

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Chronic kidney disease (CKD), defined as reduced kidney function and decline in estimated glomerular filtration rate (eGFR), is a major global public health problem, affecting 10%–20% of adults in many countries of the world, and is a strong predictor of impaired survival, especially after vascular surgery [12]. CKD has been recognized as one of the risk factors that promote atherosclerosis as well as cardiovascular disease (CVD), up to half of the individuals with CKD die from CVD [3].
Abdominal aortic aneurysms (AAA) are defined as segmental, full-thickness dilations of the aorta resulting in a 50% increase in diameter, when compared with the normal aortic diameter. The natural history of aneurysm is characterized by a slow expansion with a concomitant raised risk of rupture. Ruptured AAA is a life-threatening condition that is estimated to lead to 150,000–200,000 deaths each year worldwide [4]. In South Korea, the prevalence of AAA has increased from 201 to 278 per million population; although the proportion of ruptured AAAs decreased from 8.6% to 7.3% in 2012 and 2016, respectively, it is still one of the major health care problems [5].
There are numerous studies investigating the association between decreased renal function and various subtypes of CVD, such as coronary artery disease, myocardial infarction (MI), heart failure, and stroke [6]; however, there are sparse data that demonstrate the impact of CKD on AAA, what was worse, most of them were cross-sectional study or small sample-sized study and yield conflicting results [78]. Therefore, this study using nationwide population cohort data was conducted to identify whether the advanced stage of CKD is risk factor for AAA development.
METHODS
The study was approved by the Institutional Review Board of The Catholic University of Korea, Bucheon St. Mary’s Hospital (No. HC22ZISI0017). Informed consent was not obtained because patient records and information were anonymized and deidentified prior to analysis. This study followed the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) reporting guideline for cohort studies.
Data source
This nationwide cohort study was performed using data from the National Health Insurance Service (NHIS), the only medical insurance system available that is managed by the Korean government. The NHIS system consists of 2 major healthcare programs for universal coverage of all Korean residents: NHIS and Medical Aid (MA). Approximately 97% of the population is covered by NHIS, and the remaining 3% is covered by MA [9]. NHIS contains all information claimed by medical service providers in Korea about offers a regular health checkup for all subscribers, which includes important medical parameters (e.g., body weight, height, body mass index [BMI], waist circumference, blood pressure, fasting glucose, lipid profiles, and creatinine level), social habits (e.g., alcohol consumption, smoking status, and physical activities), income level, and insurance claims. To protect individuals’ privacy, resident registration numbers were encrypted. Statements in the NHIS database are defined by the Korean Classification of Disease, 6th edition, and a modified version of the International Classification of Diseases, 10th edition (ICD-10).
Study populations
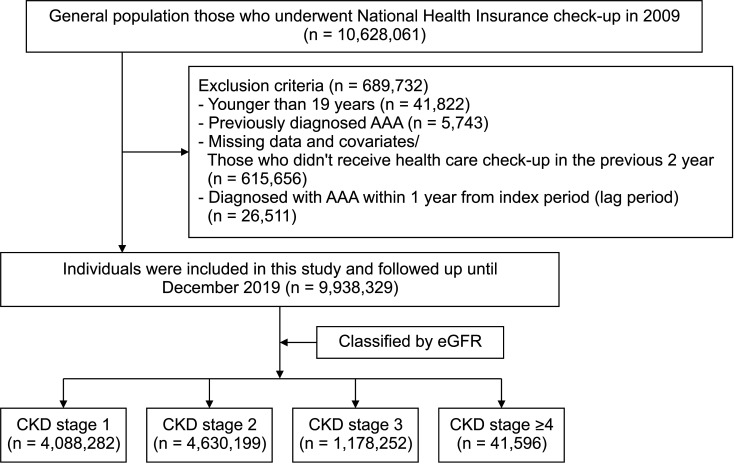
We evaluated data for Koreans older than 19 years who received at least 1 health checkup provided by the NHIS from January 2009 to December 2009. To reduce the possibility of including AAA at baseline, those who were diagnosed with AAA before the health care checkup (index date) were excluded. Moreover, in order to reduce the selection bias, those who were diagnosed with AAA within 1 year after the index date (lag period) were also excluded, as diseases that were thus far undiagnosed may be uncovered upon medical checkup. In addition, individuals with missing data for any variables and those who did not receive a general health checkup in the previous 2 years were also excluded (Fig. 1). The remaining individuals were then tracked from the index date until December 31, 2019 (last follow-up date).
Study design and definitions
The primary endpoint was newly diagnosed AAA until the last follow-up date. AAA was defined as at least 2 claims per year under ICD-10 codes, at least 1 claim for hospitalization under the same ICD-10 codes, or at least 1 claim for surgery under the same ICD-10 codes [10]. Current smokers were defined as those who smoked 100 or more cigarettes in their life and continued smoking within 1 month before the 2009 nationwide health checkup. Heavy drinking was defined as those consuming 210 g or more of alcohol per week. Regular exercise was defined as a high-intensity exercise for at least 20 minutes or moderate-intensity exercise for at least 30 minutes at least once a week based on a self-report questionnaire. Hypertension was identified based on blood pressure measurement (systolic blood pressure of ≥140 mmHg or diastolic blood pressure of ≥90 mmHg) or by at least 1 claim with ICD-10 codes for hypertension. Diabetes mellitus (DM) was diagnosed based on fasting blood glucose (≥126 mg/dL; to convert to mmol/L, multiply by 0.0555) or at least 1 claim with ICD-10 codes for DM diagnosed by a physician. Dyslipidemia was defined as fasting serum total cholesterol of ≥240 mg/dL or as ICD-10 code and a prescription for lipid-lowering drugs. CKD stage was classified into 4 group based on the eGFR (calculated by the Modification of Diet in Renal Disease Study [MDRD] equation); CKD grade 1 (eGFR of ≥90 mL/min/1.73 m2), 2 (eGFR of ≥60 and <90 mL/min/1.73 m2), 3 (eGFR of ≥30 and <60 mL/min/1.73 m2) and ≥4 (eGFR of <30 mL/min/1.73 m2 including end-stage renal disease [ESRD]). ESRD was defined as at least 1 claim with a special code (V code) that was assigned in the initiation of renal replacement therapy (hemodialysis, V001; peritoneal dialysis, V003) and kidney transplantation (V005). Proteinuria was defined as more than 1+ result in dipstick urine test. Baseline covariates and comorbidities were evaluated during the screening period and defined using ICD-10 codes (Supplementary Table 1), and the robustness of these definitions has been validated in our previous study [1011].
Statistical analysis
Data are presented as the mean with standard deviation (SD) for continuous variables and as a number with percentage for categorical variables. The t-test was used to compare continuous variables. Categorical variables were compared with the Fisher exact test or chi-square test, as appropriate. The incidence rates of AAA are presented per 1,000 person-years. Cumulative incidences of AAA according to the degree of proteinuria were compared using the Kaplan-Meier method and the log-rank test. Multivariable Cox proportional hazards models were employed to evaluate the association between the grade of CKD and the risk of AAA, and the results are presented as hazard ratios (HRs) with 95% confidence intervals (CIs). A 2-sided P-value of <0.05 was considered statistically significant. All statistical analyses were performed with SAS software ver. 9.2 (SAS Institute, Cary, NC, USA).
RESULTS
Baseline characteristics of the study population
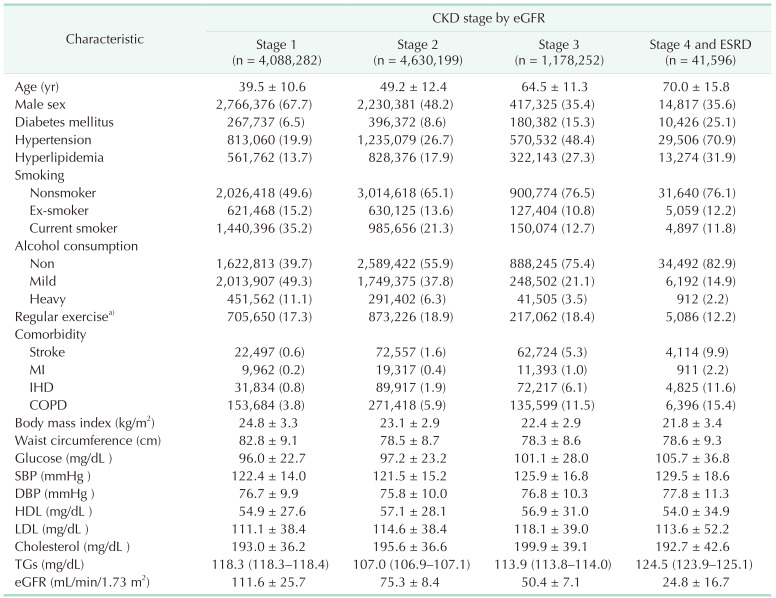
A total of 9,938,329 individuals were enrolled in this study. The subjects were classified into 4 group based on CKD stage (number [%], mean eGFR ± SD); stage 1 (n = 4,088,282 [41.1%], 111.57 ± 25.67 mL/min/1.73 m2), stage 2 (n = 4,630,199 [46.6%], 75.33 ± 8.35 mL/min/1.73 m2), stage 3 (n = 1,178,252 [11.9%], 50.36 ± 7.1 mL/min/1.73 m2), and stage ≥4 (n = 41,596 [0.4%], 24.76 ± 16.66 mL/min/1.73 m2). Baseline clinical characteristics are summarized in Table 1. The advanced stage of CKD was positively correlated with age, glucose, and various comorbidities such as DM, hypertension, hyperlipidemia, stroke, MI, CVD, and chronic obstructive pulmonary disease (COPD) (all Ps < 0.001). On the other hand, BMI, waist circumference, and the rates of current smoking and heavy drinking were significantly lower in the advanced CKD stage (all Ps < 0.001).
Incidence of abdominal aortic aneurysm according to the chronic kidney disease stage
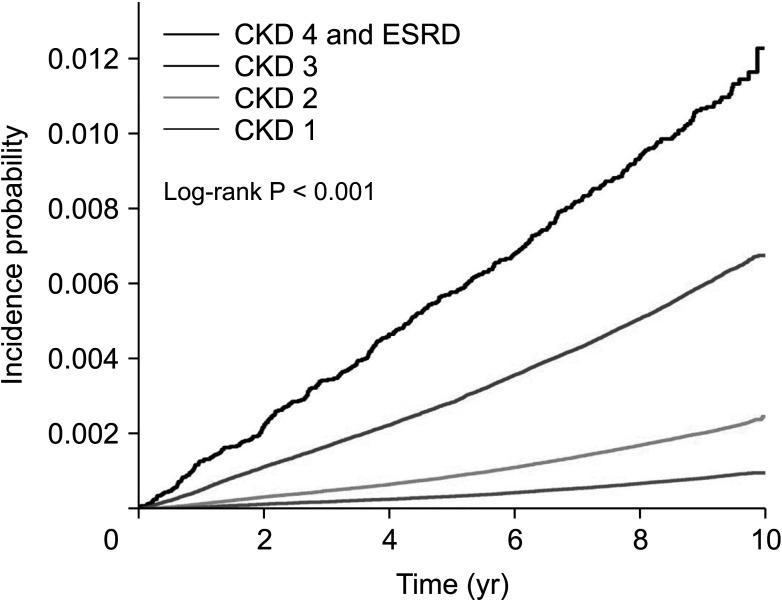
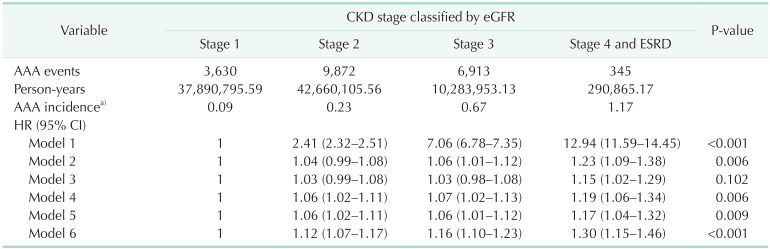
During a median follow-up of 9.3 years (interquartile range, 9.1–9.6 years), 20,760 individuals (0.2% of the total population) were observed to develop AAA. The incidence rates of AAA were 0.10, 0.23, 0.67, and 1.19 per 1,000 person-years in stages 1, 2, 3, and ≥4, respectively (Fig. 2). The Kaplan-Meier curve demonstrated that the AAA incidence increased proportionally to the stage of CKD (Fig. 2). More advanced stage of CKD was associated with an increased risk of AAA development, with unadjusted HR of 2.414 (95% CI, 2.32–2.51), 7.06 (95% CI, 6.78–7.35), and 12.94 (95% CI, 11.59–14.45) for the CKD stage 2, 3, and ≥4, respectively, compared with CKD stage 1 (P < 0.001). After adjusting covariates, including age, sex, smoking, alcohol consumption, regular exercise, HR was decreased to 1.03 (95% CI, 1.00–1.08), 1.03 (95% CI, 0.98–1.08), and 1.15 (95% CI, 1.02–1.29) for the CKD stage 2, 3, and ≥4, respectively, which was not significant (P = 0.102) (Table 2, model 3). However, the HR was slightly increased and showed a significant difference after supplementing stroke, DM, hypertension, hyperlipidemia, MI, COPD, BMI, and urine protein, risk of AAA was increased by nearly 30% in CKD stages 4 and 5 compared with CKD stage 1 HR of 1.30 (95% CI, 1.15–1.46) (P < 0.001) (Table 2, model 6).
Subgroup analysis of the abdominal aortic aneurysm development according to the chronic kidney disease stage
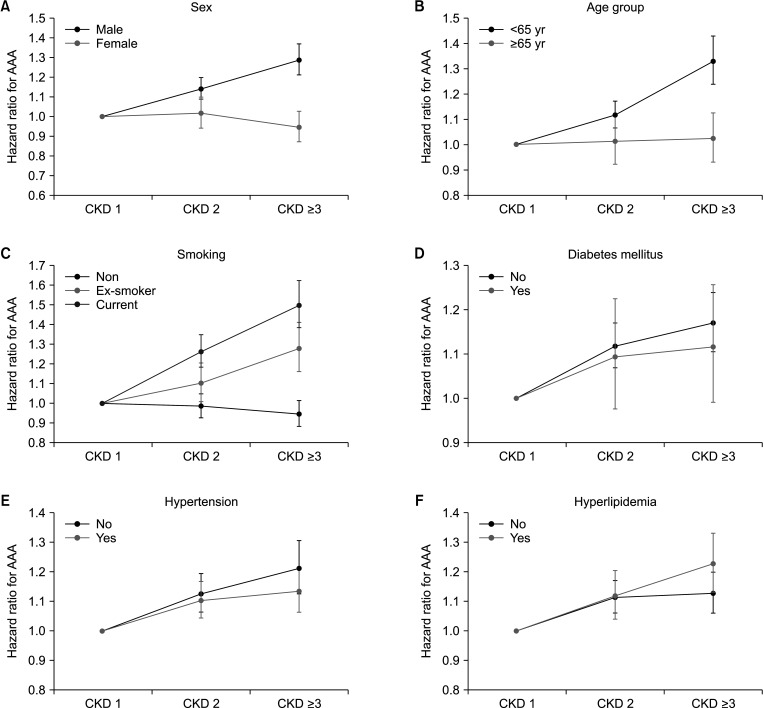
In the subgroup analysis, CKD was classified into 3 groups: stages 1, 2, and ≥3. Univariate analysis was performed to identify the effects of CKD on the development of AAA according to several factors, such as age group, sex, smoking, hypertension, hyperlipidemia, and DM and overt proteinuria with adjusting the various covariates including age, sex, smoking, alcohol consumption, regular exercise stroke, DM, hypertension, hyperlipidemia, MI, COPD, BMI, and urine protein (model 6). Compared with CKD stage 1, CKD stage ≥3 group was associated with the increased risk of AAA in individuals with male, age younger than 65 years old, ex-smoker, and current smoker, but not in those without female, age 65 years or more, and nonsmoker with adjusted HR (95% CI); 1.29 (1.21–1.37) vs. 0.95 (0.87–1.03), 1.33 (1.24–1.43) vs. 1.02 (0.93–1.13), 1.28 (1.16–1.41) vs. 0.95 (0.88–1.01), and 1.50 (1.38–1.62) vs. 0.95 (0.88–1.01), respectively (interaction P < 0.05). However, the risk of AAA development was increased those individuals with/without hyperlipidemia (adjusted HR [95% CI]: 1.23 [1.13–1.33]/1.13 [1.06–1.20], respectively) and proteinuria (adjusted HR [95% CI]: 1.30 [1.07–1.57]/1.15 [1.09–1.22], respectively) in CKD grade ≥3 group compared with CKD grade 1 (all interactive Ps < 0.05) (Supplementary Table 2). On the other hand, there was graded increase in the risk of AAA according to the CKD stage, regardless of age group (reference age of 65 years old), smoking, hypertension, hyperlipidemia, and DM and overt proteinuria. The difference between adjusted HR on each subgroup was observed more prominent as CKD advanced (Fig. 3).
DISCUSSION
To the best of our knowledge, this is one of the largest population studies which demonstrate the association between CKD and the development of AAA. The following results were obtained from the present study: (1) the CKD act as a risk factor for AAA; (2) the AAA development is increased proportionally as CKD stage as advanced; (3) regardless of age group, smoking, hypertension, hyperlipidemia, and DM and overt proteinuria, there was graded increase in AAA according to the CKD stage; and (4) this risk showed prominent as CKD stage has advanced.
CVD is one of the major causes of death in patient with CKD, and CKD is a well-known risk factor for CVD, such as coronary heart disease, heart failure, and cerebral vascular disease [1112]. The prevalence of AAA depends on associated risk factors that include advanced age, male sex, Caucasian, positive family history, smoking, hypertension, hypercholesterolemia, peripheral vascular occlusive disease, and coronary artery disease, and almost of these risk factors are the classical risk factors for atherosclerosis, which demonstrate that AAA is one of the subtypes of CVDs [6121314]. On this basis, we hypothesized that CKD is a risk factor for AAA; to evaluate the relationship between the severity of CKD and the incidence of AAA, we conducted a study using the NHIS database.
There are numerous studies about the significant relationship between poor outcomes after AAA repair and impaired renal function is more certain and has been observed in many studies for both open and endovascular aneurysm repair (EVAR) [151617]. Furthermore, renal impairment has consistently been shown to be an important prognostic indicator in the numerous risk scores that have been developed and validated in patients undergoing aneurysm repair [181920]. Reversely, there are a few studies on the association between CKD and the incidence of AAA; however, the reported data are scarce, and the results reported are conflicting [782122]. A screening program at a regional Veterans affairs health system study identified renal insufficiency as a risk factor for AAA. They found that eGFR of <60 mL/min/1.73 m2 was significantly associated with AAA (36.7% vs. 24.3%, P < 0.001) [21]. A Japanese cohort study with 261 patients suggested that CKD is an additional risk factor for aortic disease (aneurysmal rupture, aortic dissection)-related death in the general population [23]. And recently, a study using data from the ARIC (Atherosclerosis Risk in Communities) Study, which enrolled approximately 15,000 patients, demonstrated that CKD itself and its measurements, such as eGFR and microalbuminuria, are associated with the risk of AAA and greater abdominal aortic diameter [22]. The present study, which enrolled nearly 10 million people, also supports these results, and by adjusting for well-known risk factors of AAA (e.g., age, sex, smoking, hypertension, hyperlipidemia, etc.), we found that CKD is an independent risk factor for AAA development.
There was no definite explanation of how CKD affects the development of AAA; however, there is a plausible hypothesis association between CKD and AAA. First, both CKD and AAA share well-known risk factors and exhibit an increased risk of CVD, which demonstrated that risk factors of CKD could affect the development of AAA. Second, several matrix metalloproteinases (MMP) (such as MMP- 2, 8, 9), a disintegrin and metalloproteinase (ADAM) family, and tissue inhibitors of metalloproteinases (TIMPs) are concomitantly involved in the development of both aortic aneurysm and CKD [24]. MMP- 2, 8, 9, TIMP overexpressed and hyperactivated in the aneurysm [2425], at the same time these MMPs could damage the tubular cells and activate a series of proinflammatory and profibrotic signals in the kidney, and result in accelerating CKD progression [26]. Third, arteries of CKD patients have features of atherosclerosis, calcifications, and increase stiffness compared to healthy populations, and contents of atherosclerotic plaque of CKD patients showed poor collagen fiber and an increase in calcium deposition which these wall conditions could possibly be the risk of developing aneurysmal degeneration [2728]. Fourth, in the aspect of the biomechanical study, the AAA wall of CKD patient has reduced “failure tension” (defended as the resistance of a wall portion against rupture, independent of the actual wall thickness) [2930]. And this reduction of failure tension was also demonstrated in increased blood value of potassium and urea, which indicate that CKD increases the risk of AAA rupture [29]. From this point of view, CKD might increase the risk of AAA.
This study has several limitations. First, the study was a retrospective design based on data from a nationwide population database, which is susceptible to several biases, including selection bias. In the case of the national health checkup, which is not compulsory, not all health insurance subscribers receive medical examinations regularly. Therefore, the subjects most likely included those who were healthier, and patient cohorts are often excluded from the NHIS database. Second, our study was based on insurance claims with ICD-10 codes for AAA which might not accurately represent the participants’ specific disease status, and drug prescriptions do not guarantee compliance; therefore, errors in the classification of comorbidities are to be expected. Third, because information on the severity of AAA (eg., maximal diameter of aneurysm) was unavailable in the NHIS, we could not estimate how the degree of CKD affects the diameter of AAA like in other studies. Fourth, CKD grade, which was classified by eGFR calculated by the MDRD equation, has limited value as we could not consider all of their clinical course or medication history. Fifth, as the grade of CKD has advanced, there is more tendency of performing radiologic examination and medical checkup compared with healthier subjects. As a result, this might increase the diagnostic rate of AAA in advanced CKD patients, which might increase the selection bias. Finally, this study cohort was entirely composed of a Korean population, the results could not represent all ethnic groups. However, this is the largest population study, which demonstrated the impact of CKD on AAA, and by adjusting well-known risk factors of AAA such as age and sex, we made an effort to increase the robustness of study.
In conclusion, this study demonstrates that CKD was positively associated with an increased risk of developing AAA, and its risk showed a graded increase as CKD stage advanced. And by adjusting well-known risk factors of AAA such as age, sex, smoking, hypertension hyperlipidemia, CKD was an independent risk factor of AAA development. With this in mind, we suggested screening of AAA in patients with advanced CKD or ESRD, with ultrasonography or nonenhanced abdominal CT, to prevent the adverse event. However, in order to support this rationale, prospective studies and basic research are warranted.
 XML Download
XML Download