

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Recovery after death was first introduced to the medical literature in 1982 and the term “Lazarus” was used in 1986 to describe recovery after discontinuing cardiopulmonary resuscitation (CPR).12 The Lazarus phenomenon, also known as autoresuscitation, Lazarus syndrome, or delayed return of spontaneous circulation (ROSC) after failed CPR, is the spontaneous restoration of circulation following the termination of failed CPR maneuvers. Its true incidence is unknown, but it is likely that it is underreported due to medicolegal concerns or under-recognition. The Lazarus phenomenon should be emphasized and understood. In one scoping review of 65 patients who had shown the Lazarus phenomenon, 28% of them recovered completely. The majority of them had a positive neurological outcome.3
I present a traumatic cardiac arrest case in which ventricular tachycardia developed spontaneously after death was declared. At the time of declaration, the electrocardiography (ECG) rhythm was asystole. The patient died again without ROSC despite the additional resuscitation, so it is not a true Lazarus phenomenon. However, this is extremely unusual, and I believe it to be a different type of Lazarus phenomenon.
Go to : 
CASE DESCRIPTION
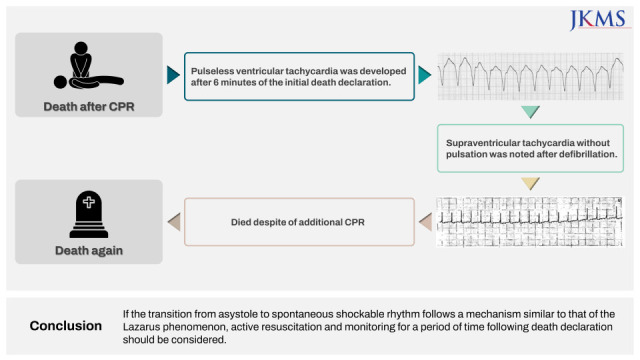
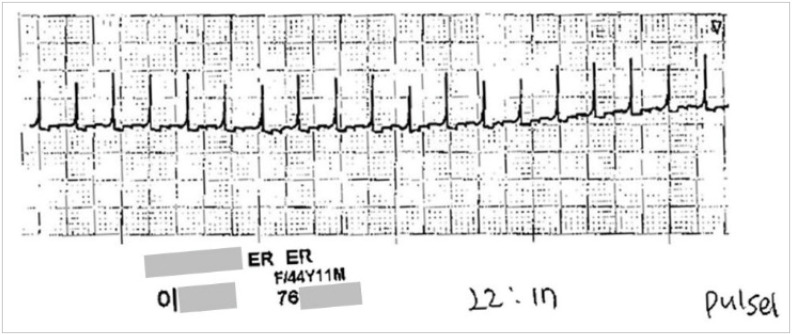
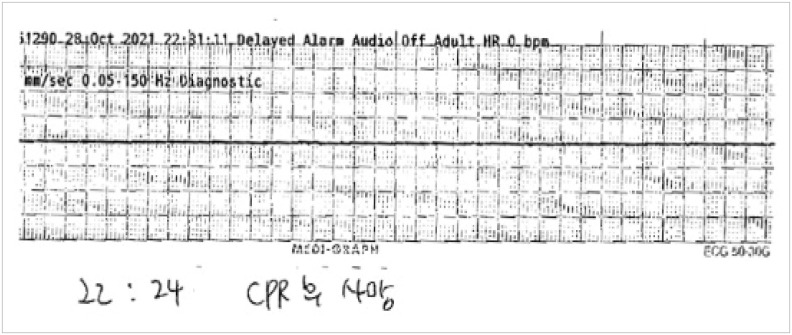
A 44-year-old woman without any previous medical history was run over by a bus and suffered a cardiac arrest on the spot. The emergency medical service (EMS) transported her to our level 1 trauma center. EMS placed an extraglottic airway with I-gel and administered CPR during the transport. When she arrived, her mental status was in a coma. The car wheel mark on her upper chest and extensive subcutaneous emphysema from neck to lower legs were noted. Asystole was the initial ECG rhythm. Emergency treatments, including CPR, were initiated in accordance with the Advanced Trauma Life Support guideline. Endotracheal intubation was used to replace the I-gel. The chest was compressed using a mechanical device, LUCAS (Physio-Control Inc./Jolife AB, Lund, Sweden). One miligram of epinephrine was given every 3 minutes. The transfusion was done. No breathing sound was heard, and tension pneumothorax was suspected. So, bilateral thoracostomies were performed. During the thoracostomy, bilateral hemothoraces were discovered. She was declared dead after 30 minutes of CPR without any ROSC. During CPR, no other ECG rhythm than asystole was seen. At the time of declaration, the monitoring device was maintained without immediate removal. The ECG monitor suddenly showed ventricular tachycardia after 6 minutes of death declaration, but no pulse was palpable (Fig. 1). An echocardiography was performed right away to identify any cardiac contraction, but no findings could be found due to massive subcutaneous emphysema. Defibrillation of 200 J was performed. The rhythm was then converted to the supraventricular tachycardia without pulsation, which is pulseless electrical activity (PEA) (Fig. 2). CPR, which included epinephrine injection, was resumed. The resuscitation was terminated after another 7 minutes of CPR, and the patient was declared dead once more. The rhythm was asystole (Fig. 3).
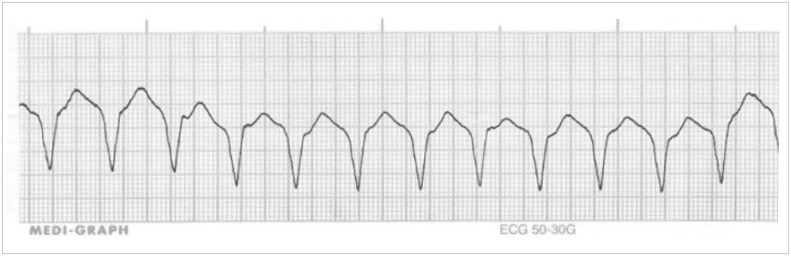 | Fig. 1Pulseless ventricular tachycardia was developed after 6 minutes of the initial death declaration.ECG = electrocardiography.
|
Ethics statement
The present case report was reviewed and approved by the Institutional Review Board of Dankook University Hospital (DKUH 2022-03-010). The informed consent was waived by the board.
Go to :
DISCUSSION
Because this case only showed spontaneous ventricular arrhythmia without ROSC after death declaration, it is difficult to say whether it is a true Lazarus phenomenon. She died after several minutes of additional resuscitation but showed a spontaneous shockable rhythm that required defibrillation converted from asystole. It is known that shockable rhythms, such as pulseless ventricular tachycardia and ventricular fibrillation, have a higher survival discharge rate than non-shockable rhythms (e.g., asystole or PEA).4 These studies, of course, were conducted on patients who had a non-traumatic cardiac arrest. Patients with traumatic cardiac arrest have a very low survival discharge rate5 and the reports of the Lazarus phenomenon are rarer in trauma patients. In this case, there are two key points to consider.
First, this occurred in a trauma patient. The Lazarus phenomenon is commonly associated with medical conditions. In trauma, on the other hand, is uncommonly reported. The following are examples of trauma-related Lazarus phenomena that have been documented in the literature. It was discovered during the treatment of a self-shooting male patient in one case. It happened after 1 month of hospitalization, due to hemorrhagic shock-induced cardiac arrest during formal vein cannulation for dialysis, rather than right after the accident. The Lazarus phenomenon has nothing to do with the trauma.6 So far, two more cases of trauma have been reported.78 What these cases have in common is that they were accompanied by severe chest injuries and PEAs were confirmed by cardiac arrest ECG rhythm. A severe chest injury was also present in this case. The initial rhythm; however, was asystole. The following possibility should be considered in the case of PEA in trauma. Despite cardiac contraction with the organized ECG rhythm, profound shock, severe hypotension or massive subcutaneous emphysema can make it impossible to feel the pulsation. It is easy to confuse it with cardiac arrest; that is pseudo-PEA. Although echocardiography can be used to visually confirm cardiac contraction in pseudo-PEA, it may be ineffective in cases of severe chest injury or subcutaneous emphysema. CPR is inevitably performed in this situation, even if it is not a true cardiac arrest, and this is mistaken for PEA. The cardiac contraction could not be identified by echocardiography in my case due to extensive subcutaneous emphysema, so pseudo-PEA could not be excluded. However, the initial death was confirmed as asystole was presented on an ECG monitor for several minutes after initial CPR termination. During postmortem care, I discovered the pulseless ventricular tachycardia on the monitor. It is still unclear why ventricular arrhythmia suddenly appeared. However, it is important to remember that this can also happen in patients who have suffered a traumatic cardiac arrest and that patients should be monitored for a period of time even after the declaration of death. Signs of life are usually visible within 15 minutes of death, but they can be discovered up to 35 minutes later.9 Signs of life were observed in 47% of cases within 5 minutes, and 22% were 6–10 minutes according to one scoping review. The Lazarus phenomenon was mostly observed between 3 and 8 minutes in a 6-year EMS prospective observational study.10 For these reasons, most studies recommend that patients be monitored for at least 10 minutes after the declaration of death.311
Second, I believe that a case in which an ECG appears spontaneously without ROSC should be classified as a subtype of the Lazarus phenomenon. Until now, this case could not be classified as the Lazarus phenomenon. However, pulseless ventricular tachycardia, which can occur during cardiac arrest, is a kind of shockable rhythm that necessitates defibrillation, and aggressive CPR should be considered as a result, necessitating further discussion. When cardiac arrest patients who initially had a non-shockable rhythm switch to shockable rhythm during CPR, survival discharge and neurological prognosis are reported to be better.1213
In trauma patients, the Lazarus phenomenon is less common. In some surveys of intensivists and emergency physicians, 37–50% said they have experienced the Lazarus phenomenon at medical practices.1415 However, I do not believe that this will become commonplace. This is because the above studies are based on surveys, and medical personnel who have participated in the treatment of Lazarus phenomenon cases or subsequent discussion at an institution can respond to the survey as if it were their own experiences and resulting in an overestimation of experience. If it is such a common occurrence, medical personnel would be very familiar with the Lazarus phenomenon, and they would not report a case in the literature if they have encountered it. In an EMS prospective observational study for 6 years conducted in Finland, the Lazarus phenomenon incidence was announced as 5.95/1,000 prehospital CPR-terminated victims.10 They performed prehospital CPR on 1,376 patients and left 840 at the scene. A total of five Lazarus phenomena have been observed. This would be a good approximation of true incidence. This is the first case of its kind in South Korea, according to the medical literature. Two cases have been reported to the media in 2014 and 2017.
Possible mechanisms of the Lazarus phenomenon include delayed venous return due to auto-positive end-expiratory pressure, hyperinflation, myocardial reperfusion due to dislodged embolized plaque, alkalosis, delayed effect of drugs, hypothermia, hyperkalemia, and myocardial stunning.911 More research is needed to understand a clear mechanism. In summary, if the transition from asystole to shockable rhythm follows a mechanism similar to the Lazarus phenomenon, active resuscitation and monitoring for a period of time (at least 10 minutes) following death declaration should be considered.
Go to :
 XML Download
XML Download