

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Steatosis is a common manifestation of various liver diseases. Among them, non-alcoholic fatty liver disease (NAFLD) is an emerging public health issue, and it has been reported in approximately 25% of the general population. NAFLD has a wide spectrum, ranging from asymptomatic to inflammation with or without fibrosis.1234 Recent studies have reported that superimposed liver steatosis is associated with a higher risk of liver cirrhosis or hepatocellular carcinoma.56 Therefore, detection and quantification of liver steatosis in patients with suspected NAFLD is important to determine prognosis and guide treatment decisions.
A percutaneous liver parenchymal biopsy is the gold standard method for staging steatosis and fibrosis; however, it has several disadvantages, including invasiveness, risk of bleeding, and risk of sampling error due to the heterogeneity of the disease distribution.789 Various non-invasive quantitative methods, including ultrasound and magnetic resonance imaging (MRI), have been developed and used to address the limitations of liver parenchymal biopsies. In particular, the magnetic resonance (MR)-proton density fat fraction (PDFF) is considered a non-invasive reference standard for assessing liver fat content.4101112 However, conventional post-processing MR-PDFF methods are limited by the use of mean signal intensity values by drawing the region of interest (ROI).1314
Radiomics enables the analysis of images beyond visual inspection by extracting dozens to hundreds of quantitative features.15 The application of radiomics in liver disease has focused on the prediction and differentiation of various tumors or fibrosis assessment1617; however, radiomic analysis of hepatic steatosis using MR-PDFF in patients with NAFLD has not yet been conducted. Therefore, we hypothesized that radiomic features extracted from MR-PDFF images would allow a more accurate assessment of hepatic steatosis than conventional ROI methods or the use of clinical data. Consequently, we investigated the diagnostic performance of several modalities including MR-PDFF radiomics for detection of hepatic steatosis grade ≥ 2 in patients with suspected NAFLD.
Go to : 
METHODS
Study participants
Patients with suspected NAFLD in our institution’s gastroenterology department who underwent MR-PDFF between November 2017 and May 2020 were included in the study. The inclusion criteria were as follows: 1) age ≥ 18 years; 2) suspected hepatic steatosis on ultrasound imaging; and 3) ≤ 60 days between MR-PDFF and liver biopsy. The exclusion criteria were as follows: 1) history of alcohol consumption; ≥ 30 g/day for man and ≥ 20 g/day for woman; 2) history of chronic liver diseases such as chronic viral hepatitis B or C infection, autoimmune hepatitis, and primary sclerosing cholangitis; 3) history of major liver surgery such as liver transplantation and hemihepatectomy; or 4) unavailability of liver biopsy. Fig. 1 shows a flow diagram of the study population and Table 1 shows their demographic and clinical characteristics.
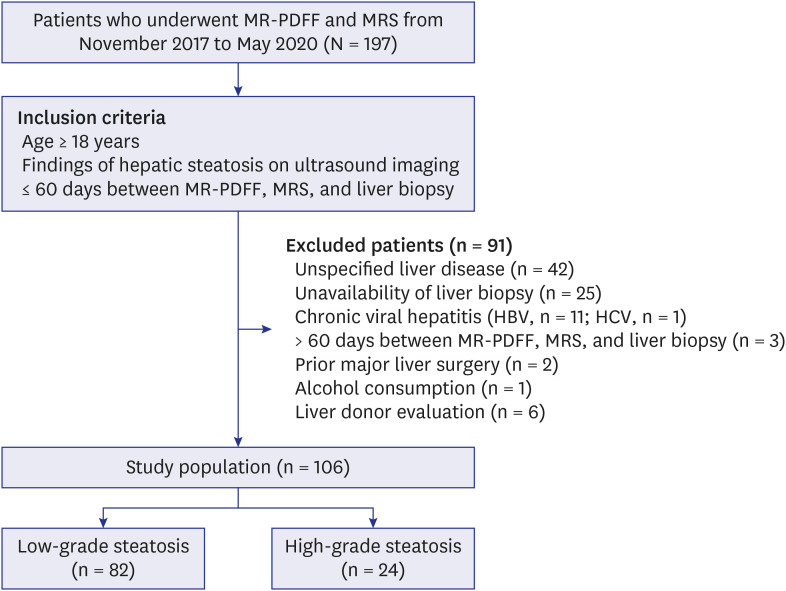 | Fig. 1Flow diagram for the study population.MR-PDFF = magnetic resonance-proton density fat fraction, MRS = magnetic resonance spectroscopy, HBV = hepatitis B virus, HCV = hepatitis C virus.
|
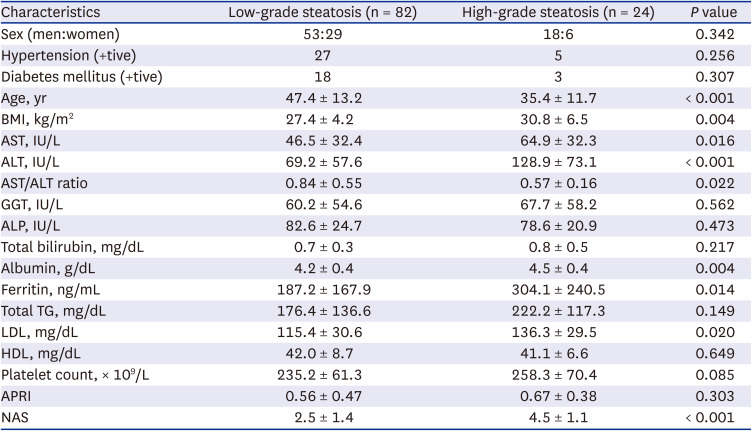
Table 1
Demographic characteristics of patients with suspected non-alcoholic fatty liver disease
BMI = body mass index, AST = aspartate aminotransferase, ALT = alanine aminotransferase, GGT = gamma-glutamyl transferase, ALP = alkaline phosphatase, TG = triglyceride, LDL = low-density lipoprotein, HDL = high-density lipoprotein, APRI = aspartate aminotransferase to platelet ratio index, NAS = non-alcoholic fatty liver disease activity score.
![]()
The clinical features collected from the patients, including age, sex, weight, height, and blood test results (alanine aminotransferase [ALT], aspartate aminotransferase [AST], triglyceride, low-density lipoprotein, and platelet count) obtained within 1 month of MR-PDFF were evaluated. Body mass index and aspartate aminotransferase-to-platelet ratio index were also calculated.
The histopathological grade of hepatic steatosis
Histopathological examination of the liver serves as the gold standard for liver steatosis. One hundred and four patients underwent a percutaneous liver biopsy using an 18-gauge semi-automated biopsy needle with a penetration depth of 20 mm targeting segment 5/6, and two biopsy cores were obtained. The remaining two patients underwent a surgical biopsy during cholecystectomy and donor hemihepatectomy. Histological preparations of liver biopsies were retrospectively reviewed by one pathologist (7 years of experience) blinded to the clinical data and MR-PDFF results. NAFLD activity score was graded according to the criteria of Kleiner et al.8 Liver steatosis was graded according to the percentage of fat within the hepatocytes: grade 0 (healthy, < 5%), grade 1 (mild, 5–33%), grade 2 (moderate, 34–66%), and grade 3 (severe, > 66%).14 The stage of pathological hepatic steatosis was classified as low-grade (grade 0 or grade 1) or high-grade steatosis (grade 2 or grade 3).181920
MRI acquisition
All MRI scans were performed using a 3.0-T system (Magnetom Skyra; Siemens Healthineers, Erlangen, Germany) with a 30-channel body coil. MR-PDFF was performed according to a previously described protocol212223 using commercial hardware and software (Resoundant Inc., Rochester, MN, USA; Syngo MR E11, Siemens Healthineers).13 For PDFF, complex-based chemical shift-encoded water-fat reconstruction techniques were used with six-echo three-dimensional gradient-recalled-echo images, an imaging matrix of 160 × 115, field of view of 380 × 304, and slice thickness of 3 mm without gaps. A low flip angle (4°) was used to minimize the T1 bias between fat and water.1223 A sufficient scan range was used to include all livers. PDFF maps were automatically reconstructed using the vendor’s algorithm with the T2* correction calculated from signal decay and a multipeak fat model.24
Furthermore, the MRS of the liver included in the vendor’s algorithm was performed in the right hepatic lobe randomly by a radiologic technologist from three rectangular ROIs for reference to the MR-PDFF value.
MR image segmentation and analysis processing
Before starting the segmentation process, three radiologists were trained using a software applicator to improve the segmentation accuracy. In addition, all radiologists preliminarily discussed about 15 cases and decided on consensus and optimization of segmentation. Three radiologists were randomly assigned to perform whole-volume segmentation. Segmentation was performed as carefully as possible to exclude the major hepatic and portal veins, hepatic fissures, and gallbladder (Fig. 2). As a result, whole-volume segmentation of fat fraction images of MR-PDFF was completed by three radiologists (two abdominal radiologists with 22 years [n = 21] and 10 years [n = 28] of clinical experience, respectively, and second year resident in radiology [n = 57]) using a commercial program, AVIEW (version 1.0.32.12; Coreline Soft, Seoul, Korea).
 | Fig. 2A 30-year-old woman with non-alcoholic fatty liver disease. The work screen shows the completion of the whole-volume segmentation of the fat fracture image of the magnetic resonance-proton density fat fraction using a commercial program. Vascular structures such as portal veins (asterisk) are excluded and only the liver parenchyma indicated in green is accurately segmented.
|
Eight or nine circular ROIs were evaluated using the fat fraction image of MR-PDFF, which has been shown to correlate accurately with liver histology and MRS.21252627 ROI areas were maintained at approximately 300–350 mm2 and manually drawn while avoiding the edges of the liver and major vessels (Fig. 3).28 All post-processing was performed using a commercial workstation by a gastrointestinal radiologist with 10 years of experience, who was blinded to the clinicopathological data. The liver steatosis values obtained from MR-PDFF were organized using the mean and median values, and the steatosis values were used as radiologic features.
 | Fig. 3A 33-year-old man with non-alcoholic fatty liver disease (hepatic steatosis grade 1 and 20% steatosis on histopathology). The liver steatosis values on the MR-PDFF are measured to be approximately 19.0% (A) and 21.3% (B). The value of liver steatosis on MRS is 19.6% (C, D). The MR-PDFF and MRS values measured at similar locations in segment 4a of the liver are almost identical (A, C).MR-PDFF = magnetic resonance-proton density fat fraction, MRS = magnetic resonance spectroscopy.
|
For the three MRS values obtained during the MRI examination (Fig. 3), the mean value was also used as a radiologic feature.
Radiomic feature extraction
Based on MR-PDFF data with whole-volume segmentation applied, several hundreds of radiomic features were analyzed using PyRadiomics 3.0.1 in Python (version 3.7.4; Python Software Foundation, Wilmington, DE, USA).2930
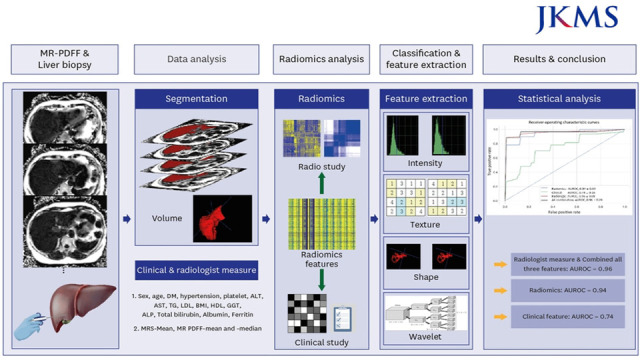
Fig. 4 illustrates the analysis pipeline. The features consisted of 14 shape features (two-dimensional and three-dimensional), 18 first-order features, and 73 texture features from the original image, as well as 144 first-order features (18 × 8) and 584 texture features (73 × 8) from eight types of wavelet-decomposition images, obtained with a high-pass filter (HLL, HLH, HHL, and HHH) and low-pass filter (LLL, LLH, LHL, and LHH). Wavelet-xyz indicates a combination of high-pass (H) and low-pass (L) filters, such as wavelet-low high low (LHL) or wavelet-high high low (HHL).31 Therefore, a total of 833 radiomic features were extracted.
 | Fig. 4Radiomics pipeline.MR-PDFF = magnetic resonance-proton density fat fraction, DM = diabetes mellitus, ALT = alanine aminotransferase, AST = aspartate aminotransferase, TG = triglyceride, LDL = low-density lipoprotein, BMI = body mass index, HDL = high-density lipoprotein, GGT = gamma-glutamyl transferase, ALP = alkaline phosphatase, MRS = magnetic resonance spectroscopy, AUROC = area under the receiver operating characteristic curve.
|
Data analysis
Feature selection and classifier training
Radiomic, radiologic, and clinical features, which are important for grading hepatic steatosis in patients with suspected NAFLD, were selected using a random forest regressor in Python (version 3.6; Python Software Foundation) with the Scikit-learn package (https://github.com/scikit-learn/scikit-learn). Although many quantitative features can be extracted from radiomic, radiologic, and clinical data, they may be highly correlated or simply considered noise. Therefore, 20 repeated 10-fold stratified cross-validation and feature selection using a random forest regressor were performed to avoid overfitting in the limited datasets.32 A random forest classifier model33 was trained to use these important features to classify steatosis grades as binary results. We evaluated the area under the receiver operating characteristic curve (AUROC) and classifier accuracy. The classifier diagnosed steatosis grade based on radiomic, radiologic, or clinical features or a combination of all features. Statistical differences in the AUROC according to each classifier were compared using a machine learning model with the Delong’s test. Statistical significance was defined as a two-tailed P value < 0.05.
Statistical analyses
Demographic and clinical data of patients with suspected NAFLD were compared using the Mann-Whitney U test, paired t-test, χ2 test, and Fisher’s exact test. The intraclass correlation coefficient (ICC) verified the correlation between steatosis measurement methods. ICC values of 0.5–0.75, 0.75–0.9, and > 0.9 were considered moderate, good, and excellent reliability, respectively.34 The steatosis grade correlation between histology and MR-PDFF was evaluated using the weighted kappa test. Weighted-kappa value of < 0.20, 0.21–0.40, 0.41–0.60, 0.61–0.80, and 0.81–1.00 were considered poor, fair, moderate, good, and very good agreement. Statistical analyses were performed with SPSS Statistics 20.0 for Windows (IBM Corp., Armonk, NY, USA) or Medcalc 20.114 for Window (MedCalc Software Ltd., Ostend, Belgium). Statistical significance was defined as a two-tailed P value < 0.05.
Ethics statements
This retrospective study was approved by the Institutional Review Board of the Korea University Medical Center (approval number: 2020AN0387), and informed patient consent for research was waived. All research and data collection procedures adhered to the tenets of the Declaration of Helsinki.
Go to :
RESULTS
Patients’ demographics
The demographic characteristics of patients with suspected NAFLD are presented in Table 1. As mentioned previously, 106 patients were enrolled in this study (Fig. 1). The mean interval between MR-PDFF and liver biopsies was 2.66 (range, 0–53) days. In 92 patients, the interval between MR-PDFF and liver biopsy was < 3 days. Of the 106 patients, 18 were grade 0 (17.0%), 64 were grade 1 (60.4%), 17 were grade 2 (16.0%), and seven were grade 3 (6.6%). Therefore, 82 patients were assigned to the low-grade steatosis group and 24 patients were assigned to the high-grade steatosis group. Only one patient was suspected of iron overload on MRI examination; however, iron overload was not identified in the histopathological review.
Liver steatosis value in MR-PDFF, MRS, and pathology
The liver steatosis values were organized according to the measurement method used for the two patient groups (Table 2). There was a significant difference in liver steatosis values between the two groups (approximately 10.7–12.0% vs. 27.7–28.9%, P < 0.001). Histopathologically, the mean value of the low-grade steatosis group was 17.3%, and that of the high-grade steatosis group was 55.2%, and there was a statistically significant difference (Table 2, P < 0.001).
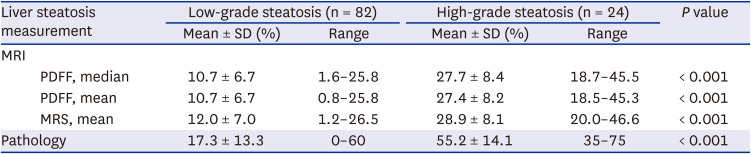
Table 2
Value of liver steatosis in MR-PDFF, MRS, and pathology in patients with suspected non-alcoholic fatty liver disease
MR = magnetic resonance, MRI = magnetic resonance imaging, PDFF = proton density fat fraction, MRS = magnetic resonance spectroscopy, SD = standard deviation.
![]()
The agreement between the MR-PDFF and the MRS showed excellent reliability (ICC, 0.980–0.998; P < 0.001) (Table 3). However, the agreement between MRI measurements and pathology showed moderate reliability (ICC, 0.720–0.740; P < 0.001) (Table 3). The agreement between histologic steatosis grade and MR-PDFF steatosis grade according to Caussy et al.14 showed very good agreement (weighted-kappa value = 0.873, 95% confidence interval, 0.800–0.946).
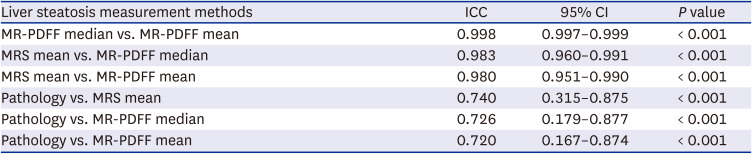
Table 3
The ICC between the liver steatosis measurement methods
MR-PDFF = magnetic resonance-proton density fat fraction, MRS = magnetic resonance spectroscopy, ICC = intraclass correlation coefficient, CI = confidence interval.
![]()
Feature selection and diagnostic performance of liver steatosis classifiers using machine learning
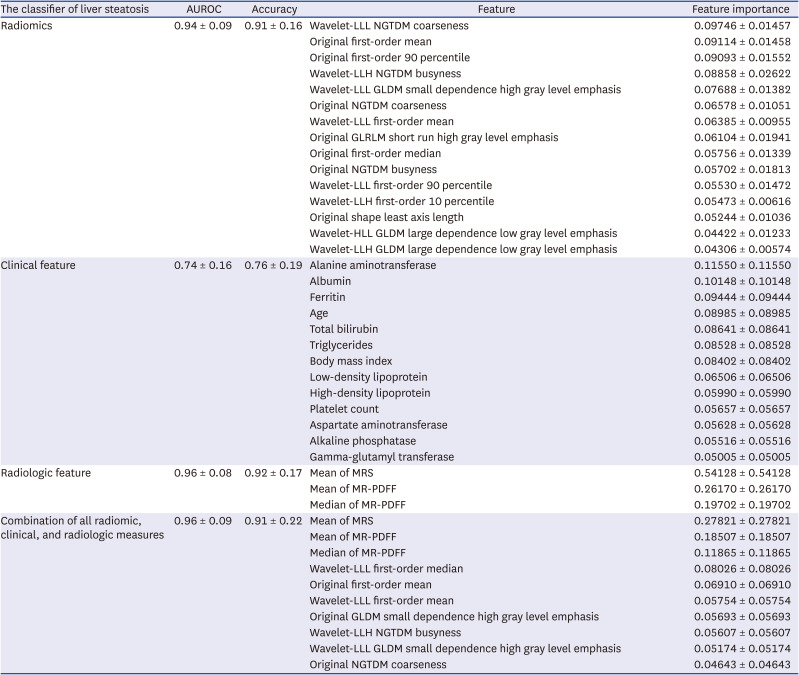
Among the hundreds of variable radiomic features, important feature selection was performed using 20 repeated 10-fold stratified cross-validations and a random forest regressor. The important features extracted by each method and the diagnostic performance of the liver steatosis classifier are presented in Table 4 and Fig. 5.
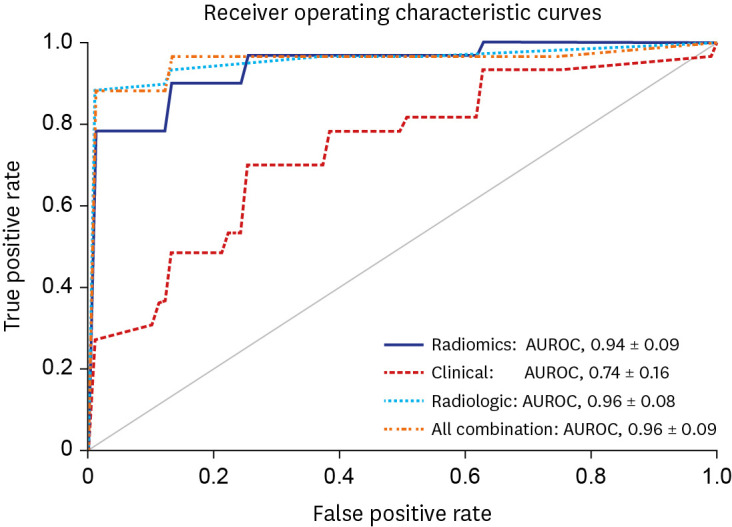 | Fig. 5Receiver operating characteristic curve for prediction of the grade of liver steatosis.AUROC = area under the receiver operating characteristic curve.
|
Table 4
Diagnostic performances of liver steatosis classifiers and several important features of each classifier
Wavelet-xyz indicates a combination of high-pass (H) and low-pass (L) filters, such as wavelet-low high low (LHL) or wavelet-high high low (HHL).
AUROC = area under the receiver operating characteristic curve, NGTDM = neighboring gray tone difference matrix, GLDM = gray level dependence matrix, GLRLM = gray level run length matrix, MRS = magnetic resonance spectroscopy, MR-PDFF = magnetic resonance-proton density fat fraction.
![]()
Radiomics classifier
A total of 15 radiomic features were extracted (wavelet-LLL neighboring gray tone difference matrix (NGTDM) coarseness, original first-order mean, and original first-order 90 percentile), which were determined to be the three most important features. The AUROC and accuracy in discriminating between low-grade and high-grade steatosis using radiomics classifier were 0.94 ± 0.09 and 0.91 ± 0.16, respectively.
Clinical feature classifier
Thirteen features were extracted, the three most important: ALT, albumin, and ferritin. The AUROC and accuracy of the clinical feature classifier were 0.74 ± 0.16 and 0.76 ± 0.19, respectively.
Radiologic feature classifier
MRS values were extracted as more important features than the mean or median PDFF values. The AUROC and accuracy of the radiologic feature classifier alone were 0.96 ± 0.08 and 0.92 ± 0.17, respectively.
All combinations of radiomic, clinical, and radiologic classifiers
Eight important features were extracted: MRS mean, MR-PDFF mean, and MR-PDFF median were extracted as the three most important features. The AUROC and accuracy of all combinations of variable features were 0.96 ± 0.09 and 0.91 ± 0.22, respectively.
Pairwise comparison of AUROCs of machine learning classifiers
Table 5 shows the pairwise comparison of the AUROC of the machine learning classifier using Delong’s test. The virtually identical AUROCs of radiologic classifier and combination of all features classifiers were obtained (AUROC = 0.96 ± 0.09 vs. 0.96 ± 0.08, P = 0.279). The AUROC of the radiomics classifier was 0.94 ± 0.09, and there was no statistically significant difference compared to the radiologic classifier (P = 0.400) and the combination of all feature classifiers (P = 0.676). The clinical feature classifier exhibited the lowest diagnostic performance (AUROC = 0.74 ± 0.16). There was a significant difference between the AUROC of the clinical feature classifier and those of the other classifiers (P < 0.001).
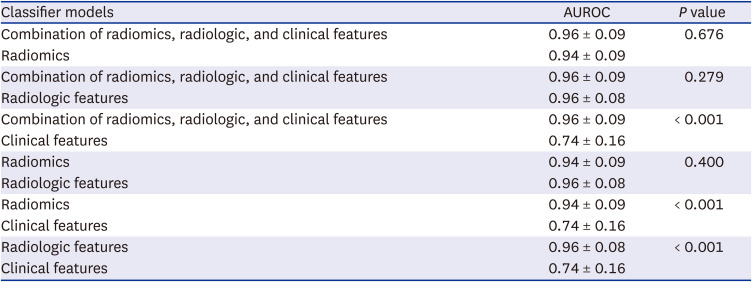
Table 5
Pairwise comparison of the AUROC of the machine learning classifier with Delong’s test
![]()
Go to :
DISCUSSION
This study developed prediction models for liver steatosis in patients with suspected NAFLD based on radiomics, machine learning from MR fat quantification imaging, and various clinical features. This study showed that radiomics analysis of MR-PDFF (AUROC = 0.94 ± 0.09) could accurately differentiate high-grade steatosis (grade 2 or grade 3) from low-grade steatosis (grade 0 or grade 1) in patients with suspected NAFLD and AUROC of MR-PDFF radiomics was comparable to that of radiologic measures (0.96 ± 0.06). Our study aimed to investigate the difference between MR-PDFF using ROI measurement, which is widely used as the gold standard, and radiomic analysis, which has recently been in the spotlight. However, the AUROC of the MR-PDFF radiomics analysis showed a slight decrease rather than an increase compared to conventional radiologic measures, without a statistical difference (P = 0.400). Our results suggest that the current radiomics analysis under specific conditions may have a lower AUROC than the existing simpler measurement method, despite the extra time and effort required. Dzyubak et al.35 have already published a study using the auto-segmentation tool, which is the first step of radiomics analysis; however, if radiomics and machine learning software are embedded in picture archiving and communication systems, radiomics analysis can be applied more widely in the future.
In addition to hepatic tumors, several radiomics studies have been conducted on chronic liver disease, mainly focusing on the staging of liver fibrosis.173637 A radiomics analysis related to liver steatosis was only conducted in one study38; however, CT was used as an imaging modality. A limitation of the study by Naganawa et al.38 was that it did not represent the whole liver using only a single slice and a single small ROI, which did not match the direction of the radiomic analysis, where whole-volume segmentation is important. Chronic liver disease is associated with changes in liver volume, morphology, and texture. Moreover, these changes can show spatial heterogeneity. Therefore, the authors’ study could reflect the whole liver information and is the first radiomics study to predict the grade of steatosis using MR images, especially MR-PDFF images.
It is believed that it is very difficult to match the meaning of the radiomic feature values and terms that a radiologist interprets as MR-PDFF images one by one. In the fat fraction image of MR-PDFF, the liver appeared brighter as the degree of steatosis increased, correlated with the increase in signal intensity in the ROI measurement. In addition, as the degree of steatosis increases, vascular structures such as the hepatic vein and portal vein are observed with dark signal intensity; thus, the contrast with the liver parenchyma is clear. The most important feature was wavelet-LLL NGTDM coarseness,30 which showed an average high value in low-grade steatosis, indicating a lower spatial change rate and a locally more uniform texture. Interestingly, the same second-order statistics, NGTDM Busyness,30 showed a low value in low-grade steatosis, indicating no rapid changes in intensity between pixels and their neighborhood. These radiomics feature values were consistent with liver expression with homogeneous low signal intensity in low-grade steatosis MR-PDFF images. In contrast, the liver shows an overall bright signal intensity in high-grade steatosis. In such a bright background, if there are blood vessels observed as signal void or uneven steatosis areas observed as heterogenous signal intensity, the liver is considered to represent a high NGTDM busyness feature and a low NGTDM coarseness feature. Additionally, features related to brightness, such as first-order mean and median, were naturally selected.
There are many studies on the correlation between MRS, MR-PDFF, and liver biopsy, which are representative methods for quantifying hepatic steatosis.1439404142 Although there were subtle differences in the results, both MRS and MR-PDFF showed an excellent correlation with the histologic grade of liver steatosis. Considering the liver volume included when measuring steatosis, it can be divided into MR-PDFF and radiomics, which can analyze the whole liver, and MRS and biopsy, which can analyze the limited volume.14 Although liver biopsy with histological scoring is used as the gold standard for diagnosing hepatic steatosis, a biopsy could be insensitive to small but important changes in liver fat content due to sampling variability, broad grading categories, and inter- and intra-rater variability. These limitations can be equally applied to MRS. However, in our study, MRS had a higher ICC with pathologic steatosis than MR-PDFF, and MRS showed the highest feature importance among radiologic features. Several reasons can be hypothesized as to why MRS was selected as the test method that was best correlated with liver biopsy for grading liver steatosis. First, the right lobe, where MRS is measured mainly, is close to the liver biopsy site (segment 5/6). In contrast, MR-PDFF also included the left and right superior segments. Second, there may be statistical bias due to the small number of subjects. Therefore, for the initial test of hepatic steatosis, it would be appropriate to perform MRS with MR-PDFF, which can evaluate the entire liver. For follow-up, it would be useful to observe changes in hepatic steatosis with non-invasive MR-PDFF.
Several demographic data showed significant differences between the low- and high-grade steatosis groups. ALT, albumin, and ferritin levels were the most important clinical features (Table 4). It can be confirmed that all these values were measured as statistically significant high values in the high-grade steatosis group (Table 1). Results, such as higher serum ALT, AST, ferritin, and obesity levels were confirmed to be in good agreement with the known laboratory and clinical risk factors related to the severity of NAFLD.434445 However, it cannot be used as a diagnostic tool to classify liver steatosis using only these clinical features (AUROC = 0.74 ± 0.16). These clinical features can be used as important markers in the setting of treatment monitoring after diagnosis or to increase the diagnostic conspicuity of patients suspected of NAFLD based on MR-PDFF. In our study, the high-grade steatosis group showed a younger age, and a higher albumin level was the opposite of known risk factors for NAFLD.4546 This may be due to the small number of patients in our study.
This study has several limitations that warrant further research. First, this study has the disadvantage of being a single-center study with a relatively small number of patients. As a result, the study population size was not sufficiently large to be divided into training and validation sets for use in the recent radiomic pipeline.4748 Second, no external validation for machine learning was performed, which limits the generalizability of our results. Third, selection bias may have been present due to the retrospective design of the study. Fourth, the grades of pathological steatosis in our study population were not equivalent, and there were more patients in grades 0–1 than in grades 2–3. Among them, 18 patients with less than 5% of hepatic steatosis confirmed through pathology were included in the low-grade steatosis group. Fifth, the inter- and intra-observer reliabilities of the multiple small- and whole-volume segmentation ROI measures could not be assessed. However, these shortcomings would have been overcome because multiple ROI drawings were performed up to nine times, and whole-volume segmentation was performed after sufficient training by a software applicator.
In conclusion, radiomic analysis using MR-PDFF provides a diagnostic performance comparable to that of conventional MR-PDFF analysis for the assessment of steatosis grading in patients with suspected NAFLD. Therefore, MR-PDFF-derived radiomics may provide a comparable alternative for grading liver steatosis in patients with suspected NAFLD.
Go to :
 XML Download
XML Download