDRC), composed of five senior trauma surgeons, developed guidelines for the overall review process and was responsible for educating the other panel members. Multiple workshops were held to introduce the guidelines and instructions for panel screening procedures. Also, when the “preventability” of a trauma death was not determined in the panel discussions at the team level, the TDRC reviewed the case once again to make the final decision. To evaluate the reliability of panel reviews conducted by each team, two teams—arbitrarily determined from the five teams—were to judge a part of the case judged by the other teams: then, the results were compared (Fig. 1).

Judging criteria for the “preventability” of trauma deaths
The basic framework for investigating trauma death cases used the method suggested in the “Guidelines for trauma quality improvement programs,” published by the WHO.1 This standard considers the severity of trauma and the appropriateness of the treatment provided to judge the “preventability” of an individual case of trauma death. Preventable trauma deaths were aggregated to include both “definite preventable (P)” and “potentially preventable (PP)” deaths.
Statistical analysis
The population was estimated with the sample weight values of the sample group. To maintain continuity with existing research, the methods for estimating and adjusting the mortality rate were identical to those used in the previous survey.9 Using multiple logistic regression analysis, risk factors for preventable trauma deaths were identified; variables estimated to have potential influence on the PTDR were used as explanatory variables. The variables included in the logistic regression model were the following: age, hospital type, transfer between hospitals, time from accident to death, time from accident to hospital arrival, and mechanism of injury. Rather than the estimated population, the actual number of deaths was used to analyze the risk factors. Additionally, Cohen’s Kappa coefficient was used to analyze the conformity rate between the judgments of panels, establishing the reliability of the results.
RESULTS
General characteristics of the patients included in the study
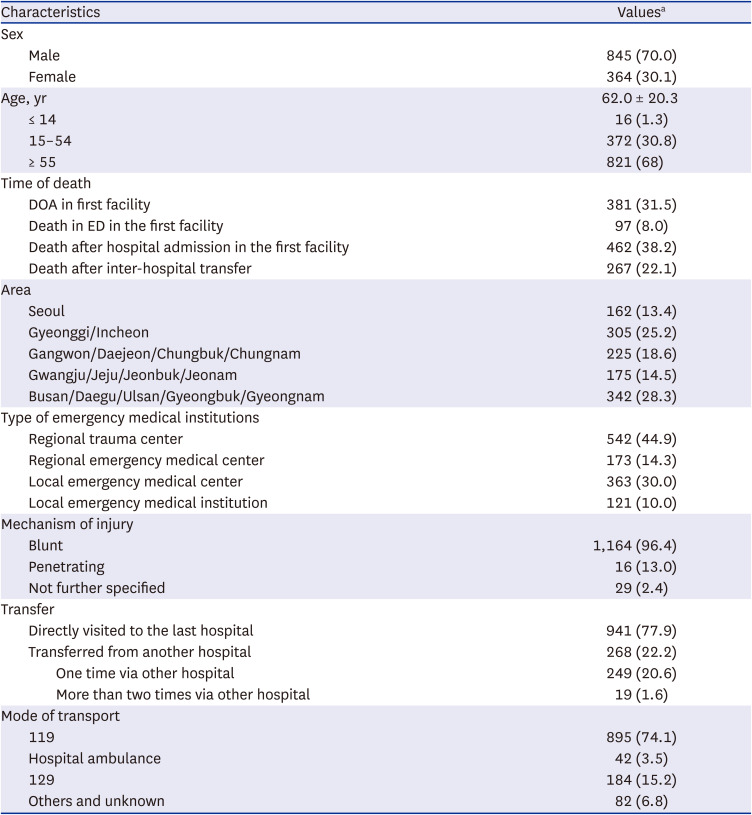
Of the 279 medical facilities extracted from the sample, 243 (87.1%) facilities provided data for 1,460 (86.3%) of the 1,692 cases in the study, all included in the case review. By region, 43 hospitals in Seoul (261 deaths), 64 in Gyeonggi/Incheon (431 deaths), 49 in Gangwon/Daejeon/Chungcheong (309 deaths), 52 in Gwangju/Jeolla/Jeju (243 deaths), and 71 in Busan/Daegu/Ulsan/Gyeongsang (448 deaths) were included in the sample (Table 1). Among these, 397 cases were excluded for being unrelated to trauma, four for the patients still alive, and 57 cases for lacking the minimum information required for judgment. Finally, the “preventability” could be judged for 1,002 cases. For all the cases judged, the raking ratio method was applied to calculate the final weight, which amounted to 1,208 cases (Fig. 2). Their average age was 62.0 years (standard deviation, 20.3 years), of whom 845 (70.0%) were men, with most of the injury mechanisms being blunt injury (96.4%). The number of patients who died at RTC was almost half (542 cases, 44.9%) of the total, the largest inclusion. The number of cases with at least one transfer was 268 (22.2%). Regarding the mode of transport, most used the 119 ambulances (895 cases, 74.1%) (Table 2).
Table 1
Distribution of the sample facilities and trauma deaths according to regions and types of facilities

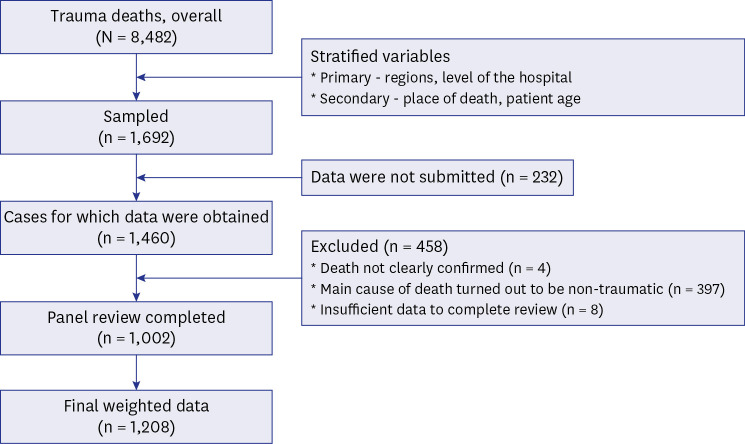
Table 2
Baseline characteristics of the study participants (N = 1,208)
PTDR and related factors
Korea's PTDR, derived from the review of the 2019 trauma mortality statistics, was 15.7%: From this value, 3.1% were P, and 12.7% were PP (Table 3). Cohen’s Kappa index of inter-rater reliability between raters, conducted with a convenience sample of 56 cases, had a value of 0.4, placing it in the moderate category. Factors such as age, time of death, type of emergency medical facility, whether the patient was transferred or not, method of transportation to the medical facility, and time from accident to death showed statistically significant differences between the univariate groups of preventable (P + PP) and non-preventable deaths (non-preventable [NP] + non-preventable, but with care that could have been improved [NPCI]) (Table 4).
Table 3
Preventable trauma death rate (N = 1,208)
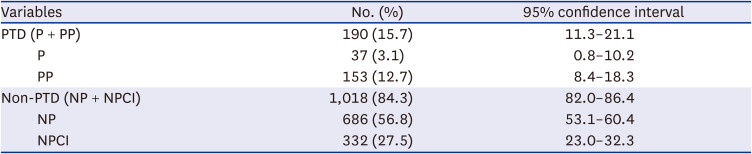
Table 4
Factors associated with preventable trauma death (N = 1,208)
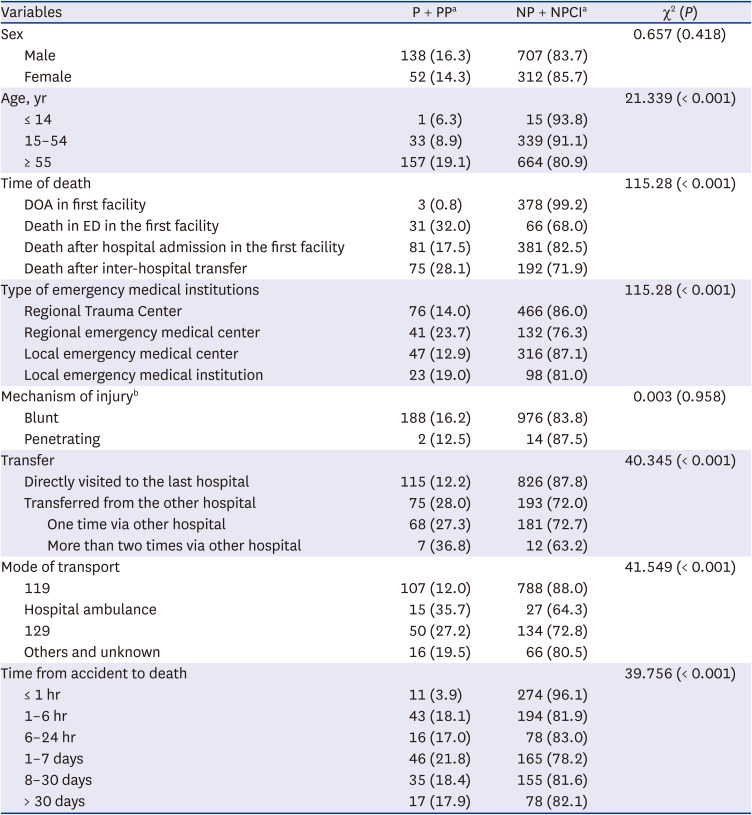
P = preventable, PP = potentially preventable, NP = nonpreventable, NPCI = nonpreventable, but with care that could have been improved, DOA = died on arrival, ED = emergency department.
aAll percentage values were weighted so there may be differences in the sum of each factor; bExcluding “Others/unknown” from the mechanism of injury.
Regression analysis on the judgment of preventable trauma deaths and related factors
The results of the regression model for the prediction of preventable trauma death—made using factors such as age, the type of final emergency medical facility where the death occurred, and the number of transfers between hospitals—indicated that the probability of the prediction of preventable trauma death was higher in cases “once through another hospital” compared to cases “directly visited the last hospital” with statistical significance, with an odds ratio of 2.56. The cases of “More than twice through another hospital” also had statistically higher probabilities of being judged as preventable trauma deaths, with a probability ratio of 3.72. In a model using the variable “time from accident to death” instead of the variable “inter-hospital transfer,” time to death was correlated with the judgment of preventable trauma deaths. Compared to the group where death occurred within one hour of the accident, all groups where death occurred one or more hours after the accident had a higher probability being judged as preventable trauma deaths, with statistical significance (Table 5).
Table 5
Factors related to preventability analyzed by logistic regression (N = 1,208)
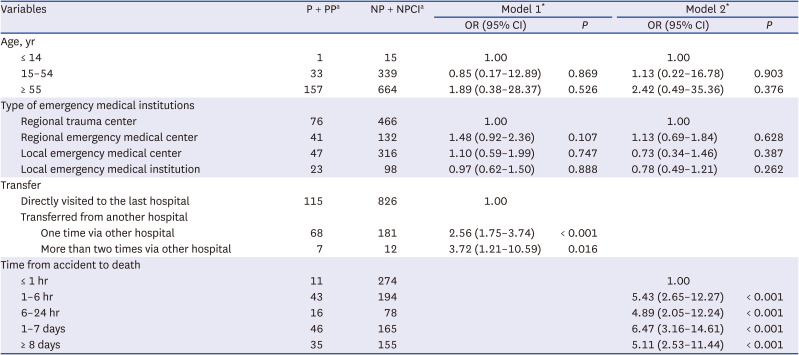
P = preventable, PP = potentially preventable, NP = nonpreventable, NPCI = nonpreventable, but with care that could have been improved, OR = odds ratio, CI = confidence interval.
aAll percentage values were weighted so there may be differences in the sum of each factor.
*For goodness of fit, we conducted the Hosmer-Lemeshow test, and the P values for model 1 and model 2 were 0.692 and 0.166, respectively.
DISCUSSION
PTDR is a fundamental metric for the intuitive evaluation of trauma treatment competency for a nation or region. Unlike Korea, which has not yet completed its system for the systematic treatment of trauma patients, nations with leading competencies in trauma treatment (e.g. the United States and Canada) have an established regional trauma system that is centered around designated trauma centers, with reported PTDR of approximately 5% since the early 2000s.1718 A 2016 report from the U.S. National Academies of Sciences, Engineering, and Medicine recommends a number of measures to improve the quality of trauma treatment, demanding the goal of 0% PTDR.19 Korea, as a realistic goal, aimed to reach 15% PTDR by 2021. For this, massive financial resources have been invested to establish RTCs in 15 cities and provinces around the country to initiate the establishment of a trauma system. The national PTDR is regularly evaluated to review the results of said efforts. The current study is a national follow-up study conducted at the request of the Ministry of Health and Welfare, 2 years after the last investigation conducted using 2017 mortality statistics.
The final PTDR derived from the current study using mortality statistics for 2019 was 15.7%. Here, the definitive PTDR was 3.1%, which is 3.0%p lower than 6.1% from the 2017 survey of trauma death cases, and the PP death rate was 12.7%, which is 1.1%p lower than 13.8% of the preceding study. Consequently, the final PTDR has decreased by 4.2%p compared to the previous study. This result indicates that Korea’s PTDR has been continuously decreasing over the past 20 years. Such improvements in PTDR can be hypothesized to result from the establishment of four new RTCs since the previous study. During the investigation period, there was an increase of 253 beds including 80 sickbeds in the intensive care units exclusively for trauma patients, indicating an increase in national capacity to provide final treatment to patients with severe trauma. Previous research supports such improvements in trauma treatment outcomes because of an increased demand factor of trauma patients in RTCs, which was possible through establishments of additional RTCs and enhanced patient categorization capabilities before arriving at the hospital.12
The results of the current study suggest that the possibility of preventable trauma death increases in the case of a patient transfer, with the risk increasing with each additional transfer. This is because transfers between hospitals delay the time of critical treatment. This has been commonly noted in numerous studies on PTDR.202122 In a study on patients who died in trauma centers, Bratton et al.23 reported unexpected deaths as being more common and the time spent in the intensive care unit as being longer when comparing patients who had been transferred to the hospital with patients who had arrived directly at the trauma centers. Similar results were reported in a study conducted in Korea based on the 2015 mortality statistics, with a strong correlation between patient transfers and preventable trauma deaths, specifically for patients with two or more transfers who had a 2.99 times higher risk of preventable trauma deaths.9 While it is important to improve the quality of care at the hospital level to improve the prognosis of trauma patients,24 it is as important to select an initial hospital on the field that can provide the final treatment for patients with severe trauma to prevent unnecessary transfers.
There were no statistical differences between the judgment of preventable trauma death of patients who died in RTCs and patients who died in other emergency medical facilities. As the index simply investigates the type of final institution where deaths have occurred, this result cannot be interpreted to mean there are no differences between the trauma treatment capabilities of RTCs and other emergency medical facilities. Often patients who died at RTCs, the decisive error occurred in the “previous hospital arrival” or “transfer between hospitals” stages. Kwon et al.25 reported in 2019 that the ratio of patients dying from decisive errors committed during treatment in RTCs was 10.3% among all cases of preventable trauma deaths, with the other 89.7% caused by errors committed in the “premium to arrival at hospital” and “transfer between hospitals” stages, and “at an emergency medical facility other than RTCs.” These results provide evidence supporting the distinct differences between the trauma treatment capabilities of RTCs and those of other emergency medical facilities. Our results should also identify the stages where errors occurred, by conducting additional research that includes the qualitative analysis of trauma death cases.
The time from accident to death had an influence on the preventable trauma-to-death judgment. All groups where death had occurred 1 or more hours after the accident had a higher probability of receiving the preventable trauma death judgment, with statistical significance. Compared to the group where the death occurred within one hour of the accident, the groups where the death occurred after six hours, 24 hours, seven days and more than seven days had almost five times the likelihood of receiving the preventable trauma death judgment. This is because deaths within one hour of trauma are likely caused by severe trauma that has no possible means of treatment. However, since autopsy is rarely performed in Korea, patients who died before arrival at hospitals might have been excluded from the study due to the lack of the minimum information required to determine the preventability of death or due to having received inaccurate judgments.2627 The current study evaluates patient care prior to arrival at the hospital and did not exclude patients who died before arrival at the hospital, to maintain continuity with previous research. To evaluate the quality of trauma patient care before arrival at the hospital, it is necessary to universally perform at least the minimum investigations required to accurately determine the cause of death of trauma patients suffering early deaths, such as autopsies or post-mortem imaging.
This study has some limitations. First, the retrospective study design precluded the analysis of unrecorded factors or missing values. Especially we could not adjust injury severity appropriately due to the limited quality of information and data collected retrospectively for trauma death cases. Second, the evaluation of “preventability” relied entirely on the analysis by expert panels, which has limitations in objective reproducibility, although the Cohen’s Kappa index indicated fair reliability similar to that in previous studies. Third, although the final results were supplemented to some extent by statistical analysis methodology, the data collection rate was lower than in previous studies. In a previous survey on 2017 trauma deaths, 117 of 118 institutions (99.2%) submitted medical records, whereas in this survey, only 243 of 279 institutions (87.1%) submitted medical records. One of the reasons was the lower compliance of emergency medical institutions to the data collection than in previous surveys. This may have been partially due to the coronavirus disease 2019 pandemic. Finally, this study only analyzed changes in the PTDR and the correlation between some variables and their preventability but did not determine the reason for the improvement in the PTDR. Further studies comparing the results of this study with those of previous studies may help to identify additional reasons for the decrease in the PTDR.
The current study is a follow-up of the national PTDR survey, conducted once every two years at the request of the Ministry of Health and Welfare. In 2019, the PTDR for deceased patients was 15.7%, which is 4.2%p less than that reported in the preceding survey. The risk of preventable trauma death judgment increased with the occurrence of inter-hospital transfers or increased time from accident to death. To achieve additional decreases in PTDR, there needs to be greater focus on patient transfers to RTCs, and post-mortem testing of deceased patients prior to hospital arrival should be performed more frequently for a detailed quality assessment of pre-hospital trauma care.
 XML Download
XML Download