

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Humidifier disinfectant-related lung injury (HDLI) and pulmonary fibrosis have been reported in Korea since early 2006 and initially presented as an epidemic of acute interstitial pneumonia of unknown cause in pediatric and peripartum patients.123456 Subsequently, individuals exposed to guanidine-based components of HDs, such as polyhexamethylene guanidine (PHMG), oligo (2-[2-ethoxy]ethoxyethyl) guanidinium chloride (PGH), 5-chloro-2-methyl-4-isothiazolin-3-one (CMIT), and 2-methyl-4-isothiazolin-3-one (MIT), have been linked to not only rapidly progressing severe interstitial lung disease with fibrosis but also upper and lower airway diseases, including asthma.78 Patients with HDLI or HD exposure with normal chest imaging findings can develop asthma symptoms.9 Prevalence of asthma treatment among school children with a history of bronchiolitis was found to be higher for those with HD exposure before the age of 3 years than for those without HD exposure.10 To mitigate the injury caused by HD, a notice on the health damage and recognition criteria of HDs was partially revised by Korea Environmental Industry & Technology Institute (KEITI). An investigation on asthma, induced or exacerbated by HDs, conducted by the Humidifier Disinfectant Damage Relief Committee identified 331 South Korean residents with HD-associated asthma (HDA) as of July 31, 2019.11
Exposure to guanidine-based components of HDs may induce irreversible airway obstruction, causing wheezing without bronchial hyperresponsiveness. It may present as mild irritant-induced lung injury or subacute irritant-induced asthma, which remains poorly characterized.1213 Further, chronic exposure to moderate levels of HD can induce delayed-onset irritant-related asthma, and its prevalence may therefore be underestimated. Since the sale of HDs was suspended in South Korea in November 2011, no new cases of HDLI have been detected, with a subsequent decrease in the prevalence of asthma,1415 suggesting a correlation between HD use and induction of asthma.
The diffusing capacity of the lung for carbon monoxide (DLCO) is a measure of gas transfer from inspired gas to red blood cells. A pulmonary function test (PFT) study of 39 patients with HDLI showed reduced forced vital capacity (FVC) and DLCO that were representative of restrictive ventilatory disorders. However, FVC recovered to normal in 54% of these patients, with a return of mean FVC (% predicted) values to a normal range, whereas the mean DLCO remained low during follow-up.16 DLCO may thus indicate irreversible lung injury or loss of an effective alveolar gas exchange unit. Since there is no evidence of lung parenchymal abnormalities on the chest computed tomography (CT) scan in HDA, its diagnosis may be based only on asthmatic symptoms after HD exposure and decreased DLCO.
We hypothesized that the pathogenesis of HDA differs from that of typical asthma, leading to differences in the pulmonary function characteristics, including DLCO, between the two diseases. Therefore, we compared the DLCO of patients with HDA to that of asthmatic patients without prior HD exposure. Second, we assessed whether the reduced DLCO in HDA was related to the degree of exposure and several other categorical variables through environmental exposure questionnaires.
METHODS
Study subjects
In South Korea, asthmatic patients with confirmed exposure to HD are diagnosed with HDA based on the criteria established by the Ministry of Environment (Notice No. 2018-166).17 Briefly, HDA is diagnosed when 1) a patient with no history of asthma is diagnosed or treated for new asthma either during HD exposure or within two years of cessation of exposure or 2) a patient with pre-existing asthma experiences aggravated asthma symptoms during HD exposure and when other causes for asthma have been excluded.17
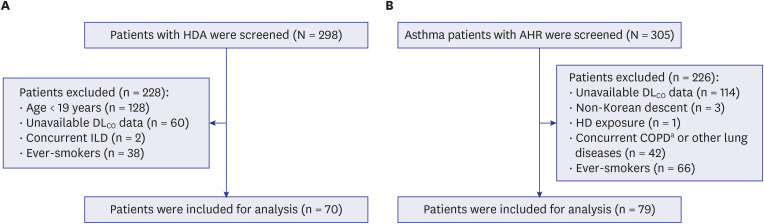
Seventy-nine asthmatic patients without exposure to HD and whose airway hyperresponsiveness (AHR) was demonstrated by a positive bronchial provocation test (BPT) at one hospital (Ulsan University Hospital, Ulsan) were recruited between 2014 and 2019 after applying the following exclusion criteria: age < 19 years, unavailability of DLCO data, concurrent interstitial lung disease (ILD), or history of smoking (Fig. 1). These patients had undergone PFT in accordance with the standard guidelines of the American Thoracic Society/European Respiratory Society (ATS/ERS),1819 and BPT-positivity was defined as 20% reduction in the forced expiratory volume in one second (FEV1) during the methacholine provocation test, with a value less than 16 mg/mL, or a 15% reduction in FEV1 during the Aridol provocation test (≤ 635 mg).202122
Fig. 1
Flow chart for the selection of study subjects. (A) Selection of patients with humidifier disinfectant-associated asthma. (B) Selection of asthma patients without exposure to humidifier disinfectant.
HDA = humidifier disinfectant-associated asthma, DLCO = diffusing capacity of the lung for carbon monoxide, ILD = interstitial lung disease, AHR = airway hyperresponsiveness, HD = humidifier disinfectant, COPD = chronic obstructive pulmonary disease.
aCOPD (n = 11), partial resections of the lung (n = 4), advanced lung cancer (n = 1), advanced esophageal cancer (n = 2), lung metastasis (n = 2), history of radiation treatment for breast cancer (n = 1), suspected acute pneumonia (n = 6), pulmonary tuberculosis sequelae (n = 2), cystic fibrosis (n = 1), pleural adhesion (n = 3), pulmonary edema or pleural effusion (n = 2), pneumothorax (n = 1), severe bronchiectasis (n = 3), and Churg-Strauss syndrome (n = 3).
Data collection
We obtained data on individuals with lung disease (HDLI and HDA) who claimed that their symptoms were related to the use of HD from KEITI. The claimants were clinically examined by the Humidifier Disinfectant Damage Relief Committee, and 298 patients with HDA were identified as of December 26, 2018. We used the medical records of individuals with HDA to collect information on their age, sex, weight, and height at the time of PFT testing, FVC results, FEV1, forced expiratory flow between 25% and 75% of vital capacity (FEF25-75), DLCO, total lung capacity measured by body plethysmography, residual volume, BPT, and chest CT findings. Information regarding environmental exposure, environmental exposure indicators, and tobacco smoking history was collected from questionnaires filled out by each participant. We collected the same information in known asthmatic patients without alleged exposure to HD through a retrospective review of their medical records and chest CT findings at Ulsan University Hospital.
The seven indicators of HD exposure, including daily usage time of a humidifier, cumulative usage time, usage time during sleep, distance from the humidifier, spray direction of humidifier, exposure concentration (HD concentration of used products × daily usage count × amount of single usage × 100,000/volume of the room with humidifier), and exposure intensity (cumulative usage time × exposure concentration), were collected using a questionnaire. The threshold criteria for satisfaction of each indicator were set as follows: at least 10 hours of daily usage time, an above-average cumulative usage time, not less than four hours of usage time during sleep, not more than a 1-m distance from the humidifier, spray direction of humidifier being oriented toward the face including nose and mouth, a higher-than-average exposure concentration, and a higher-than-average exposure intensity.
At KEITI, the exposure level assessment was conducted when a response for at least 4 of the 7 detailed exposure indicators was given, but failure to report on more than 3 items, the exposure was considered “indeterminate.” The exposure indicators with responses meeting the respective threshold levels were assessed as “satisfied.” If “satisfied” was recorded for not less than 75% of the exposure indicators, the exposure was classified as “definite.” If “satisfied” was recorded for 50% higher but less than 75% of the exposure indicators, the exposure was considered “probable,” and if “satisfied” was recorded for less than 50% of the exposure indicators, the exposure was considered “possible.” In this study, the exposure was broadly classified as “definite” and “non-definite” (probable + possible + indeterminate exposure).
Measurement
Since some hospitals in South Korea use different equations for predicted DLCO values, we recalculated the predicted DLCO and DLCO% using Park’s Korean equation.23 Previous studies have shown that Park’s equations for calculating the predicted DLCO are suitable for DLCO prediction in Koreans as compared to using foreign reference equations.2425 DLCO% was calculated by dividing the measured value by the predicted value. If the measured DLCO was reported in mmol/min/kpa units (SI unit), we converted it into mL/min/mmHg by multiplying the value with a factor of 2.987.18 A Korean reference equation (Choi’s equation)26 was used to predict the spirometry data values. A foreign European Community for Steel and Coal (ECSC) equation27 was used to calculate lung volume because a reference equation for Korean lung volume has not yet been developed, and the ECSC equation showed the lowest sum of residuals in lung volume measurements as compared with other equations used to calculate the lung volume of individuals outside of Korea.24
Statistical analysis
A Student’s t-test was used to compare baseline characteristics and PFT results between individuals with HDA and those with asthma without exposure to HD. The χ2 tests were used to compare sex distribution and the proportion of individuals with decreased DLCO between groups with different exposure levels. Exposure differences across the three groups (definite, non-definite, and none) were compared through one-way analysis of variance (ANOVA), and the DLCO (% predicted) trend across the three groups was assessed by the Jonckheere-Terpstra test.
Multiple linear regression analysis was used to assess the association of DLCO with the exposure status or FVC after adjusting for body mass index (BMI) in non-smoking patients. Regression path analyses with Sobel test statistics were used to assess the significance of mediational effects of FVC between DLCO and exposure to HD.282930 Odds ratios (ORs) and their 95% confidence intervals (CIs) for having a reduced DLCO (< 80% predicted) were then calculated with exposure status after adjusting for BMI and reduced FVC (< 80% predicted). Correlation analyses were used in patients with HDA to measure the correlation between DLCO and indicators related to exposure to HD, such as daily usage time, cumulative usage time, usage time during sleep, distance from the humidifier, exposure concentration, and exposure intensity (cumulative usage time × exposure concentration).
SPSS version 24.0 for Windows (IBM Corp., Armonk, NY, USA) was used for all statistical analyses, with a P value < 0.05 considered to indicate statistically significant differences.
Ethics statement
Since the clinical data extracted from the clinical information retrieval system at the Ulsan University Hospital (Ulsan University Hospital Information of Clinical Ecosystem) were de-identified, the need for patient consent was waived (Institutional Review Board [IRB] No. UUH 2019-11-003).
RESULTS
Selection of exposure group (asthma group with HD exposure)
Of 298 patients screened for this study, 128 children (< 19 years old) and 60 individuals whose DLCO values were unavailable were excluded. Additionally, two patients with concurrent ILD (based on their chest CT findings) and 38 ever-smokers were excluded. A total of 70 patients were included in the HDA group (Fig. 1).
Selection of asthma group without HD exposure
Between 2014 and 2019, 305 adult asthma patients with AHR confirmed through BPT and visiting the respiratory clinic in Ulsan University Hospital were screened. Of them, we excluded 114 patients whose DLCO values were unavailable, three individuals of non-Korean descent, and one patient with a history of confirmed exposure to HD. We reviewed the patients’ medical records and chest scans taken at the time of the PFT. Based on the findings, we excluded 42 patients with other lung diseases that may affect DLCO
3132333435; 11 of these individuals had chronic obstructive pulmonary disease and 31 had other lung diseases (Fig. 1). We further excluded 66 patients with a smoking history due to the potential effect on DLCO,
3637 resulting in a total of 79 non-smoking patients with asthma in the control group (Fig. 1).
Comparison of baseline characteristics of asthma groups with and without exposure to HD
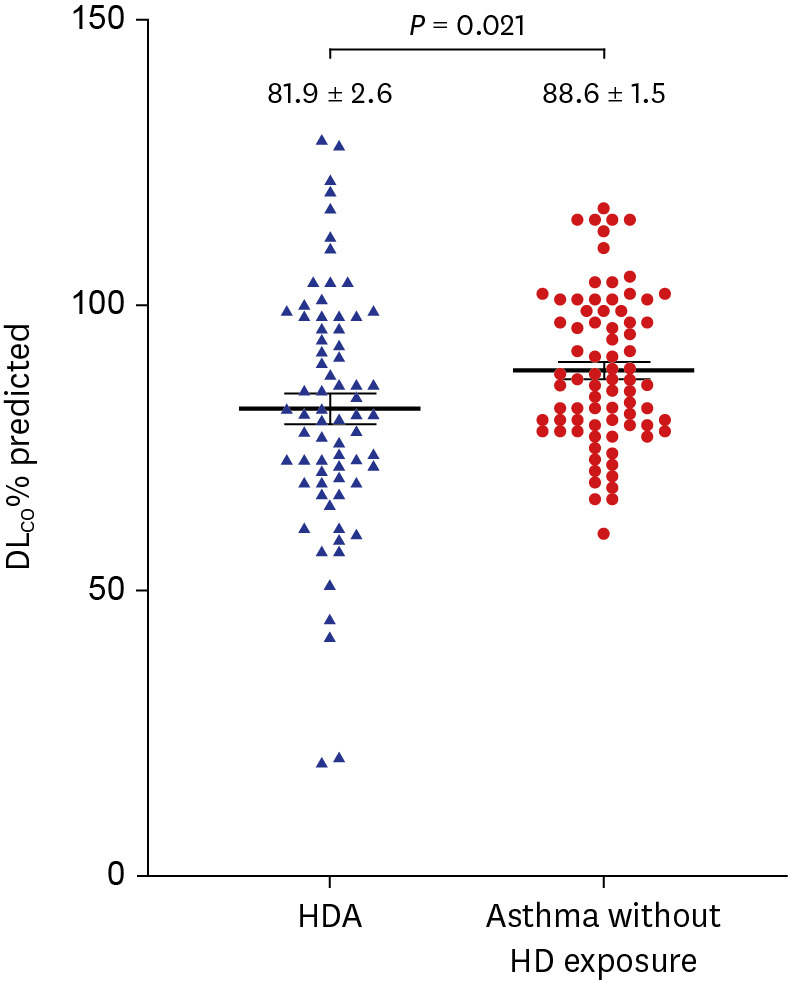
The asthma group without HD exposure showed a trend of being older but without statistically significant inter-group differences (46.6 ± 15.3 years vs. 51.8 ± 16.9 years; P = 0.051). Sex, BMI, and PFT results, including the FEV1%, DLCO/VA%, and RV/TLC% values, showed no difference between the two groups. The mean DLCO% (81.9% vs. 88.6%; P = 0.021) and FVC% (83.2% vs. 89.9%; P = 0.018) were significantly lower in the exposure group (Table 1, Fig. 2).
Table 1
Baseline characteristics of never-smoker asthma patients with and without exposure to HD
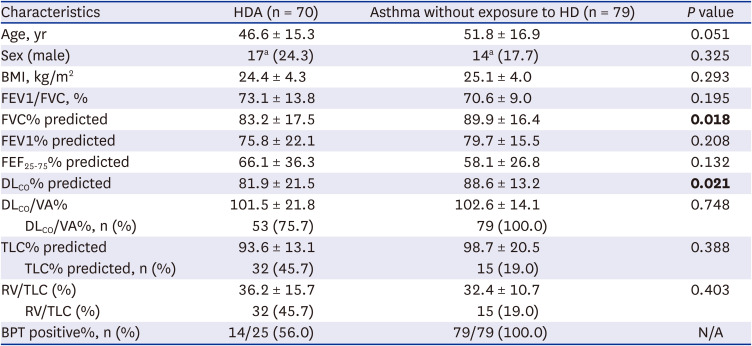
Data are presented as means ± standard deviation or absolute number (%). Bold font indicates statistical significance.
HD = humidifier disinfectant, HDA = humidifier disinfectant-associated asthma, BMI = body mass index, FEV1 = forced expiratory volume in one second, FVC = forced vital capacity, FEF25-75 = forced expiratory flow between 25% and 75% of vital capacity, DLCO = diffusing capacity of the lung for carbon monoxide, VA = alveolar volume, TLC = total lung capacity, RV = residual volume, BPT = bronchial provocation test, N/A = not applicable.
aNumber of patients with pulmonary function test results, i.e., number of patients who were able to obtain results.
Fig. 2
Comparison of the diffusing capacity between the HDA and asthma without HD exposure groups.
Plots indicate individual data points and mean ± standard error of DLCO% predicted (horizontal line and vertical bar). P value for Student’s t-test (P = 0.021).
DLCO = diffusing capacity of the lung for carbon monoxide, HDA = humidifier disinfectant-associated asthma, HD = humidifier disinfectant.
Comparison among asthma patients with different levels of exposure
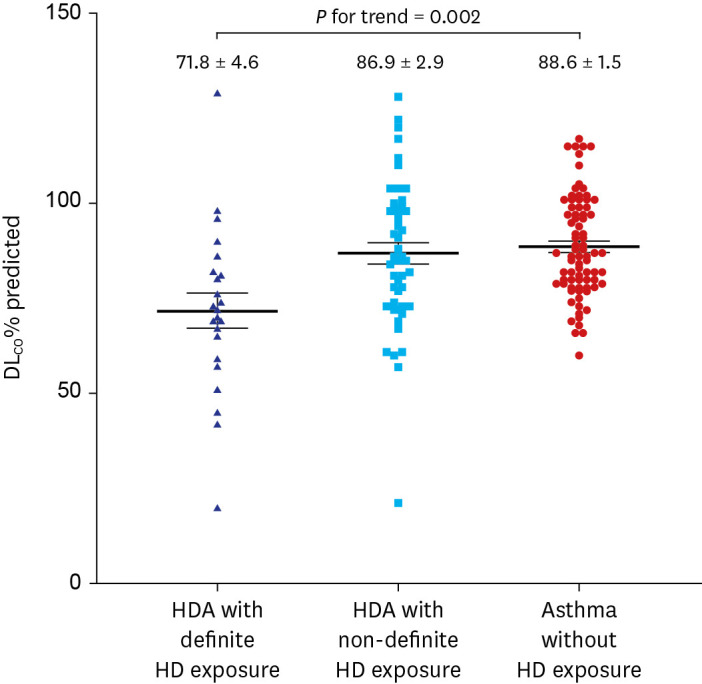
ANOVA indicated that the mean DLCO% of the non-exposure group, non-definite exposure group (probable + possible + indeterminate exposure), and definite exposure group were significantly different (P < 0.001) in a dose-dependent manner based on the Jonckheere-Terpstra test (P for trend = 0.002) (Fig. 3).
Fig. 3
Diffusing capacity of asthma patients with definite, non-definite, and no exposure to HD.
Plots indicate individual data points and mean ± standard error of DLCO% predicted (horizontal line and vertical bar). The P value for the trend was analyzed by Jonckheere-Terpstra test (P = 0.002). There was a statistical difference in the mean DLCO% of asthma patients with definite exposure (n = 23) and those with non-definite exposure group (probable + possible + indeterminate exposure, n = 47) (71.8 ± 21.9% vs. 86.9 ± 19.7%; P = 0.008 by Student’s t-test).
DLCO = diffusing capacity of the lung for carbon monoxide, HD = humidifier disinfectant.
Association of DLCO with exposure status and FVC
To evaluate the association between DLCO% and the exposure status through multiple regression analyses, after controlling for BMI, a beta coefficient and 95% CI were calculated in non-smoking patients with bronchial asthma. The beta coefficient value for the DLCO% in the HD exposure group versus the non-exposure asthma group was −5.831 (95% CI, −11.334 to −0.327) after adjusting for BMI, indicating that the DLCO% was significantly lower by 5.8% in the HDA group than that in the control group (Table 2).
Table 2
Multiple linear regression model for diffusing capacity by exposure status and BMI

| Independent variables | Beta coefficient (95% CI) | P value | R2 |
|---|---|---|---|
| Exposure to HD | −5.831 (−11.334 to −0.327) | 0.038 | 0.104 |
| BMI | 3.651 (0.566 to 1.903) | < 0.001 |
However, the significant effect of exposure status on DLCO% disappeared after adjusting for BMI and FVC% as covariates in the linear regression model (Table 3), suggesting that the effect of HD on DLCO% might be mediated in part by FVC loss.
Table 3
Multiple linear regression model for diffusing capacity by exposure status and BMI, FVC

| Independent variables | Beta coefficient (95% CI) | P value | R2 |
|---|---|---|---|
| Exposure to HD | −2.799 (−7.909 to 2.310) | 0.281 | 0.261 |
| BMI | 1.475 (0.862 to 2.087) | < 0.001 | |
| FVC% | 0.427 (0.411 to 5.656) | < 0.001 |
We performed a path analysis to investigate the mediation effect of FVC, where the results were shown with regression outputs and Sobel test statistics (Fig. 4). The proportion of the mediated effect was obtained using the following equation: indirect effect divided by total effect. The mediation proportion {(−7.091*0.444)/−5.831} was calculated to be 54% of the variance, indicating that the FVC was a significant partial mediator of the relationship between HD exposure and DLCO.
Fig. 4
Regression pathway analyses.
The proportion of the mediated effect is obtained by dividing the indirect effect by the total effect. Thus, the mediation proportion {(−7.091*0.444)/−5.831} is calculated to be 54% of the variance, showing that FVC was a significant partial mediator of the relationship between exposure and DLCO. The P values shown are for a one-tailed probability, after adjusting for body mass index.
DLCO = diffusing capacity of the lung for carbon monoxide, FVC = forced vital capacity.
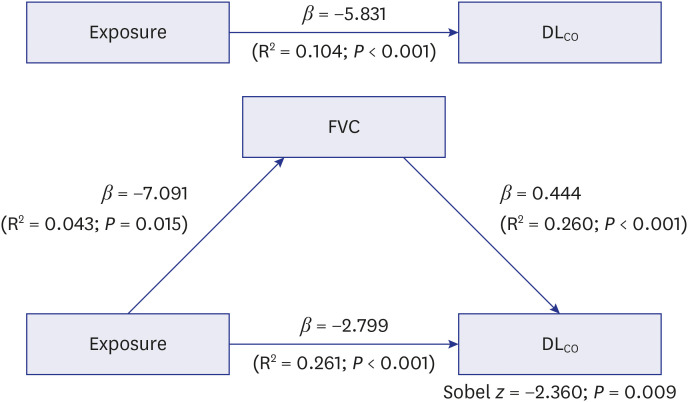
Table 4 presents the ORs and 95% CIs for the association between reduced DLCO and exposure status after adjusting for BMI and FVC% in non-smoking patients with bronchial asthma. Asthma patients exposed to HD were 2.1 times more likely to have reduced DLCO (OR, 2.127; 95% CI, 1.053 to 4.294). Patients with reduced FVC were 2.6 times more likely to have reduced DLCO (OR, 2.596; 95% CI, 1.217 to 5.539).

Analysis of DLCO within the HDA group
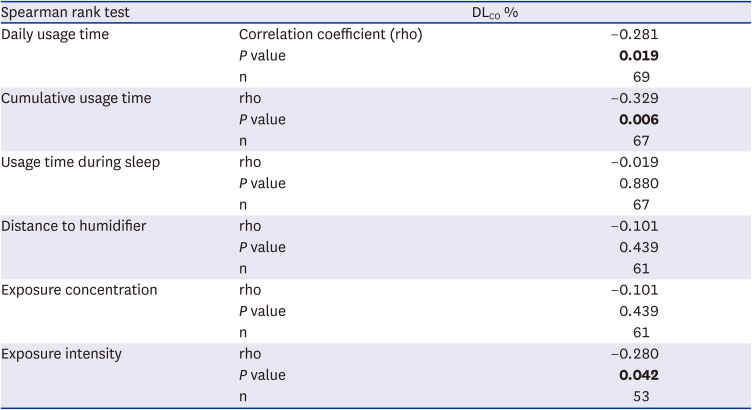
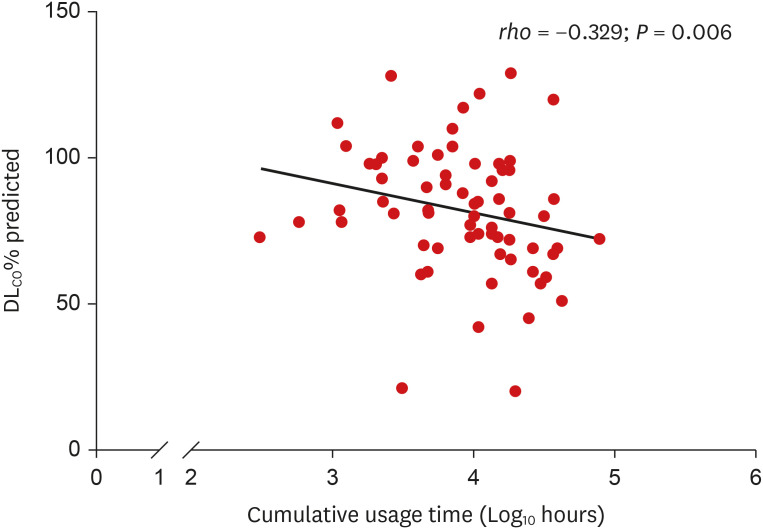
Definite, probable, possible, and indeterminate HD exposure accounted for 23, 20, 23, and 4 cases, respectively. The average DLCO% was 71.8% in definite exposure cases, 90.5% in probable cases, 81.5% in possible cases, and 100.3% in indeterminate cases. There was a statistical difference in the mean DLCO% of asthma patients with definite exposure (n = 23) and those with other exposure levels (probable + possible + indeterminate exposure, n = 47) (71.8% vs. 86.9%; P = 0.008) (Fig. 3). Further, there were statistically significant negative correlations between DLCO% and daily usage time of HDs, cumulative usage time, and exposure intensity. In particular, cumulative usage time had a stronger negative correlation with DLCO% (rho = −0.329, P = 0.006) than other exposure indicators (Table 5, Fig. 5).
Table 5
Correlation between DLCO and exposure indicators
DISCUSSION
The present study is the first to evaluate the differences between DLCO values of individuals with HDA and those of asthmatics without HD exposure and it showed that the HDA group had a significantly lower mean DLCO%. The mean DLCO% of asthma patients with definite exposure to HD was significantly lower than that of patients with other levels of exposure or no exposure in a dose-dependent manner. Further, after adjusting for BMI, the DLCO was lower by 5.8% in the HDA group with a 2.1-fold greater likelihood of HDA patients having a lower DLCO than that of asthmatic patients without exposure to HD. Additionally, DLCO% was inversely correlated with the daily usage time of HDs, exposure intensity, and particularly with the cumulative usage time. Taken together, these data suggest that the DLCO% values are indeed lower in HDA than in airway hyperreactive asthma, confirming our hypothesis.
The pathophysiology and lung function in HDA remain unclear; they differ from those in typical AHR asthma or allergic asthma but are similar to those in irritant-induced asthma caused by “moderate” levels of chronic irritant exposure.12 Asthma with prolonged exposure to low intensities of PHMG in early life is characterized by a lower FEV1 without an increase in AHR and atopy as compared to asthma without HD exposure.38 In an animal model, repeated exposure to low-dose PHMG was found to induce airway inflammation and hyperresponsiveness, with a significant increase in asthma-related histological findings; however, the characteristics of PHMG-altered gene expression patterns and airway inflammation differed from those of typical allergic asthma and was similar to those in irritant-induced asthma with Th2-low and Th17-mediated inflammatory responses.39 A previous study using a mouse asthma model demonstrated that exposure of the airways to PHMG caused aggravated AHR and lung inflammation via CCL11- and SERPINF1-induced signaling in mice. This suggests that PHMG exposure exacerbates asthma, and the underlying pathogenesis involves the profibrotic process rather than a typical allergic Th2 pathway.40 Two independent general population-based cohort studies showed that HD exposure in children can increase risk of asthma and worsen symptoms in patients with pre-existing asthma.10 Furthermore, CMIT/MIT, an HD component, can reduce the expiratory airflow in small airways.41 These prior studies provide a basis for HDA patients to be recognized as victims of HD use. However, there is a lack of HD-induced injury biomarkers, and additional indicators are necessary to assess lung abnormalities caused by HD exposure.
A previous study showed that HDLI patients had a restrictive physiologic pattern with decreased DLCO. Lung function returned to normal in 54% of these patients, with a return of the mean FVC (%) to within the normal range; however, the mean DLCO was persistently low at the 5-year follow-up.16 Thus, a reduced DLCO may be a potential marker of long-term lung injury. Typical asthmatic patients not associated with HD have normal or increased DLCO values if their symptoms are mild and airflow obstruction is not severe.4243 Although no clear mechanisms have been identified, the DLCO values may be attributed to increased lung volume and perfusion in the upper zones of the lungs with greater negative pressure in the chest cavity during inspiration.42 As such, normal or increased DLCO may become a distinguishing feature of asthma and other lung diseases, while reduced DLCO in asthmatic patients may be a clue to the coexistence of other lung diseases.4244 Based on this, DLCO is a potential indicator of lung injury caused by HD and may be associated with lower diffusing capacity in HDA. However, there are no previous reports on DLCO levels in HDA.
Previous studies have indicated that the finer particulate matter (aerodynamic diameters < 2.5 μm) responsible for lung parenchymal tissue remodeling with predominant pathological effects is confined to the epithelial and interstitial tissue compartments of the respiratory bronchioles.45 The respiratory bronchioles, which form the transitional zone between the conducting airways and gas exchange regions of the lungs, are well-established as a target of particulate-induced injury in occupational settings.46 Exposing 16 normal subjects to ultrafine particles (particles less than 0.1 μm in diameter) at a concentration of 50 μg/m3 caused a reduction in the maximal mid-expiratory flow rate and DLCO without evidence of airway inflammation.47 Based on these studies and the results of our study, we speculate that chronic exposure to 0.1-μm-sized HD aerosols48 vaporized by humidifiers can damage the interstitial tissue of respiratory bronchioles with tissue remodeling and/or alveolar-capillary injury, remaining undetected by chest CT and leading to DLCO and FVC reduction in HDA patients. Another possible mechanism is that long-term exposure to airway irritants, such as PHMG or CMIT/MITT, causes both chronic inflammation leading to small airway obstruction and fibrotic or other interstitial changes surrounding small airways, leading to the reduction of the lung diffusing capacity and FVC. Although pathological confirmation with lung tissue was beyond the scope of this study, it is plausible that the main target site of HD-related injury may be in the gas exchange regions of the lungs, including the interstitial tissue of respiratory bronchioles and small airways, rather than in the conducting airways. Moreover, pathway analysis suggested that exposure to HDs affects DLCO directly, and indirectly through FVC, meaning that most affected areas were respiratory bronchioles and the surrounding interstitial tissue. A prospective study assessing the presence of small airway dysfunction in HDA is necessary.
Our findings suggest that DLCO was lower in HDA than in asthma without HD exposure. Further, HD exposure was assessed quantitatively, and a graded association of DLCO change with the exposure level in a dose-dependent manner was identified.
This study has some limitations. First, the sample was relatively small. Further studies with more asthmatic patients with and without exposure are necessary to confirm our findings. Second, there may have been a selection bias inherent to the retrospective selection of asthmatic patients without exposure despite exclusion of patients with concurrent lung diseases that could have affected the DLCO through extensive review of medical and CT records. The DLCO of asthmatic patients without HD exposure may have been examined specifically to rule out any comorbid lung diseases causing a reduced DLCO. Although not statistically significant, the control group tended to be older, making it more likely to have other systemic diseases affecting DLCO. However, this bias may cause underestimation of the reduction in DLCO values in the HDA group as compared to asthma control group without HD exposure. In addition, hemoglobin correction was required as anemia or polycythemia can affect DLCO values18; however, the hemoglobin values were unavailable. In future studies, it will be necessary to record hemoglobin values and obtain the corrected DLCO%. Finally, the HD exposure status was determined retrospectively based on the medical records. Thus, there may be unidentified exposures in the control group. However, we excluded the possibility of exposure to HD in asthmatic patients as controls by reviewing the data of all registered claimants.
In conclusion, this study found that the DLCO was lower in HDA than in asthma without HD exposure. Thus, monitoring DLCO values in asthma patients with HD exposure may help in the early identification of HDA. For patients with history of HD exposure and persistent respiratory-related symptoms that cannot be explained by the clinical pattern or diagnostic criteria of HDLI, HDA should be considered as a differential diagnosis. Furthermore, a lower DLCO is a potential diagnostic criterion for confirming HDA, and revision of the existing criteria may be warranted.
 XML Download
XML Download