

 PDF
PDF Citation
Citation Print
Print




INTRODUCTION
The current roles of infectious disease (ID) specialists are diverse, including diagnosis and treatment of various IDs, infection control, antibiotic stewardship, response to disease outbreaks, and vaccination. The social need for ID specialists is higher than ever because of the emergence of antimicrobial-resistant pathogens and recurrent outbreaks caused by emerging IDs. In particular, the spread of coronavirus disease 2019 (COVID-19) has affected more than 150 million people worldwide—including more than 128,000 people in Korea—since January 2020. This has created demand for ID specialists.12 Unfortunately, the number of ID specialists in several countries is suboptimal, and the number of applicants into ID training programs is insufficient.3456
In 2019, there were 242 active adult ID specialists in Korea, representing 0.42/100,000 of the population. One ID specialist in Korea was in charge of 342 hospital beds, which was higher than that in other countries, including the US, Europe, and Brazil.3467 Experienced ID specialists improve clinical outcomes. Direct system level improvements through infection and antimicrobial stewardship subsequently enhance patient satisfaction while optimizing the overall quality of care. However, the shortage of ID specialists can lead to unfavorable public health outcomes, including the emergence of a number of antibiotic-resistant bacteria89 and poor response to ID epidemics.10 Additionally, the shortage can lead to long work hours and low job satisfaction among ID specialists, leading to few applicants for ID specialist courses.1112
Recently, we analyzed the current working status and geographical distribution of adult ID specialists.3 However, there is limited information about the actual scope of work and time spent relative to their responsibilities. This study aimed to analyze the areas of practice and time spent in each area among adult and pediatric ID specialists in Korea and to identify commonly encountered problems and propose solutions from the perspective of ID specialists.
METHODS
Study design and population
A survey was conducted on December 17–27, 2020, targeting all adult and pediatric ID specialists (N = 392) in Korea. At the time of the survey, 40 experts that were either retired or had passed away were excluded. In total, 352 ID specialists (281 adult ID physicians and 71 pediatric ID specialists) were identified as potential participants in the survey. An online-based survey link was forwarded to them via text messages and e-mails by the office of the Korean Society of Infectious Diseases and the Korean Society of Paediatric Infectious Diseases. To encourage participation, we sent a reminder on the fifth day. The responders were anonymized, and only one response from each participant was accepted.
Survey items
Survey items included baseline characteristics of respondents (age, sex, marital status, number of children, and academic degree), type of working institution, job title, and practice area. Questions regarding the practice areas of ID specialists were divided into five categories: 1) clinical practices of outpatient care, inpatient care, and consultations; 2) infection control; 3) antibiotic stewardship; 4) research; and 5) education and training. The education and training area includes all kinds of lectures or training for students/residents or non-clinical position health care workers. All practices, except research, were based on activities conducted a year before the survey period (December 2019–November 2020). Meanwhile, research-related activities were based on the three years before the survey period (December 2017–November 2020). We determined that the sum of the weights for each expert’s clinical and research fields was 100%. Items related to job satisfaction were surveyed using a 5-point Likert scale. To determine compensation, we investigated vacation benefits and average annual income.
Weekly patterns of time use
Respondents selected one week (from Monday to Sunday) between November 2, 2020 and December 6, 2020, and chose activities they performed from 6 am to midnight. One of the nine activities was entered on an hourly basis: 1) outpatient care; 2) consultation; 3) inpatient care/rounding; 4) education/training; 5) research; 6) infection control; 7) antibiotic stewardship; 8) volunteer work; and 9) participation in conferences (except infection control meetings). Additionally, the start and finish times for a daily work period from Monday to Saturday were recorded to investigate the working hours in a week.
Statistical analysis
SPSS version 24.0 for Windows (IBM, Armonk, NY, USA) was used for statistical analysis. Chi-square or Fisher’s exact tests were used to compare categorical variables. Continuous variables were compared using the Student’s t-test or Mann-Whitney U test, as appropriate. Variables with P values < 0.05 were considered statistically significant.
RESULTS
Demographic characteristics of respondents
Overall, 195 (55.4%) ID specialists (144 adult ID specialists and 51 pediatric ID specialists) completed the survey. Detailed baseline characteristics are shown in Table 1. Majority of the respondents (192, 98.5%) worked in a clinical position. Most ID specialists (181, 92.8%) worked in acute-care referral hospitals, with two thirds of respondents (127, 65.1%) working in metropolitan areas (Supplementary Table 1).

Table 1
Main characteristics of ID specialists
Data are number (%) of patients, unless otherwise indicated.
ID = infectious disease, IQR = interquartile range.
aNon-clinical areas included pharmaceutical companies (n = 2) and a life science company (n = 1).
bOthers included pharmaceutical companies (n = 2), life science companies (n = 1), laboratories (n = 1), and medical schools (n = 1).
![]()
In total, 144 (73.8%) respondents were involved in all of the following practices: inpatient and outpatient care, consultation, infection control, antibiotic stewardship, research, and education/training. Adult ID specialists were more involved in the practices of consultation, infection control, antibiotic stewardship, and participation in the public sector (Table 1). The major areas of specialization were bacterial/viral infections and infection control (Fig. 1A).
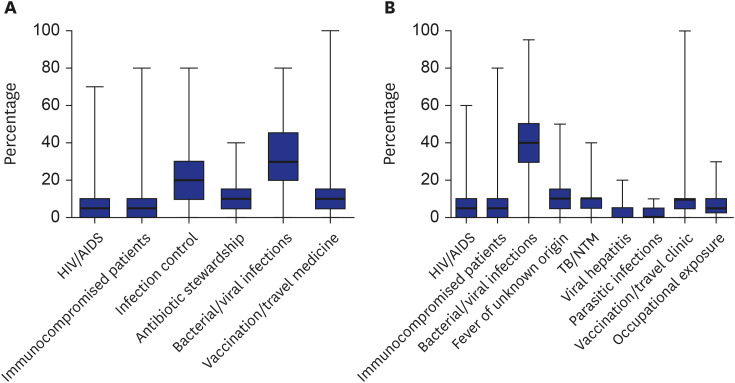
Fig. 1
Proportion of practice times (median hours and range) among infectious disease specialists by specialized areas (A) and clinical areas of practice (B). Data are presented as the median hours and range.
HIV = human immunodeficiency virus, AIDS = acquired immune deficiency syndrome, TB = tuberculosis, NTM = nontuberculous mycobacteria.
![]()
Clinical practices of the respondents
The most common area of clinical practice was bacterial/viral diseases, followed by fever of unknown origin, and immunocompromised infection (Fig. 1B, Table 2). Human immunodeficiency virus/acquired immune deficiency syndrome, parasitic infection, immunocompromised infection, and occupational exposure were more common among adult ID specialists. In contrast, pediatric ID specialists were more often involved in vaccination/travel clinics. The majority of ID specialists had 6–10 hospitalized patients per day (48.5%); 41.9% of adult ID specialists had 6–10 hospitalized patients, while 61.9% of pediatric ID specialists had fewer than five hospitalized patients per day. The number of patients per outpatient clinic was similar between adult and pediatric ID specialists, with the majority having 11–20 patients per section. A large percentage of adult ID specialists (29.6%) performed > 20 formal consultations per day, while the majority of pediatric ID specialists (76.7%) had < 5 formal consultations per day. The number of informal consultations per day was similar between the two groups. Consultations were conducted without assistive personnel for 73.0% of the respondents. Twenty-three percent of adult ID specialists participated in pediatric ID consultation, and 7.0% of pediatric ID specialists participated in adult ID consultation.

Table 2
Clinical practices of respondents
Data are number (%) of patients, unless otherwise indicated.
ID = infectious disease, IQR = interquartile range, HIV = human immunodeficiency virus, AIDS = acquired immune deficiency syndrome, TB = tuberculosis, NTM = nontuberculous mycobacteria.
aConsultation via formal paperwork.
bConsultation via informal communication (e.g., telephone, text messages).
![]()
Among 183 respondents, 131 (71.6%) answered that their institution took care of hospitalized patients with COVID-19, of whom 105 (80.2%) participated in COVID-19 care (Supplementary Table 2).
Infection control and antibiotic stewardship
Participation in infection control and antibiotic stewardship activities was more common among adult ID specialists (90.3% vs. 74.5%, P = 0.009) than among pediatric ID specialists (Table 1). Among 183 respondents participating in infection control activities, 96 (52.5%) had been an infection control team chair, with a median period of five years (interquartile range [IQR]: 2–10 years) (Supplementary Table 3). The most common infection control activities were attending infection control meetings (97.0%), responding to emerging ID (91.1%), and responding to unexpected exposure to transmissible diseases (88.7%). The most common antibiotic stewardship activities were review and approval of restricted antibiotics (81.5%), active monitoring of antibiotic prescription (51.8%), and review of surgical prophylactic antibiotics (42.8%).
Research
Overall, 164 (84.1%) respondents were involved in research, including clinical research (88.4%), basic research (19.2%), and research in public health/epidemiology (18.0%) (Supplementary Table 4). The main research interests of adult ID specialists were bacterial/viral infections (78.5%), infection control (40.8%), and antibiotic stewardship (27.7%), while those of pediatric ID specialists were bacterial/viral infections (85.7%), vaccination (59.5%), and immunocompromised patients (23.8%). Most respondents (90.2%) had published in Science Citation Index/Expanded (SCI/E) journals, and the median number of publications as the first or corresponding author to SCI/E journals within 3 years was three (IQR: 2–6). Of the ID specialists involved in research, 59.8% had acquired research funds. Detailed response results according to position (professor, clinician, or non-clinical position) are shown in Supplementary Table 5.
Education and training
Overall, 153 respondents (78.5%) were involved in education and training. The contents of education/training included ID (93.5%), antibiotics (75.9%), infection control (75.9%), and vaccination (58.2%) (Supplementary Table 6).
Weekly patterns of time use
In total, 153 (43.5%) ID specialists reported weekly patterns of time use. Detailed results are shown in Table 3. Weekly working hours were longer among adult ID specialists than among pediatric ID specialists (median: 59.0 vs. 55.0 hours from Monday to Friday, P = 0.005; median: 62.0 vs. 57.5 hours from Monday to Saturday, P = 0.015). Among activities, ID specialists spent the longest hours on patient care, especially outpatient services (median: 12 hours, IQR: 7–16 hours), followed by inpatient services (median: 10 hours, IQR: 6–13 hours) and consultation (median: 8 hours, IQR: 4–14 hours), altogether resulted in a median of 29 hours (IQR: 14–37 hours) each week. Adult ID specialists spent more time on consultation, infection control, and antibiotic stewardship, while pediatric ID specialists spent more time on outpatient services, research, and volunteer medical services.

Table 3
Weekly patterns of time use
![]()
Job satisfaction and compensations
Among ID specialists, 37.4% (n = 73) responded that they were satisfied with their current job. The percentage of respondents who answered positively to question whether they would select the ID major if they had to choose again was higher for the adult ID specialist group than for the pediatric ID specialist group (P = 0.004) (Supplementary Table 7). Factors for satisfaction as ID specialists were shown in the Supplementary Table 8. In a multivariable logistic analysis, characteristics with male gender and working area in Seoul, Incheon, or Gyeonggi-do were significantly associated with job satisfaction (Supplementary Table 8). Most ID specialists spent 5–10 days of vacation per year (52.5%), earning 4,479–89,572 USD per year (46.2%) (Supplementary Table 9). Respondents answered that the ideal number of hospital beds covered by one adult and pediatric ID specialist was 151–200 beds (30.8%) and 401–500 beds (30.3%), respectively (Supplementary Table 10).
Main problems and complaints
To foster ID specialty in Korea, ID specialists suggested that they should be appropriately compensated, especially for infection control or antibiotic stewardship activities (n = 91, 37.0%), and that additional ID specialists are necessary (n = 61, 24.8%). Respondents also suggested that the opinions of ID specialists should be respected and reflected in government policies (n = 34, 13.8%) (Supplementary Table 11).
DISCUSSION
In the present study, we found that most ID specialists in Korea spent longer time treating patients with IDs. Concurrently, they also participated in infection control, antibiotic stewardship, or education/training. They work for more than 60 hours weekly, which exceeded the 52 hours set legally by the government. Accordingly, the demands for ID specialists have been concentrated on appropriate compensation of their work and increase employment of ID specialists. Considering that the number of ID specialists in Korea is low, the promotion of ID training will not negatively affect the training system of other specialties.
Among the various roles of ID specialists, patient care is essential. Involvement of ID specialists in the care of patients with IDs results in reduced hospitalization rates, mortality, healthcare costs, and hospital stay.13141516 In this study, most ID specialists were engaged in several patient care activities, including inpatient and outpatient care and consultations in the same week. Furthermore, about one fourth of adult ID specialists were engaged in pediatric ID consultations. The diverse clinical responsibilities of the ID specialists may be due to shortage in ID staff.
Following the outbreak of the Middle East respiratory syndrome in medical institutions in 2015, the medical law in Korea was revised to strengthen the legal regulations for infection control personnel.17 Furthermore, since 2017, the Ministry of Health and Welfare has reimbursed medical institutions for infection prevention and management measures. However, for reimbursement, a hospital requires an ID doctor in charge of 300 hospital beds and doctors in charge of infection control to perform infection control duties for at least 20 h/week and complete 16 hours of training related to infection control.17 Consequently, infection control rounding has become a mandatory activity for ID specialists in Korean hospitals.18 However, the pattern of weekly time use among ID specialists shows limited room for additional infection control activities. Despite this workload, the majority of ID specialists had to undertake multiple responsibilities, including being director of infection control. This results to insufficient time for infection control activities.
Participation in antibiotic stewardship mainly focused on approval for specific and restricted antibiotics.19 Similar to other activities related to the ID specialty, antibiotic stewardship in Korean hospitals is mostly conducted by one or two ID specialists.19 However, for more comprehensive ID activities, approximately 3.01 personnel are required per 1,000 beds.20 An increase in the emergence of antimicrobial-resistant pathogens emphasizes the importance of appropriate antibiotic use and antibiotic stewardship programs.21 Securing ID specialists is necessary to implement and expand the antibiotic stewardship program in Korean hospitals.
According to our results, ID specialists devoted similar amounts of time to research and patient care. This may be because a large proportion of ID specialists were stationed at university-affiliated hospitals. However, they were unlikely to receive research funds and perform basic research in their early careers. Given that a rapid response to emerging infectious and re-emerging diseases is enhanced by a strong research base22 promoting ID research is necessary to strengthen public health control efforts. Besides expanding ID research funds, emphasizing basic research in ID training courses should be considered.23 Promoting research in ID will most likely attract more applicants for training in ID specialties.24
Unfortunately, the actual time that ID specialists allocated to education and training activities was 3 hours per week. This duration may be insufficient for providing adequate educational opportunities. Due to the increase in emerging IDs and IDs caused by antimicrobial-resistant pathogens, it is important to educate students/trainees and healthcare personnel on infection control. An adequately staffed ID workforce is necessary to achieve this.
ID specialists worked an average of 60.5 hours per week. Given that more than half of the respondents were women and more than two thirds were married and had children, one can expect that it is difficult for ID specialists to achieve an appropriate work-life balance. In our previous survey,11 only 8.7% of ID specialists responded to having a work-life balance. In this study, working hours were based on work and leave hours. Only 2.6% answered that they did not carry work at home. It is known that long working hours can lead to health risks, including an increased risk of stroke.25
Interestingly, this study revealed differences between adult and pediatric ID specialists. Adult ID specialists had a greater role in consultation, infection control, and antibiotic stewardship than pediatric ID specialists. Although, the satisfaction level was similar between the two types of experts, pediatric ID specialists responded more positively to reselecting the same major. It is estimated that more weekly working hours for adult ID specialists may be the cause of the reselection factor; however, further studies should be conducted in this regard.
The strength of our study is the high response rate; 55.4% of ID specialists participated in the study. Therefore, the results may adequately represent the status of ID specialists in Korea. Nonetheless, this study had some limitations. First, clinical microbiologists who can be classified as ID specialists were not included in the study. Second, the survey was conducted in the middle of the COVID-19 pandemic, which may have affected the operational times of ID specialists. Third, there could be information or selection bias due to non-response and questionnaire-based, cross-sectional study design. Further studies with more meticulous designs such as longitudinal or repeated cross-sectional studies are needed to guarantee a more reliable data.
We identified areas of practice and patterns of time use among adult and pediatric ID specialists in Korea. Even during the middle of the COVID-19 pandemic, most experts oversee all necessary areas (e.g., treatment, education, research, infection control, and antibiotic stewardship) in medical institutions with limited resources. It is expected that these problems can be solved by appropriately compensating individuals and medical institutions for their invisible activities (including infection control and antibiotic stewardship) and by securing additional human resources.
 XML Download
XML Download