

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Unexpected cardiac arrest is a major health problem worldwide.1 The incidence of pediatric out-of-hospital cardiac arrest (OHCA) is 1–20 per 100,000 person-years, and the survival rate and neurologic outcomes of pediatric OHCA are poor, with regional variation.234567 The relatively small number of cases and poor survival outcomes cast doubt on the value of pediatric cardiopulmonary resuscitation (CPR).78910 Nevertheless, the survival outcomes of pediatric OHCA patients need to be improved; because of children’s long potential life expectancy, even a few deaths from pediatric cardiac arrest cause significant social and economic losses.11
In the Republic of Korea, the government has endeavored to improve the chain of survival through the National OHCA registry, regular public reports, a mandatory CPR training program, a telephone-assisted CPR program, and medical oversight for emergency medical service (EMS) CPR performance since 2008.1213 Due to those efforts, the survival outcomes of adult OHCA patients in the Republic of Korea have improved, but the survival rate of pediatric OHCA patients has not changed significantly.31415
Epidemiological analyses of OHCA have allowed researchers to find vulnerabilities in the chain of survival and to improve survival outcomes during the past few decades.16 Some studies have reported age-related variations in the mechanisms of OHCA and survival outcomes.17181920 Children’s growth and development vary significantly with age.21222324 As a result, the mechanism of OHCA and survival outcomes also vary significantly with age. Understanding the characteristics and patterns of OHCA in each age group is critical for designing long-term national prevention measures, age-specific resuscitation care strategies, and pediatric OHCA training programs.
New policies are based on epidemiology research, so it is necessary to analyze recent trends and identify variables that affect survival outcomes.1214 In addition, the delivery of pre-hospital emergency care differs from country to country, so research using regional data is needed.62526 Our aim in this study was to use data from the Korea OHCA Registry (KOHCAR) to assess the most recent trends in the epidemiology and survival outcomes of pediatric OHCA patients and to analyze the factors that influence survival outcomes.
METHODS
Study setting
The Republic of Korea occupies an area of 100,431.8 km2 and has a population of more than 50 million people.2728 The Korean EMS is a single-tiered system operated by the government,29 that employs 13,133 EMS personnel and 1,579 EMS vehicles in 17 divisions.29 The EMS transports patients to 517 emergency departments (EDs) across the country.29 EMS personnel are divided into level 1 and level 2 paramedics.29
Data source
We analyzed data from Korean statistics and KOHCAR in the Republic of Korea. The annual total and age-group population and populations of the Republic of Korea were obtained from the Korean Statistical Information Service.30 KOHCAR is maintained by the Korea Disease Control and Prevention Agency (KDCA) in cooperation with the national fire agency, and it contains information about all cardiac arrest patients transported to a hospital via EMS.12
To control the data quality, KDCA employs and trains medical record reviewers to maintain standardized medical records.31 They visit every hospital to assess the records and collect information about treatment and clinical outcomes according to the Utstein guidelines.31 These processes are supervised every month by a national cardiac arrest investigation and surveillance committee that consists of emergency physicians, epidemiologists, statisticians, and medical record reviewers.123132
Study population
Pediatric patients (younger than 18 years) with OHCA between 2009 and 2018 were selected. Cardiac arrest cases were selected when the chief complaint was cardiac arrest or respiratory arrest and EMS personnel performed CPR. We excluded patients who were dead-on-arrival (DOA), had do-not-resuscitate (DNR) orders, or whose outcome information was missing.
We divided the patients into four groups by age: group 1, younger than 1 year; group 2, 1 to 5 years; group 3, 6 to 12 years; and group 4, 13 to 17 years.
Variables
We collected the following demographic information about the patients: sex, age, and medical history. Prehospital data were the date, location, and etiology of OHCA; the type of first responder; and whether the patient received bystander CPR or prehospital treatment from an automated external defibrillator (AED). The analyzed hospital data were ED visit time, initial electrocardiography (ECG) rhythm in the ED, defibrillation in the ED, and CPR duration.
‘Cardiac origin’ describes cardiac arrest caused by failure of the heart itself and cases in which the cause of cardiac arrest is unknown. ‘Respiratory origin’ describes patients with a high-risk respiratory disease and those with acute respiratory distress observed prior to cardiac arrest. ‘Sudden unexpected infant death (SUID)’ describes cases in which a patient younger than 13 months is found dead in bed or when a doctor records sudden infant death syndrome as the cause of death. ‘Other diseases’ describe cases in which the cause of cardiac arrest is clearly diagnosed.
An event location of ‘home residence’ indicates cardiac events that occurred in houses, parking lots, on-site playgrounds or swimming pools, dormitories, and orphanages. An event location of ‘healthcare facilities’ indicates that the event occurred in a medical institution, defined by Korean medical law as midwifery centers, oriental medicine clinics, dental clinics, and hospitals. ‘Places of recreation’ are amusement parks, botanical gardens, parks, theaters, and exhibitions. ‘Public/commercial buildings’ are schools, public institutions, bus terminals, airports, stores, restaurants, and hotels. Kindergartens, daycare centers, and religious buildings are categorized as other.
The time from arrest to arrival at the ED is defined as the time from cardiac arrest (or the last normal time) until ED arrival. CPR duration is defined as time from ED arrival to the end of CPR.
Outcome
The primary outcome was survival to hospital discharge. The secondary outcomes were return of spontaneous circulation (ROSC) at the ED and good neurological status, defined as a pediatric cerebral performance category (PCPC) of 1 or 2 at discharge. PCPC is classified as 1 for good cerebral performance and 2 for moderate cerebral disability.
Statistical analysis
Categorical variables are reported as number and percentage (%), and continuous variables are reported as mean with standard deviation. We performed logistic regression analysis to examine the population-based incidence rates (IRs) with 95% confidence intervals (CIs) for each outcome with age and sex adjustment. Univariate and multivariate logistic regression analyses were conducted to find factors associated with the outcomes of pediatric OHCA. P < 0.05 was considered to indicate statistical significance in all statistical tests. The post hoc analysis used Bonferroni correction. R statistical software version 4.0.5 (R Foundation for Statistical Computing, Vienna, Austria) was used for the statistical analyses.
RESULTS
Annual trends in pediatric cardiac arrests
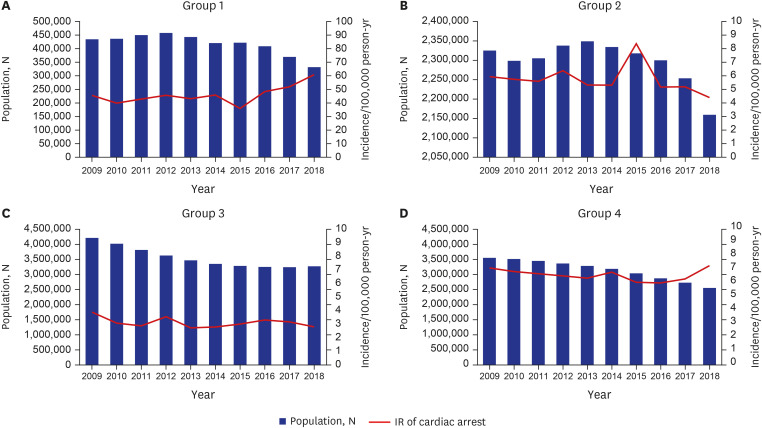
The total population of Korea increased from 50,833,594 in 2009 to 53,599,421 in 2018, but the annual number of births decreased from 454,209 to 348,253 during that time.30 The population of group 1, younger than 1 year, has been decreasing for 10 years, but the IR of pediatric OHCA in group 1 increased from 45.57 to 60.89 (Fig. 1). The IR of pediatric OHCA in group 2 decreased from 5.93 in 2009 to 4.40 in 2018, and the IR of pediatric OHCA in group 3 decreased from 3.89 to 2.81 during the same 10 years. The IR of pediatric OHCA in group 4 increased from 7.15 to 7.32 while the population has been decreasing.
Demographics of pediatric OHCA
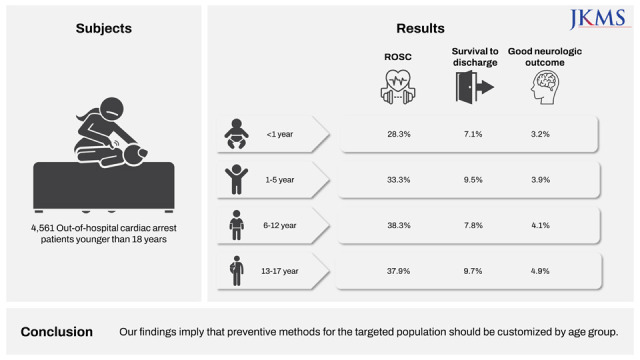
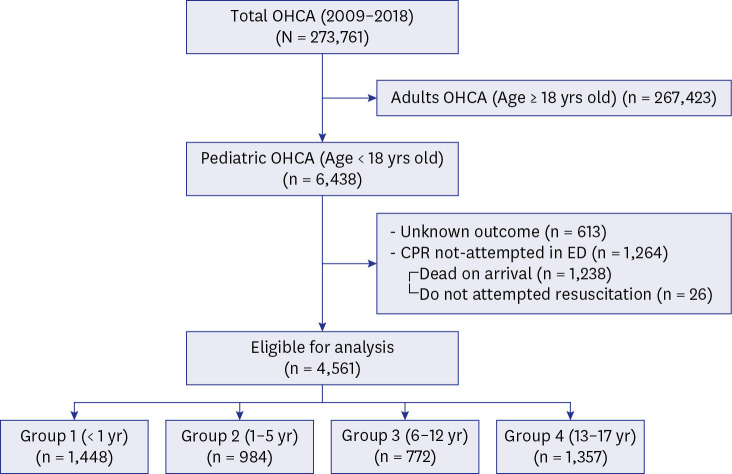
Of the 273,761 OHCAs that occurred in the Republic of Korea between 2009 to 2018, we analyzed 4,561 patients after excluding 267,423 older than 18 years, 613 with no hospital outcome data, 1,238 who were DOA, and 26 with DNR orders (Fig. 2). Of the total study population, group 1 contained 1,448 patients (34.7%); group 2 contained 984 patients (21.6%); group 3 contained 772 patients (16.9%); and group 4 contained 1,357 patients (29.8%).
The mean ages of groups 2, 3, and 4 were 2.5 ± 1.4 years, 9.0 ± 2.0 years, and 15.5 ± 1.4 years, respectively. Males accounted for 57.57% of group 1, 60.8% of group 2, 65.9% of group 3, and 70.7% of group 4 (Table 1).
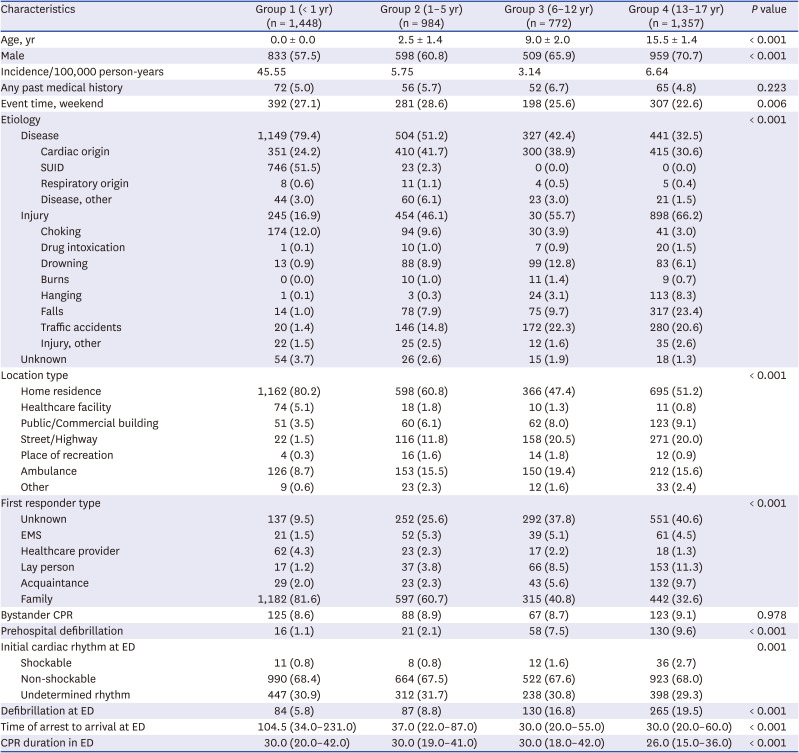
Table 1
General characteristics of the study population by age group
Values are presented as median ± standard deviation, number (%), or median (interquartile range).
SUID = sudden unexpected infant death, EMS = emergency medical service, CPR = cardiopulmonary resuscitation, ED = emergency department.
![]()
The most common cause of cardiac arrest in group 1 was SUID (51.5%), followed by cardiac origin (24.2%) and choking (12.0%). In the other age groups, injury (group 2, 46.1%; group 3, 55.7%; group 4, 66.2%) was the most common cause of cardiac arrest, followed by cardiac origin (group 2, 41.7%; group 3, 38.9%; group 4, 30.6%).
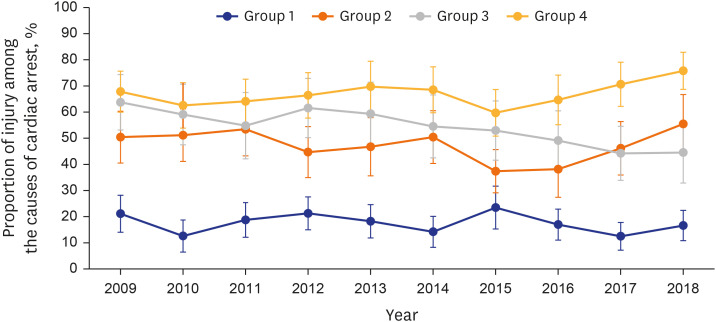
In group 1, choking was the most common cause of cardiac arrest caused by injury, whereas that in group 2 was traffic accident (14.8%) followed by choking (9.6%); in group 3, it was traffic accident (22.3%) followed by drowning (12.8%); and in group 4, it was fall (23.4%) followed by traffic accident (20.6%). Fig. 3 shows the annual changes in injuries that caused pediatric OHCA. In groups 1 and 3, the proportion of injury decreased during the 10-year study period, but it has been increasing in groups 2 and 4 since 2015.
Most of the OHCAs (group 1, 80.2%; group 2, 60.8%; group 3, 47.4%; group 4, 51.2%) occurred at the patient’s home. First responders were often family in all age groups (group 1, 81.6%, group 2, 60.7%, group 3, 40.8%, group 4, 32.6%). The rate of bystander CPR and prehospital defibrillation rate were less than 10% in all age groups.
Only 0.8% of group 1, 0.8% of group 2, 1.6% of group 3, and 2.7% of group 4 initially presented in the ED with a shockable rhythm; and 5.8% of group 1, 8.8% of group 2, 16.8% of group 3, and 19.5% of group 4 received defibrillation at the ED. The median time between the OHCA and arrival at the ED was 104.5 minutes in group 1, 37 minutes in group 2, 30 minutes in group 3, and 30 minutes in group 4. Median CPR duration in the ED was 30 minutes in groups 1, 2, and 3 and 26 minutes in group 4.
Outcomes of pediatric OHCA
Group 4 had the highest survival to hospital discharge rate (9.7%), followed by group 2 (9.5%), group 3 (7.8%), and group 1 (7.1%; Table 2). The rate of good neurologic outcome was also highest in group 4 (4.9%) and lowest in group 1 (3.2%). Fig. 4 shows the trends of pediatric OHCA outcomes from 2009 to 2018. During that 10-year period, ROSC, survival to discharge, and good neurological outcome did not noticeably improve.
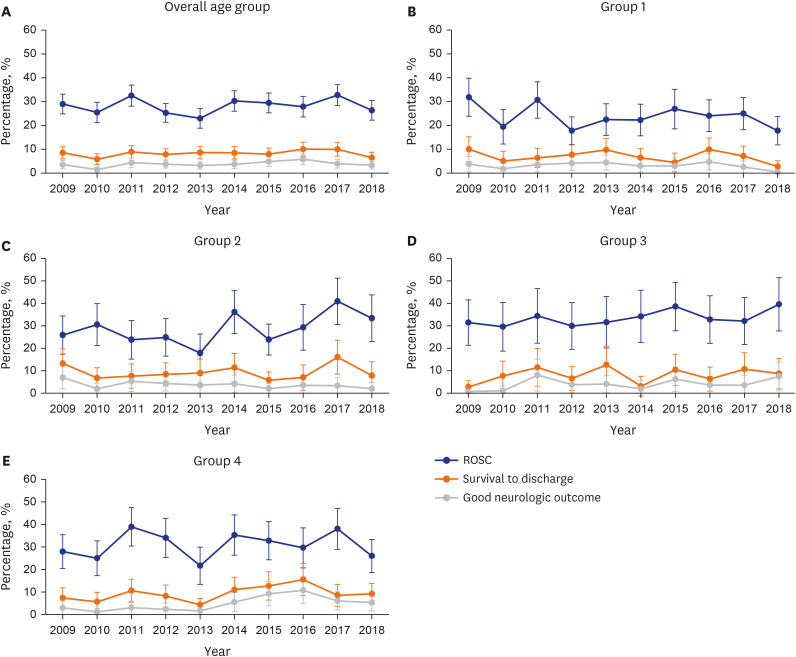

Fig. 4
Trends in ROSC, survival to discharge, and good neurologic outcomes in (A) overall age groups, (B) group 1, (C) group 2, (D) group 3 and (E) group 4 from 2009 to 2018. The line graph (blue) shows the ROSC of each age group. The line graph (orange) shows the survival to discharge of each age group. The line graph (gray) shows the good neurologic outcome of each age group.
ROSC = return of spontaneous circulation.
![]()
Table 2
Outcomes of pediatric out-of-hospital cardiac arrest
Values are presented as number (%).
ROSC = return of spontaneous circulation, PCPC = pediatric cerebral performance category.
aBonferroni-adjusted two-sided significance level is P < 0.008. Groups 1 and 3, and groups 1 and 4 differed significantly.
bWhen using Bonferroni-adjusted P < 0.008, no pairwise comparisons among groups were significant.
![]()
Logistic regression
The model used for multivariate analysis contained variables that were significant in univariate analysis or were important according to the opinions of researchers: age, sex, weekday or weekend event occurrence, past medical history, etiology, location of OHCA, first responder type, bystander CPR, prehospital delivery of AED shock, initial ECG rhythm at ED and defibrillation at ED. Multivariate analyses by age group were also performed and are presented as Supplementary Tables 1, 2, 3, 4.
Multivariate analysis
The odds ratio (OR) for survival to discharge with group 1 as the reference was 0.55 (CI, 0.37–0.82) in group 3 (Table 3). The values in the other age groups were not significant. For etiology, cardiac disease was the reference for analysis. The OR for ROSC was 1.86 (CI, 1.43–2.43) for choking, 0.51 (CI, 0.38–0.70) for falls, and 0.36 (CI, 0.27–0.48) for SUID. The OR for survival to discharge was 0.23 (CI, 0.10–0.54) for traffic accident, 0.17 (CI, 0.08–0.35) for falls, and 0.11 (CI, 0.06–0.20) for SUID. The OR for good neurologic outcome was 0.24 (CI, 0.09–0.62) for falls, 0.23 (CI, 0.05–0.94) for traffic accident, and 0.06 (CI, 0.02–0.18) for SUID.
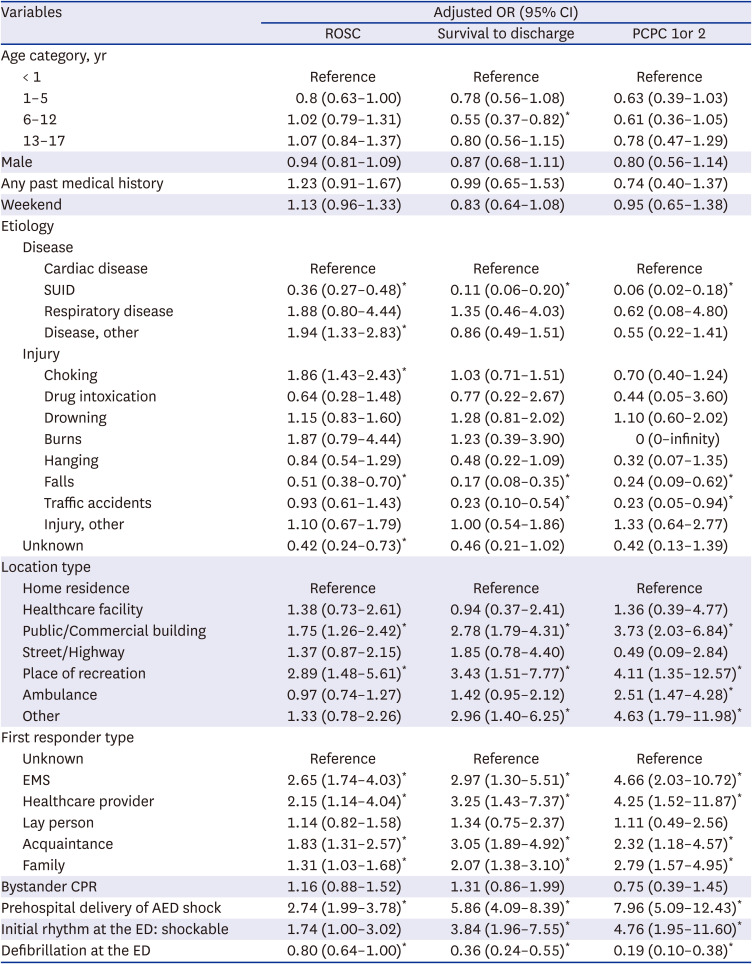
Table 3
Multivariate analysis for factors associated with ROSC, survival to discharge, and good neurologic outcome
OR = odds ratio, CI = confidence interval, ROSC = return of spontaneous circulation, PCPC = pediatric cerebral performance category, SUID = sudden unexpected infant death, EMS = emergency medical service, CPR = cardiopulmonary resuscitation, AED = automated external defibrillator, ED = emergency department.
*P < 0.05.
![]()
With home residence as the reference OHCA location, the OR for ROSC following an OHCA in a place of recreation was 2.89 (CI, 1.48–5.61), and that following an OHCA in a public/commercial building was 1.75 (CI, 1.26–2.42). The OR of survival to discharge in a place of recreation was 3.43 (CI, 1.51–7.77), and that in a public/commercial building was 2.78 (CI, 1.79–4.31). The OR for good neurologic outcome following an OHCA in a public/commercial building was 3.73 (CI, 2.03–6.84), that in a place of recreation was 2.51 (CI, 1.47–4.28), and that in an ambulance was 4.63 (CI, 1.79–11.98).
When the reference for first responder type was unknown, the OR for ROSC was highest with EMS at 2.65 (CI, 1.74–4.03), followed by healthcare provider at 2.15 (CI, 1.14–4.04), acquaintance at 1.83 (CI, 1.31–2.57), and family member at 1.31 (CI, 1.03–1.68). The OR for survival to discharge was highest with a healthcare provider at 3.25 (CI, 1.43–7.37), followed by acquaintance at 3.05 (CI, 1.89–4.92), EMS at 2.97 (CI, 1.30–5.51), and family member at 2.07 (CI, 1.38–3.10). The OR for good neurologic outcome was highest with EMS at 4.66 (CI, 2.03–10.72), followed by healthcare provider at 4.25 (CI, 1.52–11.87), family member at 2.79 (CI, 1.57–4.95), and acquaintance at 2.32 (CI, 1.18 – 4.57).
With prehospital delivery of AED shock, the OR for good neurologic outcome was 7.96 (CI, 5.09–12.43), that for survival to discharge was 5.86 (CI, 4.09–8.39), and that for ROSC was 2.74 (CI, 1.99–3.78). With an initial shockable rhythm at the ED, the OR for good neurologic outcome was 4.76 (CI, 1.95–11.60), and that for survival to discharge was 3.84 (CI, 1.96–7.55). With defibrillation at the ED, the OR for ROSC was 0.80 (CI, 0.64–1.00), that for survival to discharge was 0.36 (CI, 0.24–0.55), and that for good neurologic outcome was 0.19 (CI, 0.10–0.38).
Multivariate analysis of group 1
The OR for ROSC was 0.71 (CI, 0.54–0.93) in males (Supplementary Table 1). With an etiology of SUID, the ORs for ROSC, survival to discharge, and good neurologic outcome were 0.35 (CI, 0.25–0.48), 0.08 (CI, 0.04–0.16), and 0.06 (CI, 0.02–0.20), respectively. With an etiology of drowning, the OR for good neurological outcome was 4.95 (CI, 1.17–20.91). With healthcare facility as the location, the OR for ROSC was 3.09 (CI, 1.02–9.34). The OR for ROSC was highest when EMS was the first responder, 9.44 (CI, 2.46–36.29), followed by acquaintance at 3.26 (CI, 1.20–8.88). The OR for survival to discharge was highest when an acquaintance was the first responder, 19.60 (CI, 4.35–88.19), followed by EMS at 11.39 (CI, 1.91–67.98). However, neither of those variables was significant for good neurologic outcome.
Multivariate analysis of group 2
When the etiology was choking, the OR for ROSC was 2.94 (CI, 1.77–4.89), and when the etiology was traffic accident, the OR for survival to discharge was 0.16 (CI, 0.04–0.72) (Supplementary Table 2). The OR for survival to discharge was highest when the event location was a place of recreation, 8.41 (CI, 2.07–34.07), followed by street/highway at 4.95 (CI, 1.10–22.35), and public/commercial building at 3.01 (CI, 1.20–7.53). The OR for good neurological outcome was also highest when the event location was a place of recreation, 14.19 (CI, 2.09–96.53), followed by an ambulance at 4.25 (CI, 1.10–16.45). When the first responder was family, the OR for survival to discharge was 2.84 (CI, 1.34–6.02). When the first responder was a healthcare provider, the OR for good neurological outcome was 29.81 (CI, 1.97–452.09), and when it was family, the OR was 11.03 (CI, 2.33–52.18). With prehospital defibrillation, the OR for ROSC was 2.70 (CI, 1.03–7.06). With defibrillation at the ED, the OR for survival to discharge was 8.01 (CI, 1.66–38.63).
Multivariate analysis of group 3
When the etiology was choking, the OR for ROSC was 2.41 (CI, 1.05–5.55) (Supplementary Table 3). When the event location was a place of recreation, the OR for ROSC was 4.35 (CI, 1.16–16.24), and when it was a public/commercial building, the OR for survival to discharge was 4.11 (CI, 1.24–13.64). When the first responder was an acquaintance, the OR for ROSC was 2.64 (CI, 1.28–5.45). When the first responder was EMS, the OR for survival to discharge was 5.59 (CI, 1.24–25.25), and the OR for good neurological outcome was 8.88 (CI, 1.59–49.60). With prehospital defibrillation, the ORs for survival to discharge and good neurologic outcome were 5.91 (CI, 2.61–13.36) and 12.24 (CI, 4.23–35.38), respectively. With the initial shockable rhythm at the ED, the OR for survival to discharge was 8.55 (CI, 1.22–59.69), and with defibrillation at the ED, the OR for survival to discharge was 10.50 (CI, 2.40–46.01).
Multivariate analysis of group 4
With an etiology of choking, the ORs for ROSC and survival to discharge were 4.62 (CI, 1.99–10.70) and 3.16 (CI, 1.36–7.33), respectively (Supplementary Table 4). With an etiology of falls, the ORs for ROSC, survival to discharge, and good neurologic outcome were 0.32 (CI, 0.20–0.52), 0.16 (CI, 0.06–0.43), and 0.10 (CI, 0.02–0.48), respectively. When the event location was a public/commercial building, the ORs for ROSC, survival to discharge, and good neurological outcome were 2.14 (CI, 1.19–3.85), 3.40 (CI, 1.52–7.57), and 4.64 (CI, 1.47–14.60), respectively. When the event location was an ambulance, the ORs for survival to discharge and good neurologic outcome were 2.60 (CI, 1.20–5.65) and 3.94 (CI, 1.29–12.02), respectively.
When the first responder was an acquaintance, the ORs for ROSC, survival to discharge, and good neurologic outcome were 1.74 (CI, 1.07–2.86), 2.95 (CI, 1.50–5.79), and 2.59 (CI, 1.00–6.71), respectively. When the first responder was family, the ORs for survival to discharge and good neurologic outcome were 2.19 (CI, 1.03–4.67) and 2.03 (CI, 0.67–6.18), respectively.
With prehospital defibrillation, the ORs for ROSC, survival to discharge, and good neurologic outcome were 3.39 (CI, 2.12–5.42), 8.83 (CI, 5.24–14.87), and 12.73 (CI, 6.42–25.25), respectively. With the initial shockable rhythm at the ED, the OR for survival to discharge was 3.78 (CI, 1.38–10.37), and the OR for good neurological outcome was 7.12 (CI, 1.57–32.37). With defibrillation at the ED, the OR for survival to discharge was 2.46 (CI, 1.33–4.54), and the OR for good neurological outcome was 11.29 (CI, 3.60–35.45).
DISCUSSION
This study is the most recent nationwide OHCA study to investigate pediatric patients across a 10-year period using detailed variables and clinical outcomes. Although the population of all pediatric age groups has decreased during the past 10 years, the IR of OHCA has decreased in groups 2 and 3 and increased in groups 1 and 4 (Fig. 1). Furthermore, the clinical outcomes have not improved in any of the pediatric groups (Fig. 3). We found significant differences between age groups in IR, etiology, and clinical outcomes. Cardiac arrest on a weekend, at a public/commercial building or place of entertainment, first responder type, prehospital delivery of an AED shock, initial shockable rhythm at the ED, and defibrillation at the ED were all associated with survival to discharge.
Over 10 years, the IR of OHCA has decreased in groups 2 and 3 but increased in groups 1 and 4 (Fig. 1). Looking at the trend over 10 years, all clinical outcomes of overall pediatric groups were not improved over 10 years (Fig. 3). The survival to discharge rate in groups 1 and 2 deteriorated slightly, and that in groups 3 and 4 improved slightly. Group 4 showed the most favorable outcomes in terms of ROSC, survival to discharge, and good neurological outcomes, which is consistent with previous nationwide studies (Table 2).3334 Group 4 also had good prognostic factors, such as prehospital AED shock, initial shockable rhythm at ED, and a higher likelihood that the OHCA occurred in a public location (Table 1).35 The poorer prognosis of group 1 might be because children younger than 1 year have less physiological reserve and increased vulnerability to cardiac arrest compared with older children.3637
In group 1, SUID accounted for more than 50% of all cases and is related to poor survival outcomes (Table 1). Most cardiac arrests in group 1 occurred at home (80.2%) and most first responders were family members (81.6%). SUID occurs during unobserved sleep and is not recognized early.38 Therefore, the median time between the last normal time and the arrival in the ED was 104 minutes, longer than in the age groups. Moreover, prehospital defibrillation was conducted in only 0.8% of the patients in age group 1. These findings suggest that parents recognized their infant’s cardiac arrest long after it happened, which could have contributed to the low survival rate in group 1. Therefore, it is important to monitor infants at high risk for SUID and to teach parents to place their infants in a supine position on a firm surface to sleep and get regular check-ups for their baby.39 It is also important to teach parents the early sign of cardiac arrest, EMS activation and bystander CPR, which are crucial elements in the chain of survival.1340
Choking was the etiology for 12% of the OHCAs in group 1 and 9.6% of those in group 2. Choking correlated with a relatively good ROSC rate and is generally preventable by caregivers (Table 3).41 Guardians for children in these age groups should learn how to prevent suffocation and cope with choking accidents through training in the Heimlich maneuver.
In group 2, the influence of disease on OHCA decreased, and the influence of injury increased (Table 1). Traffic accident as a cause increased remarkably and was related to poor survival (Table 3). Group 2 is an age group with high physical activity and a poor understanding of safety, so the attention of a guardian is necessary.
In group 3, more than 50% of OHCAs were due to injury, primarily traffic accidents and drowning (Table 1). Because OHCAs caused by safety accidents occurred remarkably often in group 3, safety education for elementary school students needs to be strengthened, and parents need pay attention when their children ride bicycles, kickboards, or play in the water.
In group 4, falls accounted for 23.4% of OHCAs, the most common injury cause in this group (Table 1). Falls correlated with poor ROSC, survival to discharge, and neurologic outcomes (Table 3). Although intentionality was not considered in this study, falls might be related to suicide, which is the leading cause of death among people aged 10 to 29 in Korea.42 Therefore, prevention of cardiac arrest needs to include suicide prevention strategies.
Overall, OHCAs that occurred in public places such as a public/commercial building or place of recreation had good survival outcomes (Table 3). When the first responder was EMS, a healthcare provider, or an acquaintance, patients showed a better survival to discharge rate than when family members were the first responders. The bystander CPR rate was 8.6–9.1% in our study, which is higher than the 2.9% reported in the 2006–2007 KOHCAR (Table 1).6 Bystander CPR correlated with a good survival to discharge rate, but the association was not significant (Table 3).
Most cardiac arrests in group 1 occurred at home (80.2%), the first responders were mostly family members (81.6%), and the bystander CPR rate was low (Table 1). The poor outcomes in this age group could be due to the etiology of SUID. Also, strong emotional stress and failure to recognize the signs of death might have complicated family members’ initial resuscitative efforts.34
Age groups 2, 3, and 4 showed better survival outcomes when the OHCA occurred in a public place than at home, though stratified analyses showed variations among age groups (Supplementary Tables 2, 3, 4). Group 2 is the age group most likely to be sent to childcare and educational facilities away from their families, so the rate of OHCAs at home decreased.43 As physical activity increases in this age group, awareness of the OHCA situation is faster, and the survival outcomes were good even when the first responder was a family member (Supplementary Table 2).
From group 1 to group 4, the proportions of patients with prehospital delivery of AED shock, initial shockable ECG rhythm at ED, and defibrillation at ED increased (Table 1). In other words, a shockable ECG rhythm and high-quality CPR using AED increased with age. It is known that a shockable ECG rhythm is a good prognostic factor in cardiac arrest.44 Prehospital delivery of AED shock in groups 3 and 4 correlated with good survival to discharge and good neurologic outcomes in our study (Supplementary Tables 3 and 4). Also, a shockable ECG rhythm and defibrillation at the ED correlated with a good survival to discharge rate in groups 3 and 4.
The main limitation of this study is its retrospective observational nature. Therefore, it can show associations but not establish causal relationships and there is a limitation to the analysis by each variable. Second, only OHCA cases reported to emergency services were analyzed in this study; cases transferred to a hospital without calling for an ambulance were not included. Third, because the data used in this study were collected from hospital medical records, we could not control for incomplete or inaccurate records. Because survival outcomes for transferred patients have been recorded only since 2015, all data for transferred patients had to be excluded. Nonetheless, we did our best to maintain the quality of the data. Fourth, the time-related information recorded in the records is insufficient for analysis. The KOHCAR data contain the arrest time, EMS call time, ED arrival time, defibrillation time, and CPR end time. To evaluate the response time and time on-scene, which could be used to improve EMS in the Republic of Korea, the on-site arrival time and on-site departure time should also be included in the KOHCAR data.
In conclusion, this study reports comprehensive trends in pediatric OHCA in Republic of Korea. Our findings imply that preventive methods for the targeted population should be customized by age group because factors important in cardiac arrest differ by age.
 XML Download
XML Download