

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Since the outbreak of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2; coronavirus disease 2019 [COVID-19]) in Hubei Province, China, in December 2019,1 there have been more than 510 million cases, 6 million deaths worldwide. Seventeen million cases and 23 thousand deaths in South Korea have been ascribed to COVID-19.2
With mounting cases of COVID-19, the Community Treatment Center (CTC) was deployed in South Korea for mild cases during the acute COVID-19 phase. Admission criteria at the time of entry were: patients who 1) are asymptomatic or mildly symptomatic; 2) have no or well-controlled underlying diseases; 3) do not require oxygen treatment. If symptoms aggravated and required medical care, the patient was transferred to a hospital.
The ongoing pandemic commonly manifests constitutional, cardiopulmonary, neurological, and gastrointestinal symptoms during the acute phase.34 Still, COVID-19 can produce prolonged debilitating sequelae, namely the “Long COVID.”5 In a nationwide study on the US Veterans, an association was found between the severity of COVID-19 and long COVID.6 One systematic review pointed out that although COVID-19-associated symptoms were more distinct in patients with severe illness, individuals with mild and moderate severity also reported various symptoms after the acute phase.7 Also, in a study on home-isolated young patients, 61% reported residual symptoms at 6 months, irrespective of the disease severity during the acute phase.8
Published data have concentrated on hospitalized patients. Hence, the impact of clinical sequelae on non-hospitalized patients with mild severity remains elusive. A case-fatality ratio of 0.13% in South Korea9 and increasing number of COVID-19 survivors highlight the necessity of investigation into long COVID and its impact on survivors’ health in mild cases. This study aimed to determine persistent symptoms in asymptomatic and mildly symptomatic patients and their impact on health-related quality of life (HRQoL) using the EuroQol-5 dimensions-5 levels (EQ-5D-5L) measure.
METHODS
Study design and data collection
This prospective online survey study was conducted on COVID-19 patients admitted to Seongnam CTC, located in Gyeonggi province, South Korea, from November 23rd, 2021 to January 2nd, 2022. All cases were reverse transcription-polymerase chain reaction-confirmed. No antiviral therapy was administered. On admission day, patients above the age of 19 were invited to participate in the study, and those who agreed, filled in an online survey via cellular phone. The questionnaires on the survey consisted of date of birth, height, weight, smoking status, underlying medical conditions, present symptoms, and EQ-5D-5L measures. Electronic medical records were reviewed to update baseline symptoms and underlying medical conditions. Three months after discharge, patients were re-invited to fill out an online survey, which consisted of persistent symptoms and EQ-5D-5L questionnaires.We used the EuroQol Group’s EQ-5D-5L questionnaire,10 a generally valid and responsive instrument11 in assessing HRQoL, and Korean standard value set to assess HRQoL that is specified to the Korean population.12 The EQ-5D-5L includes 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension has 5 levels of response options (no problems, slight problems, moderate problems, severe problems, and unable to/extreme problems) to denote all possible health states. One level from each dimension is put together to make a combination numbers, ranging from 11111 (complete health state) to 55555 (poor health state). Based on this 5-digit combination of numbers, an index value, preference-based on the general population of a country, is provided, ranging from −0.066 (worst HRQoL) to 1.000 (best HRQoL) in South Korea, with a score less than 0 representing a health state worse than death.12
Study sample
Two hundred one patients participated in the initial survey. Eight patients were below the age of 19, not meeting the inclusion criteria. Four patients were transferred to a hospital due to pneumonia and 2 due to conditions requiring other medical needs and were subsequently excluded from the study. Forty patients declined to return to the follow-up survey. A total of 147 participants completed the follow-up survey.
Definitions
Persistent or residual symptoms in this study were defined as any remaining or newly identified symptoms related to COVID-19 that were present at the time of follow-up. Messenger ribonucleic acid (mRNA) and viral vector vaccines were available in South Korea during the study period. Complete vaccination was defined as inoculated with a booster shot or past 14 days from the 2nd dose of vaccination. Any other cases of vaccination were regarded as incomplete. The follow-up period was counted from the day of discharge from the CTC until the day when follow-up online survey was submitted.
For analysis, index values corresponding to the lower quartile were classified as low EQ-5D-5L index values. Symptoms were categorized by organ-systems for logistic regression analysis. Constitutional symptoms included fatigue, chilling sense, febrile sense, hyperhidrosis, anhidrosis, and myalgia. Cardiopulmonary symptoms included sore throat, globus sensation, sputum, rhinorrhea, nasal congestion, dyspnea, and chest discomfort or pain. Neurological symptoms included headache, dizziness, hyposmia, hypogeusia, memory impairment, extremity numbness, brain fog, and eye soreness. Gastrointestinal symptoms included dyspepsia, nausea or vomiting, and diarrhea or constipation. Neuropsychiatric symptoms included anxiety and insomnia. Dermatologic/musculoskeletal symptoms included rash, arthralgia, hair loss, and skin desquamation.
Participants with metabolic disease was defined as those with hypertension (HTN), dyslipidemia (DL), or diabetes mellitus (DM).
Statistical analysis
We conducted a descriptive analysis on baseline characteristics. Continuous variables are presented as median (interquartile range, IQR) or mean ± standard deviation (SD) values, and categorical values are presented as numbers (percentage, %). Categorical variables were analyzed using the χ2 test or Fisher’s exact test, and non-categorical variables were analyzed using the t-test. Logistic regression analysis was used to examine the factors associated with the presence of symptoms and decreased HRQoL at follow-up. Logistic regression analysis was adjusted for age, sex, body mass index (BMI), smoking status, underlying medical conditions, and vaccination status. Two-sided P values < 0.05 were considered statistically significant. All analyses were performed using Stata Version 16.1 (StataCorp, College Station, TX, USA).
RESULTS
Demographics and characteristics
Table 1 shows the incidence of demographic characteristics, smoking status, and underlying medical conditions of the participants. Of the 147 participants (median [IQR] age, 51.0 [43.0–61.0] years), symptomatic patients were younger than asymptomatic patients (P = 0.044), but no difference in age groups between asymptomatic and symptomatic participants were identified (P = 0.062). Seventy-nine (53.7%) were male and 68 (46.3%) were female. There were more males than females with symptoms at baseline (P = 0.006). The median (IQR) BMI was 23.9 (21.3–26.6). Eighty-five (57.8%) were never smokers, 42 (28.6%) were ex-smokers, and 20 (13.6%) were current smokers. Sixty-seven participants (45.6%) did not have any underlying diseases. HTN was the most common comorbidity (40 [27.2%]) followed by DL (18 [12.2%]), DM (14 [9.5%]) and cancer of any type (11 [7.5%]). Incidences of other medical conditions are demonstrated in Table 1. A hundred and fourteen patients (77.6%) had completed their COVID-19 vaccination and 33 (22.4%) had incomplete or uncertain vaccination history. The median (IQR) length of stay in the CTC and the interval period (IQR) between the initial and follow-up survey were 8.0 (7.0–9.0) and 96.0 (93.0–98.0) days, respectively. According to BMI, smoking status, underlying medical conditions, vaccination status, length of stay, and follow-up period, no difference between asymptomatic and symptomatic patients was identified (P = 0.295, 0.543, 0.876, 0.531, 0.162, and 0.643, respectively) (Table 1).
Table 1
Clinical characteristics of 147 participants at baseline
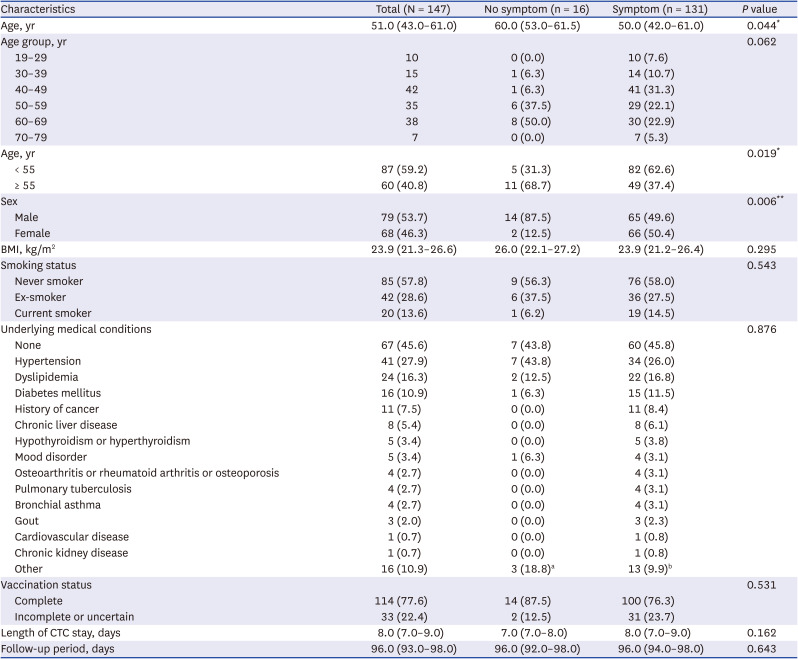
Values are presented as median (interquartile range) or number (%).
BMI = body mass index, CTC = Community Treatment Center.
aTwo benign prostatic hyperplasia, 1 arrhythmia.
bFour benign prostatic hyperplasia, 2 arrhythmia, 1 allergic rhinitis, 1 cerebral aneurysm, 1 postherpetic neuralgia, 1 benign paroxysmal positional vertigo, 1 cervical stenosis, 1 hearing loss, 1 spinal cord meningioma.
*P < 0.05; **P < 0.01.
Characteristics of clinical sequelae and HRQoL assessment
At baseline, 131 of 147 patients (89.1%) had 1 or more symptoms. Upper respiratory symptoms (cough [61.2%], sputum [55.8%], rhinorrhea [51.0%], and sore throat [34.7%]) and neurological symptoms (headache [22.5%], hyposmia [21.1%], and hypogeusia [20.4%]) were pervasive. Eighty-two (55.8%) participants were symptomatic at follow-up. The most common persistent symptoms were fatigue (48 [32.7%]), memory impairment (22 [15.0%]), hyposmia (21 [14.3%]), anxiety (14 [9.5%]), myalgia (11 [7.5%]), hypogeusia (10 [6.8%]), and dizziness (10 [6.8%]) (Fig. 1). As shown in Table 2, neurological and neuropsychiatric symptoms demonstrated a correlation at baseline and follow-up (P = 0.006 and < 0.001, respectively).
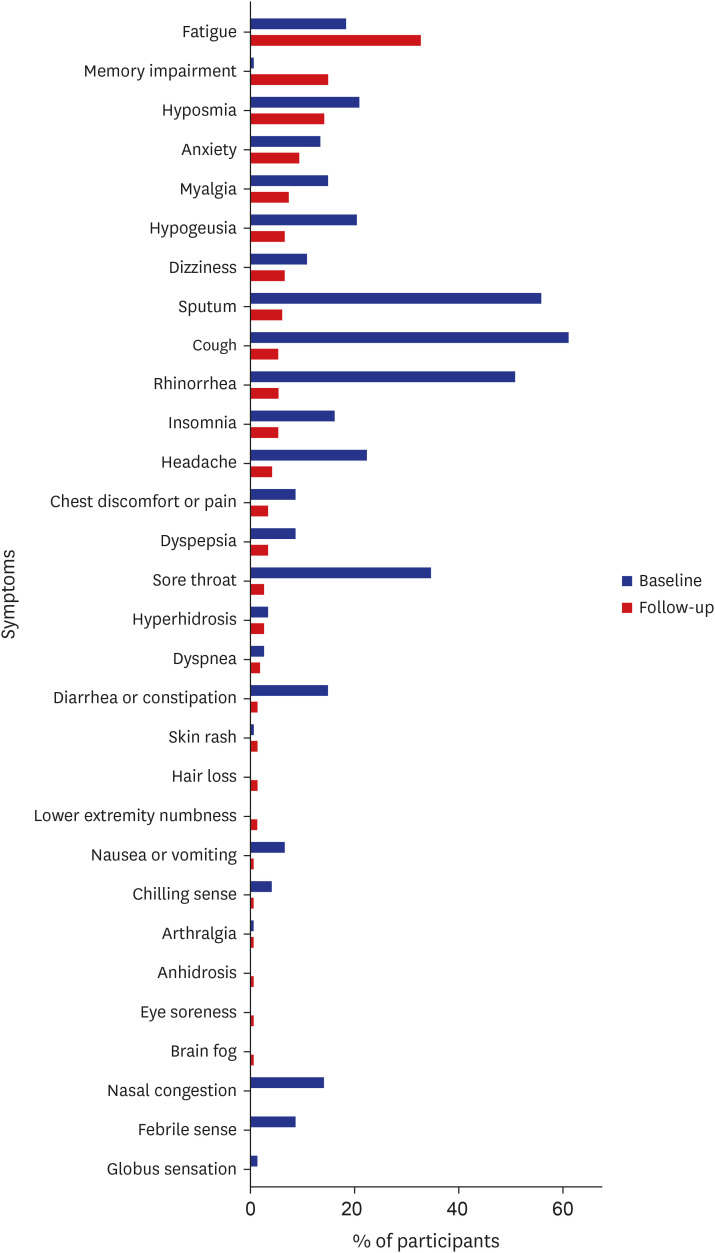
Table 2
Symptoms and EQ-5D-5L index values at baseline and follow-up
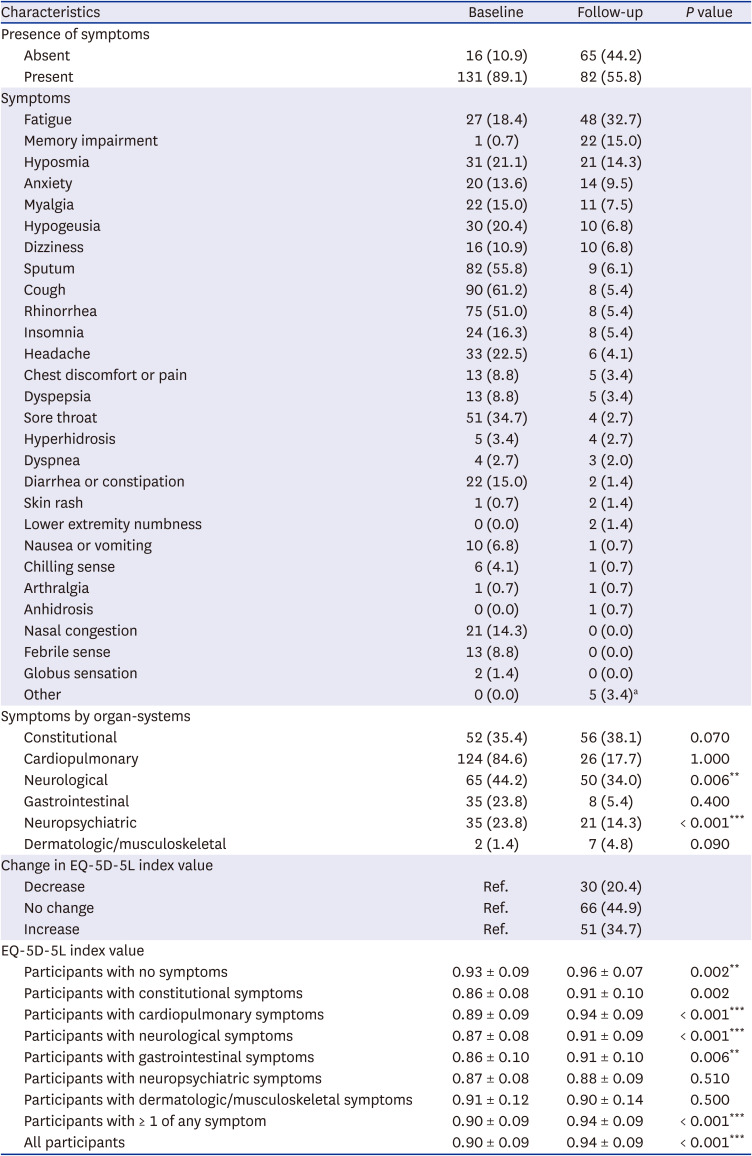
While 30 out of 147 participants (20.4%) reported a decline in EQ-5D-5L index value compared with baseline, 66 (44.9%) expressed no change and 51 (34.7%) reported increased index values. Participants with neuropsychiatric symptoms had the lowest mean EQ-5D-5L index values at follow-up (0.88 ± 0.09) and presented an insignificant statistical difference between baseline and follow-up (P = 0.507). The mean EQ-5D-5L index values at follow-up (0.94 ± 0.09) was higher than that of baseline (0.90 ± 0.09) in symptomatic participants (P < 0.001). The mean EQ-5D-5L index values at baseline and follow-up of all participants were 0.90 ± 0.09 and 0.94 ± 0.09 respectively (P < 0.001) (Table 2).
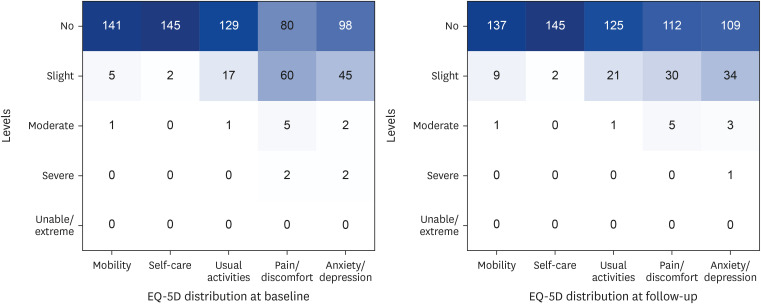
At baseline and follow-up, the number of patients reporting no, slight, moderate problems on mobility dimension changed from 141 (95.9%) to 137 (93.2%), 5 (3.4%) to 9 (6.1%), 1 (0.7%) to 1 (0.7%), respectively. No participant reported severe nor unable to/extreme problems on either point. On the self-care dimension, the number of patients reporting no and slight problems was 145 (98.6%) and 5 (1.4%), respectively. There was no change incidence-wise. No participant reported moderate, severe, or unable to/extreme problems at baseline and follow-up. The number of patients suffering from no, slight, and moderate problems on usual activities dimension changed from 129 (87.8%) to 125 (85.0%), 17 (11.6%) to 21 (14.3%), and 1 (0.7%) to 1 (0.7%), respectively. No participant reported severe nor unable to/extreme problems on either point. The number of patients reporting no, slight, moderate, and severe problems on pain/discomfort dimension was 80 (54.4%) vs. 112 (76.2%), 60 (40.8%) vs. 30 (20.4%), 5 (3.4%) vs. 5 (3.4%), 2 (1.4%) vs. 0 (0.0%), respectively. No participant reported unable to/extreme problems at neither baseline nor follow-up. The number of patients reporting no, slight, moderate, and severe problems on anxiety/depression dimension was 98 (66.7%) vs. 109 (74.1%), 45 (30.6%) vs. 34 (23.1%), 2 (1.4%) vs. 3 (2.0%), 2 (1.4%) vs. 1 (0.7%), respectively. No participant reported being unable to/extreme problems on either point. The prevalence of the 5 dimensions is demonstrated in Fig. 2.
Factors associated with presence of persistent symptoms and decline of EQ-5D-5L index values
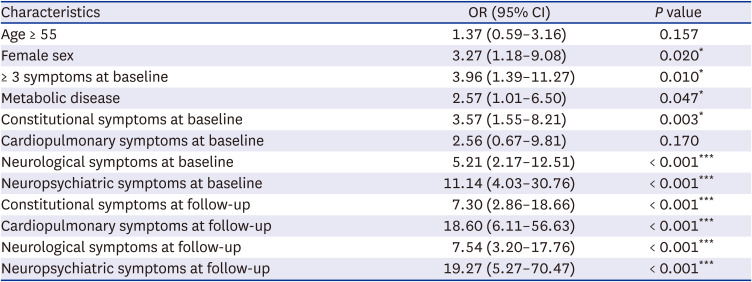
After observing the change of EQ-5D-5L among participants, factors associated with low EQ-5D-5L index values at follow-up were investigated. Female sex (odds ratio [OR], 3.27 [1.18–9.08], P = 0.020), more than 3 symptoms at baseline (OR, 3.96 [1.39–11.27], P = 0.010), presence of metabolic disease (OR, 2.57 [1.01–6.50], P = 0.047), constitutional, neurological, and neuropsychiatric symptoms at baseline (OR, 3.57 [1.55–8.21], P = 0.003; OR, 5.21 [2.17–12.51], P < 0.001; and OR, 11.14 [4.03–30.76], P < 0.001, respectively) were associated with low EQ-5D-5L index values. Also, constitutional, cardiopulmonary, neurological, and neuropsychiatric symptoms (OR, 7.30 [2.86–18.66], P < 0.001; OR, 18.60 [6.11–56.63], P < 0.001; OR, 7.54 [3.20–17.76], P = 0.005; and OR, 19.27 [5.27–70.47], P < 0.001, respectively) at follow-up were associated with the low values. Increasing age was not a relevant factor (Table 3).
Table 3
Factors associated with low 5-level version of the EuroQol 5-dimensional questionnaire index values at follow-up
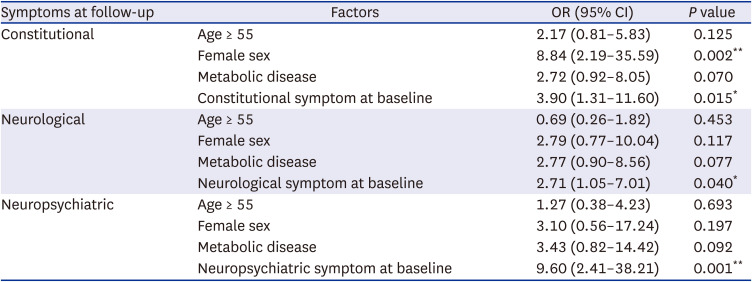
Next, factors associated with persistent symptoms and low EQ-5D-5L index values were investigated. We defined symptoms of interest as the most common persistent symptoms, which were fatigue, memory impairment, hyposmia, anxiety, myalgia, hypogeusia, and dizziness. Symptoms of interest were grouped into organ-systems and analyzed with age ≥ 55, female sex, presence of metabolic disease, and presence of the corresponding symptom at baseline. According to logistic regression, no association between symptoms, low EQ-5D-5L index values, and increasing age was found. Female sex was relevant for constitutional symptoms (OR, 8.84 [2.19–35.59], P = 0.002). Presence of constitutional, neurological, and neuropsychiatric symptoms at baseline was associated with persistent corresponding symptoms (OR, 3.90 [1.31–11.60], P = 0.015; OR, 2.71 [1.05–7.01], P = 0.040; and OR, 9.60 [2.41–38.21], P = 0.001, respectively) (Table 4).
Table 4
Factors associated with organ-system symptoms and low 5-level version of the EuroQol 5-dimensional questionnaire index values at follow-up
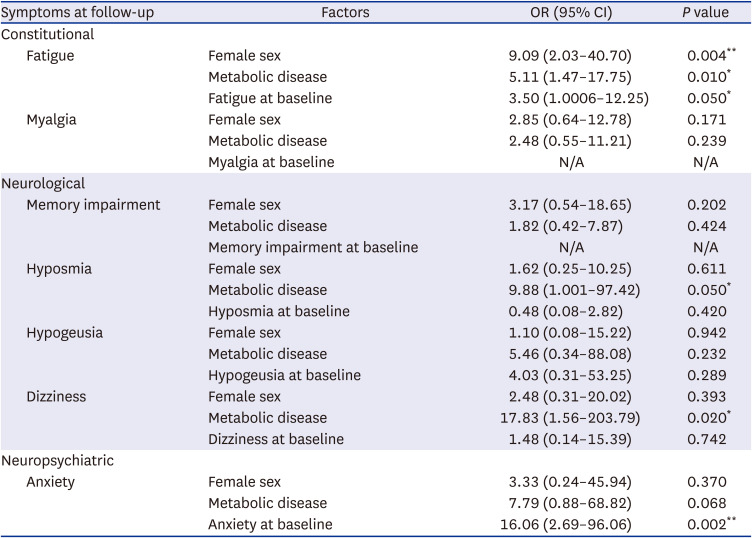
Seven most commonly identified persistent symptoms were analyzed in subgroup analysis. Female sex (OR, 9.09 [2.03–40.70], P = 0.004), patients with metabolic disease (OR, 5.11 [1.47–17.75], P = 0.010), and fatigue at baseline (OR, 3.50 [1.0006–12.25], P = 0.050) had higher odds of fatigue and low EQ-5D-5L index values at follow-up (Table 5). The presence of metabolic disease was a relevant factor for both hyposmia and dizziness (OR, 9.88 [1.001–97.42], P = 0.050; and OR, 17.83 [1.56–203.79], P = 0.020, respectively). Participants with anxiety at baseline (OR, 16.06 [2.69–96.06], P = 0.002) were at higher odds of persistent anxiety at follow-up than those without at baseline. No factors were associated with myalgia, memory impairment, and hypogeusia.
Table 5
Subgroup analysis for the factors associated with symptoms and low 5-level version of the EuroQol 5-dimensional questionnaire index values at follow-up
DISCUSSION
Based on the data collected from CTC, South Korea, 55.8% of mild COVID-19 survivors reported symptomatic at 3-month post-discharge; the most common residual symptoms were fatigue (32.7%), memory impairment (15.0%), hyposmia (14.3%), anxiety (9.5%), myalgia (7.5%), hypogeusia (6.8%), dizziness (6.8%). Similar to the findings of Ding et al.13 our study revealed that at follow-up, cardiopulmonary symptoms such as chest discomfort or pain, dyspnea, cough were minimal and constitutional, neurological and neuropsychiatric symptoms were pervasive in isolated patients.
On EQ-5D-5L, 25.9% had anxiety/depression, 23.8% had pain/discomfort, 15.0% had problems with usual activities, 6.8% had problems with mobility, and only 1.4% had self-care problems at follow-up. Although our study participants were of mild severity, participants with neuropsychiatric symptoms (anxiety and insomnia) reported having the lowest mean EQ-5D-5L index value at follow-up. Also, anxiety at baseline is associated with anxiety at follow-up. We expected neuropsychiatric symptoms to improve after discharge as participants left the CTC, an unfamiliar environment, and returned to their residences but the mean EQ-5D-5L index value remained the lowest of all symptoms with an insignificant difference (P = 0.507) from that of baseline, and anxiety at baseline was associated with anxiety and low EQ-5D-5L index values at follow-up (OR, 16.06 [2.69–96.06], P = 0.002), which indicates that neuropsychiatric symptoms continued to affect HRQoL after recovery. This continuity can be explained by job and wage losses, uncertainty about the future, and the fear associated with the pandemic itself, such as losing a family member or a friend.14
Except for those with neuropsychiatric and dermatologic/musculoskeletal symptoms at baseline, the mean EQ-5D-5L index values were significantly higher at follow-up than baseline (Table 2), indicating an improvement in HRQoL. The mean EQ-5D-5L index value of participants with no symptoms was found to be comparable to that of the general adult population, as the mean ± SD EQ-5D-5L index value of the adult population in South Korea in 2017 was reported to be 0.97 ± 0.08.15
Sudre et al.16 reported that old age, female sex, disease severity, and BMI were attributes and predictors of long COVID. Our study also revealed similar results in that female sex and having more than 3 symptoms during the acute COVID-19 infection was associated with decreased HRQoL at follow-up. Yet, age and BMI were not relevant factors in our case. Also, unlike the results from studies in the US proving the association between vaccination with mRNA, viral vector vaccines and less COVID-19 hospitalization,1718 vaccination status showed no statistical significance to long COVID. This may be attributable to the difference in disease severity between the study participants. Patients who needed hospitalization or oxygen supply or had uncontrolled underlying diseases were excluded from our study, thereby neutralizing the effect of age, BMI, and vaccination status on patients with minimal disease burden.
In our study, among the major neurological symptoms, the presence of metabolic disease was at higher odds of hyposmia and dizziness with diminished HRQoL at follow-up. Although the mechanisms of SARS-CoV-2-specific immune responses remain elusive, possible explanations for neurological manifestations are systemic hypoxia leading to brain injury and oxidative stress and microglial activation from COVID-19 inflammation inducing neuronal injury, leading to declining neurological functions.1920 Together with the impact of metabolic diseases on central and peripheral nervous systems,21222324 patients with HTN, DL, or DM may be prone to neurological symptoms in the long term. Yet, our study’s wide confidence intervals prompt for future studies with a larger sample size for more precise population estimates.
COVID-19 poses comparable but distinct complications on those contracted25 when placed in juxtaposition with other Coronaviruses. For one, infected Middle East respiratory syndrome (MERS) and SARS patients commonly experience lung function abnormalities, chronic fatigue, anxiety or depression, and neuropsychiatric disorders,262728 but neurological symptoms are more common in severe COVID-19 patients.29 Until the end of February 2022, confirmed MERS and SARS have reached 2,585 and 8,096 cases with a case-fatality ratio of 34.4% and 9.6%, respectively.3031 However, the cumulative number of COVID-19 cases far outruns that of SARS and MERS,9 prompting research on long-term sequelae and their effects on HRQoL.
While a prior study concluded that COVID-19 severity is linked to a worse HRQoL,32 other studies have shown the association of mild COVID-19 survivors and decreased HRQoL, similar to our findings. Research has established that survivors with sequelae of COVID-19 are likely to report having a decreased HRQoL.3334 Sixty-three (44.1%) of 143 discharged patients reported worsened quality of life in a study conducted in Italy.35 Another study reported that functional impairment of non-hospitalized patients (n = 96) was similar to that of hospitalized patients’ (n = 22) at 3–4 months post-COVID-19 diagnosis.36 Lower scores for both physical and mental component summary on a group of standardized instruments evaluating neurocognitive function, psychiatric morbidity and quality of life were found in mild-to-severe COVID-19 survivors with neurocognitive impairment (n = 179).37 Given that innumerable persons worldwide are infected with COVID-19 or have recovered from the acute phase, it is necessary to assess the implication of long COVID on HRQoL.
Although EQ-5D-5L covers various domains of daily life and reflects generic health status, there is a shortfall in symptom-specific measurement and dimensions that are not included, such as sleep, concentration or vitality. As majority of survivors suffer from long COVID,38 assessment based on 5-dimensions of life instrument alone may be insufficient to comprehensively analyze HRQoL of COVID-19 survivors. Based on the findings that post-COVID-19 symptom burdens are heterogeneous, including fatigue, anosmia, dyspnea, cough, chest pain, arthralgia, sleep disturbances, and worse mental health,3940 symptom-specific questionnaires or a new preference-based HRQoL instrument must be considered together for evaluation.
There are several limitations in this study. First, collected data on follow-up symptoms were not based on objective evaluation as our online survey was reported directly from participants. Second, the sample size in this study was considered not large enough. Future research might extend the explanations of the effect of lingering symptoms and decreased HRQoL with a larger study sample, providing improved validity and reliability. Third, our study focused on the presence of symptoms, and the severity of symptoms has been overlooked. The correlation of symptom severity and degree of change in HRQoL requires further investigation. Self-selection bias is possible, as patients electing to participate in online follow-up surveys may have more persistent symptoms than the average survivor. The generalizability of results is limited, given that this is a single-institution study.
Despite the limitations, to our acknowledgement, this is the first study conducted in South Korea to report on the clinical sequelae and their impact on HRQoL of asymptomatic or mildly symptomatic COVID-19 patients. Our results stress the need for further investigation into the long-term complications of COVID-19 cases and its health-related effects as long-term symptoms diminish HRQoL in COVID-19 survivors and as the current pandemic is begetting survivors relentlessly.
In conclusion, based on a single CTC sample data, 20.4% of mild COVID-19 survivors reported decreased HRQoL. At follow-up, those with neuropsychiatric symptoms (anxiety and insomnia) were identified with the lowest mean EQ-5D-5L index value. Female sex, manifesting more than 3 symptoms during the acute COVID-19 phase, identified constitutional, cardiopulmonary, neurological, and neuropsychiatric symptoms at follow-up were associated with diminished HRQoL. Female sex, presence of metabolic disease, and fatigue at baseline were relevant factors of fatigue and low HRQoL. The presence of metabolic disease had significantly higher odds of hyposmia, dizziness and decreased HRQoL at follow-up. Patients with anxiety at baseline were associated with anxiety at follow-up. Observation of long-term symptoms of COVID-19 with diminished HRQoL and integrated research in COVID-19 survivors are warranted.
 XML Download
XML Download