

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The worldwide spread of coronavirus disease 2019 (COVID-19) still poses enormous problems. Though vaccination rates increase progressively, it does not mean complete control of the disease, and an effective cure does not seem close. The successive advents of variants such as delta and omicron result in new challenges. The South Korean government has, thus far, successfully prevented, detected, and responded to the threat of COVID-19.12 However, when we raise a simple question as to what discharged COVID-19 patients experience types of medical and social problems, not much has been discussed among medical experts and policymakers.
The shift to “Living with Corona” policy assumes high vaccination rates, effective treatment of infected patients with enough hospital beds, and proper social policies to help the infected and the discharged. It allows the increase in infection rate to a certain extent in exchange for restoring everyday life. However, there remains an unseen risk behind this policy: the COVID-19 sequelae. We do not know about the COVID-19 sequelae and its recovery cost. Therefore, the most needed information for social policy against COVID-19 is 1) what kind of repercussions the recovered encounter and 2) what kind of social support is required. This knowledge is more pertinent when we think of the future with COVID-19 being a constant threat, because going back to normalcy presupposes adequate policies with proper medical and social service delivery systems for care of infected and recovered patients. However, little information about the COVID-19 sequelae is available even two years post outbreak.
Literature on discharged COVID-19 patients can be categorized into two parts: 1) studies investigating types of residual symptoms former patients’ experience, and 2) endeavors to identify the social needs of the recovered. According to the first line of research, respiratory distress is the most frequently mentioned symptom of the recovered. Though there is a lack of comprehensive research tracing the sequela, several research studies following patients for 100 days or more after discharge found respiratory distress to be the most common symptom.34567 Other frequently reported symptoms include anxiety and fatigue (https://www.cdc.gov/coronavirus/2019-ncov/long-term-effects.html), both a physical response to COVID-19 virus infection and a psychological burden. For example, the study by Wang et al.8 dealing with mental burden of patients because of COVID-19 related hospitalization, reported that 57% of patients had mental difficulties, including post-traumatic stress disorder, and 42% of people who did not have psychological problems before and 78% who did have cognitive problems before declared that they had new psychosomatic complications. In the Korean scenario, a study by Park et al.9 shows that half of the patients they observed experience depression, which supports the hypothesis that people suffer from psychological and physical burdens post recuperation. While some studies have investigated meaningful variables that influence residual symptoms, the results have not pinpointed underlying factors effectively. Although previous studies hypothesized that age might significantly impact post-discharge symptoms, they have not discovered a consistent pattern for it or for demographic variables.410
Few studies have investigated social needs of recovered patients, because we are still in the middle of the widespread COVID-19 infection. Even fewer studies have explored long-term needs of patients since the demand for the study of short-term needs is much greater. Yet, some scholars have reported the needs of recovered patients with respect to various aspects of life. First, Chopra et al.11 investigated multidimensional needs of 488 discharged patients in the state of Michigan, USA and reported that 60% (117/195) did return to work, but 30 of them had to reduce work hours or be transferred to other duties due to health difficulties. Further, they found that almost half of the respondents were going through psychological troubles, with 28 using counselling, psychological support services and other social services. Finally, their findings from personal finance-related questions showed that while 179 of the respondents were experiencing more than moderate levels of financial distress, 47 had to spend all or almost all of their savings, and 35 had to reduce their expenditure on essentials. Second, Qu et al.12 followed 581 patients after discharge for three months and found that they experienced reduced health-related quality of life and had physical problems. Finally, a study focusing on the recovered patients’ psychological conditions also reported that most patients need emotional support from their families and neighbors.9
One of the crucial implications from this review is that the recovered patients of COVID-19 face mental and physical challenges. However, whether the psychological troubles originate from the infection or the isolation period is unclear. The policy implication is the same: appropriate policy measures should include physical and psychological intervention and support. Regrettably, empirical evidence is not strong enough to appraise COVID-19 sequelae and patients’ social service needs. Hence, it is necessary to have a more comprehensive investigation of the after-discharge experience of COVID-19 patients. The following analysis addresses this requirement.
METHODS
Study design and participants
This paper employs a two-stage research design: in-patient stage and discharged stage. First, we enrolled patients diagnosed as COVID-19 positive and hospitalized in the National Medical Center (NMC) in Seoul, Korea, between May and July 2021. The four criteria used for sample selection were: 1) diagnosed COVID-19, 2) over 19 years old, 3) without HIV or malignancy, and 4) without dementia due to the limitation of a telephone interview. All patients admitted to NMC for COVID-19 were screened and asked if they agreed to enroll in this study. Initially, 94 patients were enrolled and interviewed about their symptoms and subjective health and living conditions; each patient’s medical records and treatments were reviewed. The patients were discharged when their clinical symptoms improved and fever resolved without antipyretics at least 10 days after admission. All patients were interviewed over telephone 12 weeks after discharge.
Data collection and outcomes
We collected information on their persistent symptoms, subjective health condition, and quality-of-life-related changes or need for care services in person at admission and on the telephone after 12 weeks from discharge. The structured questionnaire for the interview included clinical systemic symptoms (headache, fatigue, muscle pain, joint pain, nausea and/or vomiting, diarrhea), need for medical treatment (including the visit of clinics or emergency rooms), unemployment, or need for care from others. We also measured their degree of clinical frailty. The Clinical frailty scale (CFS) was introduced to summarize the overall fitness level. According to CFS, CFS 1 means very fit, CFS 2 well, CFS 3 managing well, CFS 4 living with very mild frailty, CFS 5 living with very frailty, CFS 6 living with moderate frailty, CFS 7 living with severe frailty, CFS 8 living with very severe frailty and CFS 9 terminally ill.14 And the CFS significantly increases with COVID-19.15 The patients were asked to describe their subjective health status using EuroQol visual analogue scale (EQ-VAS, best imaginable health-worst imaginable health, 100–0). Eastern Cooperative Oncology Group (ECOG) performance status was used to describe their performance status (0–5, fully active-dead).
Statistical analysis
Statistical analyses were conducted using R 4.0.13 Descriptive statistics were performed for the collected data. The logistic regression is used to explain the change in QoL-related measures. Besides, the paired t-test are used to compare before and after discharge conditions.
RESULTS
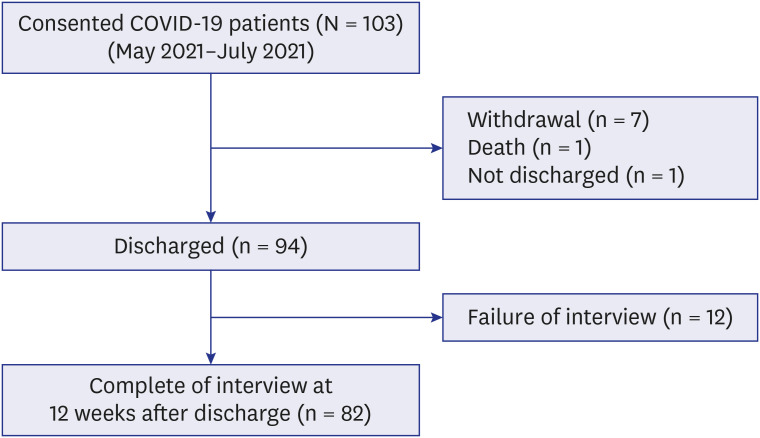
During the study period, 103 patients aged 19 years and older were enrolled. Seven patients withdrew their consent, one patient expired during hospitalization, and one was not discharged by the end of our research. We conducted telephone interview 12 weeks after discharge and completed 82 interviews of the 94 attempted (Fig. 1).
Fig. 1
Flow chart. Consecutive 82 COVID-19 patients who completed the interview at 12 weeks after discharge.
COVID-19 = coronavirus disease 2019.
Demographics
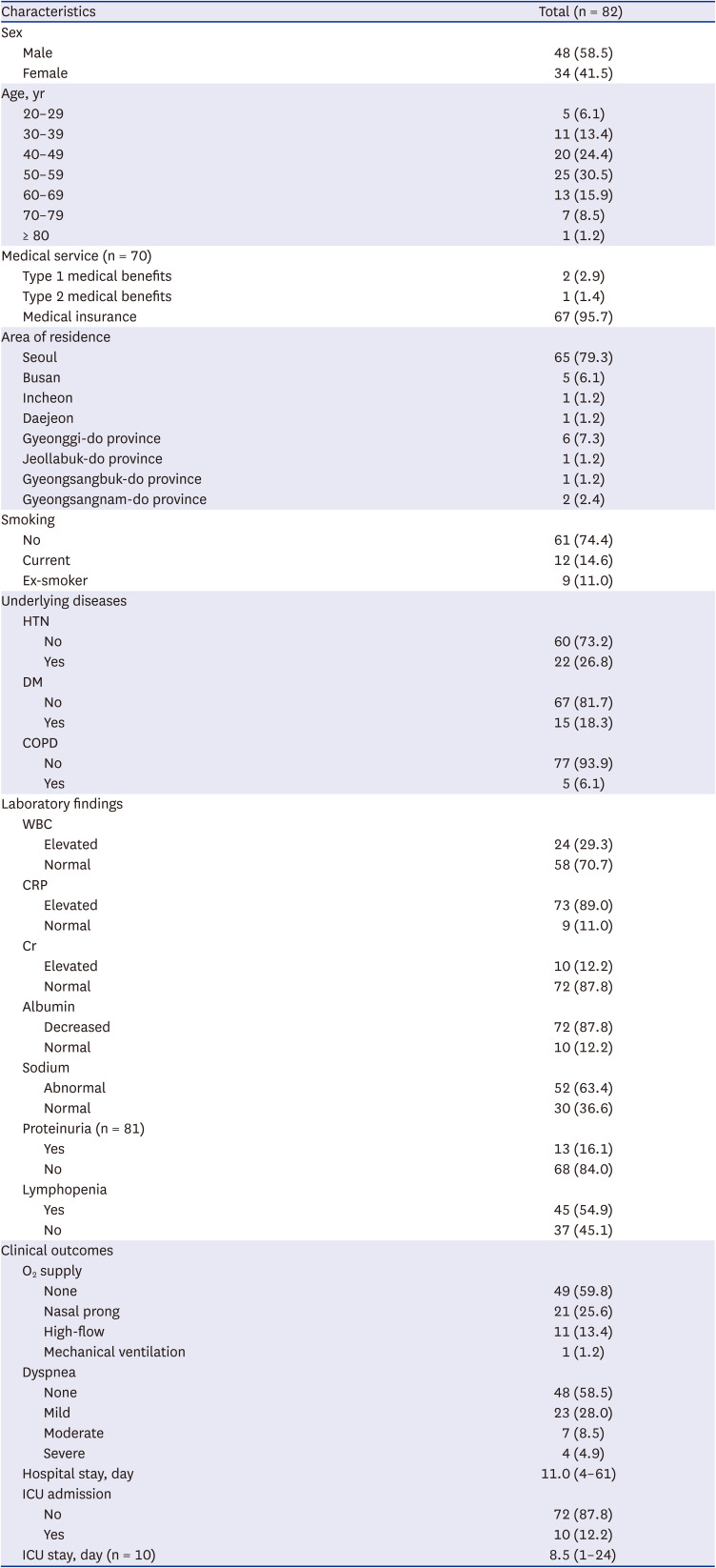
The final analysis included 82 patients, and their baseline demographic information is shown in Table 1. The median age was 52 years (range: 23–84 years). Of the participants, 48 (58.5%) were male and 34 (41.5%) were female. Sixty-seven had medical insurance and two were recipients of type 1 medical benefits and one received type 2 medical benefits.
Table 1
Baseline demographics and clinical characteristics, including medical records and symptoms at admission
Clinical characteristics including medical records and symptoms
The median height was 166.50 (157–176) cm, and the median body weight was 70.00 (54.4–85.6) kg. The rate of patients who had hypertension (HTN), diabetes mellitus (DM), and chronic obstructive pulmonary disease (COPD) as medical history was 26.8%, 18.3%, and 6.1%, respectively and 50 (61.0%) showed no underlying disease (HTN, DM, and COPD). The median length of hospital stay was 11.00 (4–61) days, with 10 (12.2%) patients in intensive care unit (ICU). The median length of ICU stay was 8.50 (1–24) days. Thirty-three patients (40.2%) required oxygen therapy, and all reported shortness of breath at admission (Table 1).
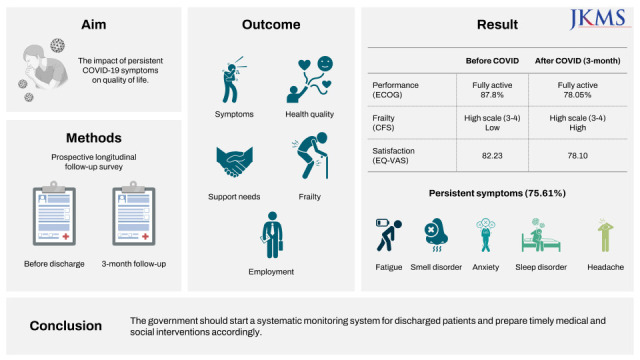
Change of performance, CFS, and EQ-VAS
Fully active status reduced from 87.8% before admission to 78.1% at 12 weeks post discharge. Two patients (2.4%) were ambulatory and capable of all self-care after discharge but were unable to carry out any work activities at 12 weeks after discharge. CFS levels 1, 2, 3 and 4 changed from 31 (37.8%), 40 (48.8%), 8 (9.8%) and 3 (3.7%) at admission to 22 (26.8%), 31 (37.8%), 24 (29.3%), and 5 (6.1%) at 12 weeks after discharge, respectively. Just after admission, the median EQ-VAS was 82.23 (67.85–96.61), and it decreased to 78.10 (62.08–94.12) at 12 weeks after discharge. The reduction rate of EQ-VAS was 4.13. The decrease was more remarkable in females (71.62 [56.21–87.03] from 80.38 [64.01–96.75]) than in males (82.69 [67.73–97.65] from 83.54 [70.74–96.34]) (Table 2).
Table 2
Change of ECOG, CFS, EQ-VAS, need for care and employment (n = 82)
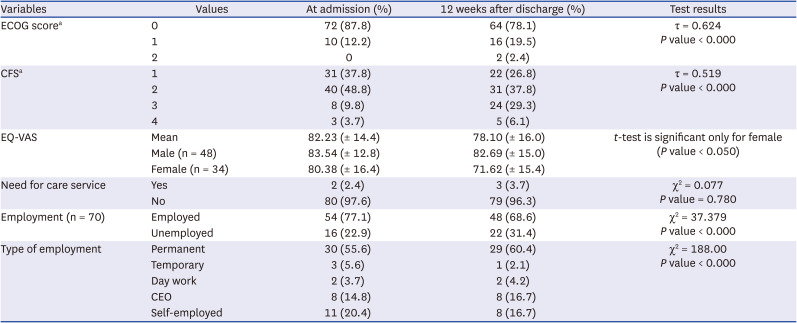
ECOG 0: fully active, ECOG 1: restricted in physically activity strenuous but ambulatory and able to carry out work of a light or sedentary nature, ECOG 2: ambulatory and capable of all self-care but unable to carry out any work activities, ECOG 3: capable of only limited self-care, ECOG 4: completely disabled, CFS 1: very fit, CFS 2: well, CFS 3: managing well, CFS 4: living with very mild frailty, CFS 5: living with very frailty, CFS 6: living with moderate frailty, CFS 7: living with severe frailty, CFS 8: living with very severe frailty, CFS 9: terminally ill, EQ-VAS: the patient's self-rated health on a vertical visual analogue scale, where the endpoints are labeled ‘the best health you can imagine’ and ‘the worst health you can imagine.’
ECOG = eastern cooperative oncology group, CFS = clinical frailty scale, EQ-VAS = EuroQol visual analogue scale.
aKendall’s rank correlation test is conducted.
Need for care services
Before admission, two patients (2.4%) needed help from others. At 12 weeks after discharge, one more patient needed help from others (Table 2). This implies that change of care services was insignificant.
Change in employment
Of the 54 (77.1%) patients who were employed before admission, six lost their jobs after discharge (Table 2). One had a permanent job, while two had temporary employment. The most vulnerable job type was the self-employed category, with three patients not working at 12 weeks post discharge. In general, permanent job workers have more time for rehabilitation; however, self-employed patients are concerned about decreased income and more possibility of psychological distress as a persistent symptom.
Persistent symptom at 12 weeks after discharge
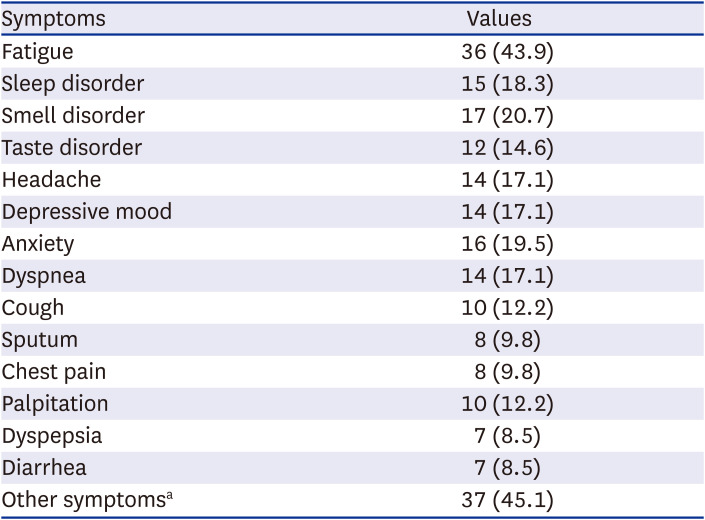
Sixty-two (75.6%) patients reported at least one symptom at 12 weeks after discharge (Table 3). The most frequently reported symptom was fatigue (43.9%) followed by smell disorder (20.7%), anxiety (19.5%), sleep disorder (18.3%), headache, depressive mood, dyspnea (17.1%) and taste disorder (14.6%).
Table 3
Persistent symptoms at 12 weeks after discharge (n = 82)
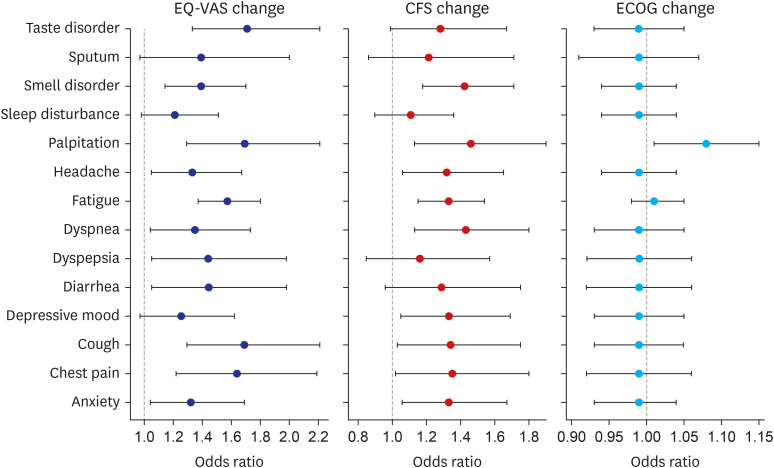
We performed a simple logistic regression analysis for the change in QoL-related measures (ECOG, EQ-VAS, CFS) using the severity of each sequela as predictor (Fig. 2). Due to the limited information, the measures were recoded as a binary variable, with 1 representing “QoL getting worse” and 0 “getting better.” Though a causal relationship cannot be inferred, the result can indicate the direction of covariation. Eleven out of 14 sequelae had a negative relationship with EQ-VAS change, nine sequelae appeared significant for CFS change, and only palpitation had a significant relationship with ECOG change. In summary, only palpitation had a significant influence for the three measures.
Change of receiving medical services
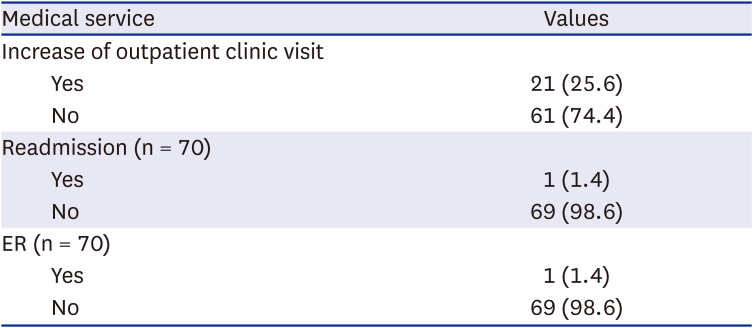
Compared with regular outpatient clinic visits before admission, 21 patients (25.6%) reported an increased number of outpatient clinic visits due to any reason including symptom related with long COVID-19 or aggravation of combined medical disease. Among 70 patients, one patient (1.4%) reported readmission, and one patient (1.4%) reported an ER visit (Table 4).
DISCUSSION
To identify COVID-19 patients’ needs after hospital discharge, we followed 82 COVID-19 patients after 12 weeks of discharge and analyzed the responses. Given that the sequelae of COVID-19 are mentioned frequently without a solid empirical basis in Korea thus far, our analysis results can be extensively utilized in policy discussion.
The results from the survey based on the subjective quality of life (EQ-VAS), CFS score, and ECOG performance status scale show consistent downward trends after 12 weeks from discharge. The decrease is more evident in females, which is consistent with the previous finding that females encounter considerably higher reduction in life satisfaction.14 Second, in case of residual symptoms, patients go through widely-reported troubles such as fatigue and diverse physical problems such as loss of taste and psychological conditions like depression.
On analyzing the relationship between life satisfaction/frailty score/ECOG scale and the sequelae, we found that various symptoms have a statistically significant impact on worsening life satisfaction, frailty score, and ECOG performance status. This suggests that without proper intervention post-discharge, COVID-19 patients will experience a drop in quality of life. Finally, the patients’ economic status after discharge should be a point of concern because COVID-19 infection and treatment will persistently lower their quality of life due to financial stress. Our survey found that some did show interest in contractual labor market participation, which could be a critical point for discharged COVID-19 patients.
The results demonstrate that the discharged COVID-19 patients have medical and social service needs. As of the point of writing this paper (February 2022), the Korean government has not released any systematic analysis of COVID-19 sequelae and their predicaments. Our analysis suggests that medical experts and the community should address more policy-related agenda on the patients’ experience after discharge, especially physical and psychological difficulties. COVID-19 patients suffer more from decreasing quality of life due to mental stress than physical symptoms, which implies that COVID-19 patients after discharge require appropriate social services in addition to medical interventions to bring them back to the normalcy they enjoyed before. The limitation of our research is that our study is based on the survey with small samples. However, as the Korean government announced that it will open medical service data of the discharged COVID-19 patients on 31 March 2022, our findings needs to be validated by the larger sample. At the same time, as our research was done before the prevalence of omicron variant, we need to examine how different variants cause different sequalae in future studies.
 XML Download
XML Download