

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Primary liver cancer accounts for 8.3% of cancer deaths. It is the 4th leading cause of cancer-related death in the world [1]. Hepatocellular carcinoma (HCC) accounts for a major proportion of primary liver cancer. Its incidence is on the rise in the Americas and most European countries. It is still the highest in East Asia. Common causes of HCC are HBV, HCV, alcohol, and nonalcoholic steatohepatitis [2]. Although many efforts have been made to manage HCC, its prognosis is still poor. The survival rate of HCC decreases dramatically year by year. One of the contributing factors to such a poor prognosis is the presence of tumor thrombus in portal vein or hepatic vein at the time of diagnosis [34]. Cancer cells can disseminate through bloodstream where vascular invasion is present, leading to a high recurrence rate [5]. Tumor thrombus can also deteriorate remnant liver function by reducing blood supply [6].
In Barcelona Clinic Liver Cancer (BCLC) staging, HCC accompanied by portal vein tumor thrombus (PVTT) is classified as advanced stage. Other associations such as the European Association for the Study of the Liver and the American Association of the Study of Liver Diseases follow the BCLC staging classification. Without treatment, expected median survival time of patients with HCC accompanied by PVTT is only 2.7–4.0 months [5]. PVTT is a relatively stronger factor affecting mortality than extrahepatic spread or performance status [6].
Considering expected survival time, the BCLC staging system does not recommend curative treatments to patients with HCC accompanied by PVTT. Instead, systemic therapy such as sorafenib is recommended currently. However, the outcome of sorafenib therapy remains unsatisfactory, with overall survival (OS) time of only 6–8 months [2]. Under these circumstances, various therapeutic approaches have been made for improving OS, such as treatment with surgical resection (SR), radioembolization, transcatheter arterial chemoembolization (TACE), and combination of these treatments [5]. Recently, studies have reported that these treatments can give better survival outcomes than sorafenib [57]. Nonetheless, it is still unclear which of these treatments yields better outcomes. In addition, most previous studies compared survival outcomes with a retrospective observational method.
Designing a prospective randomized controlled study that directly compares the priority of each treatment modality in patients with HCC accompanied by PVTT has practical limitation. While traditional meta-analysis can perform direct treatment comparison, it is not suitable for comparison between multiple treatment groups. Network meta-analysis can help decision-making by comparing multiple competing treatments in a single analysis even when there is no direct comparison between 2 specific treatments. Thus, the aim of this study was to determine the relative effectiveness and priorities of different treatment regimens for patients with HCC accompanied by PVTT using network meta-analysis.
METHODS
This meta-analysis study followed the guidelines of PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses). It was registered with the PROSPERO database (no. CRD42022336841). The Institutional Review Board of Catholic Kwandong University International St. Mary’s Hospital confirmed that ethical approval was not required because this study used previously published papers.
Search strategy
A systematic search of MEDLINE/PubMed, Embase, and the Cochrane Library was undertaken to identify candidate articles published between January 2001 and December 2021 reporting OS after different types of treatments in patients with locally advanced HCC accompanied by PVTT and comparing OS according to different modalities. To identify as many appropriate articles as possible, we selected “carcinoma, hepatocellular” or “liver cell carcinomas” or “vascular invasion” or “portal vein invasion” or “portal vein tumor thrombus” as Medical Subject Headings terms. Other keywords such as “sorafenib,” “Nexavar,” “transarterial chemoembolization,” “TACE,” “radiotherapy,” “radiation,” “EBRT,” “radioembolization,” and “TARE” were also used. Detailed search terms used for this analysis are presented in Supplementary Table 1. Titles and corresponding abstracts of articles in search results were examined to select relevant ones. When an article was considered to be potentially relevant to our analysis, 2 researchers (SL and BB) independently reviewed a full copy of the publication based on the inclusion and exclusion criteria stated below. Hazard ratios (HRs) and restricted mean survival time (RMST) were obtained either directly or via the method described below from original articles. They were then combined for the network meta-analysis.
Inclusion and exclusion criteria
We selected articles that presented OS after treating patients with HCC accompanied by PVTT following different treatment regimens and provided HR between different treatment groups. If Kaplan-Meier (KM) survival curve was only provided without HR reported, we obtained cumulative HRs using the method described below. Eligible studies were limited to prospective randomized controlled studies, propensity score-matched retrospective cohort studies, and retrospective observational studies using propensity score analysis to reduce bias. If 2 or more studies shared identical cohort data, the one using more accumulated data was selected. Articles published in non-English language were excluded.
Data extraction
Two researchers (BB and YP) extracted data of the first author, year of publication, country of origin, study design, the number of patients, demographics of patients, each treatment regimen, and estimated HR and RMST between 2 different treatment groups. The extent of PVTT was reclassified according to the General Rules for the Study of Primary Liver Cancer by the Korean Liver Cancer Study Group as Vp0–Vp4 [8].
Reconstructing Kaplan-Meier data and obtaining cumulative hazard ratios
If obtainable from the original article, HR and 95% confidential interval (CI) between 2 different treatment groups were recorded. If not available, KM survival data were secondarily restored from printed survival curves to calculate HR. The number of patients at risk at time interval points and the total number of events were obtained from the text. Coordinates of time and survival probability were obtained from original survival curves printed on the paper employing the DigitizeIt software (www.digitizeit.de). Restored KM survival data of 2 different treatment groups were combined to calculate HR of corresponding study by applying a unique algorithm proposed in a previous study [9]. RMST differences between treatment groups were also obtained using restored KM survival data. Secondarily computed HRs and RMST differences were used for network meta-analysis with original ones.
Assessing risk of bias in included studies
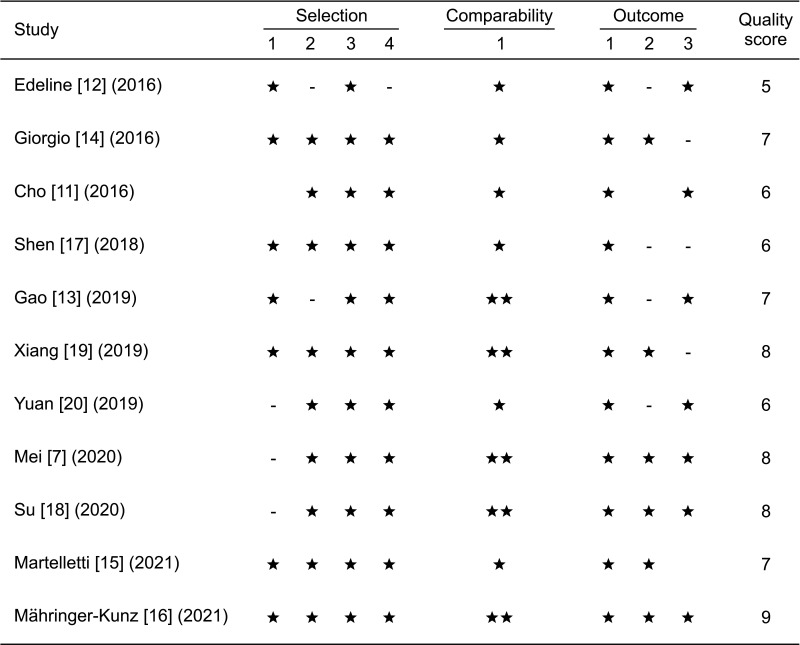
The quality of each study included in this analysis was formally assessed using the modified Newcastle-Ottawa Scale (NOS) that included selection, comparability, and outcome.
Statistical analyses
All statistical analyses were performed using R software ver. 3.6.3 (R Foundation for Statistical Computing, Vienna, Austria). “Survival” package in R was used for HR calculation. The RMST difference was estimated using the “survRM2” package. Network meta-analyses were conducted employing the “netmeta” package. Endpoints in this network meta-analysis were HRs, mean difference (MD) of survival length compared to systemic therapy with sorafenib alone, and corresponding 95% CIs using random-effects model. Each treatment regimen was then ranked using the P-score provided by the “netmeta” package to assess the probability of the superiority of each treatment regimen. Statistical significance was set at P < 0.05. The I2 statistics provided a measure for the percentage of total variation attributable to heterogeneity between studies. Heterogeneity was considered significant when the I2 value exceeded 50% [10].
RESULTS
Search results
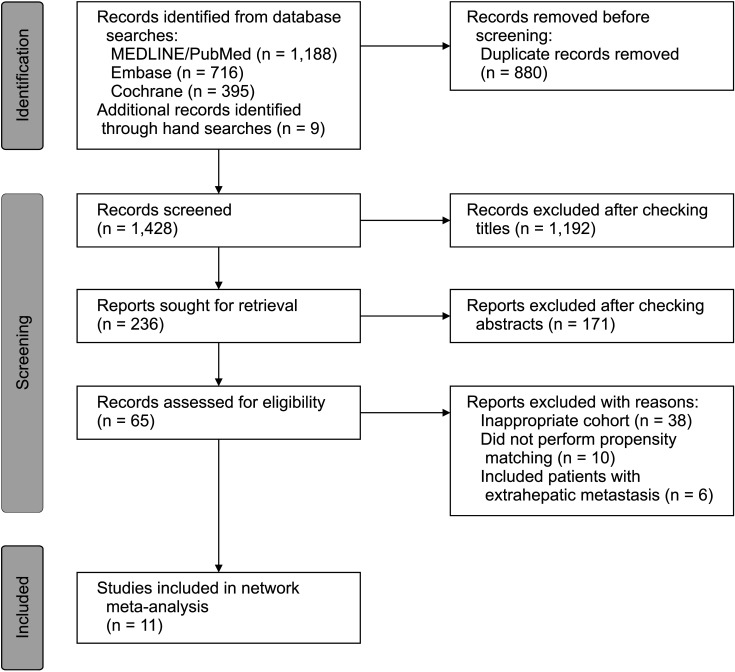
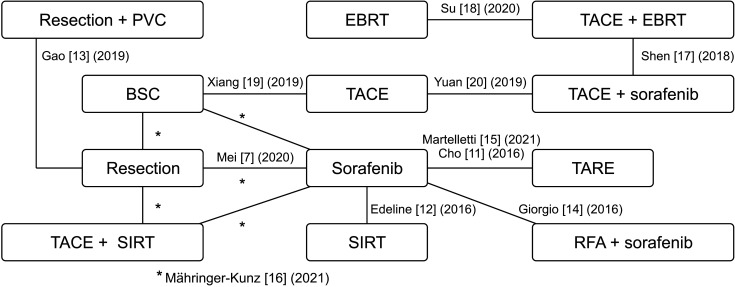
Detailed results from the search strategy are presented in Supplementary Table 1. Of 1,428 non-duplicate studies identified in the literature search, 1,192 were excluded due to their irrelevant titles. The remaining 236 studies were screened again based on their abstracts and 65 studies were selected for full-text review. Finally, 11 studies were found to be qualified for analysis [711121314151617181920]. A flow diagram of the literature searches and selection process is shown in Fig. 1. The 11 studies included 1 prospective randomized trial, 9 propensity-matched retrospective cohort studies, and 1 retrospective cohort study implementing propensity score adjustment in a regression model. Seven studies were conducted in East Asian countries (China and Korea) and 4 were conducted in European countries (France, Germany, and Italy). Those 11 studies included for analysis had NOS scores ranging from 5 to 9, indicating a high quality (7 studies with NOS scores of 7–9 and 4 studies with NOS scores of 5–6) (Fig. 2). Because of a multi-arm design in 1 study, 16 pairwise comparisons were available for 12 different treatment regimens: (1) systemic therapy with sorafenib alone, which was used as the reference treatment regimen; (2) best supportive care; (3) SR; (4) SR followed by portal vein chemotherapy (PVC); (5) radiofrequency ablation (RFA) with sorafenib therapy; (6) external beam radiation therapy (EBRT); (7) selective internal radiation therapy (SIRT); (8) TACE; (9) TACE with EBRT; (10) TACE combined with SIRT; (11) TACE with sorafenib therapy; and (12) transarterial radioembolization (TARE). The network diagram for OS is presented in Fig. 3.
Characteristics and demographics of selected studies
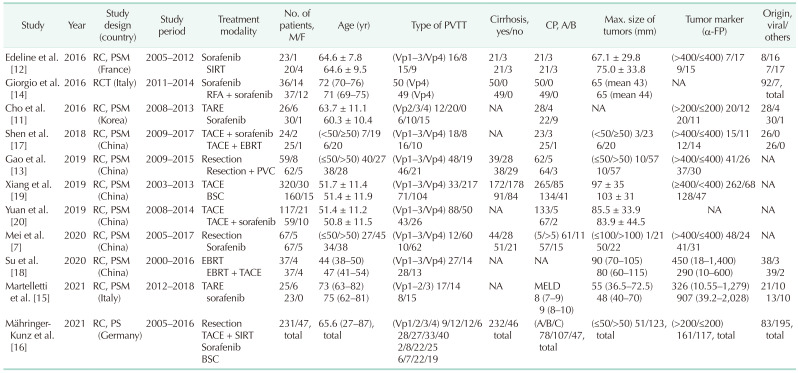
Characteristics of patients enrolled in the 11 selected studies are provided in Table 1. A total of 1,623 patients were included for data analysis. Most treatment groups were composed predominantly of patients with Child-Pugh class A cirrhosis. All studies included more male patients than female patients. Viral hepatitis was the predominant etiology of HCC in most studies. Serum α-FP levels were markedly elevated in most patients with HCC accompanied by PVTT. On average, 47.7 % (range, 23.8%–100%) of PVTT status was Vp4.
Network meta-analysis results
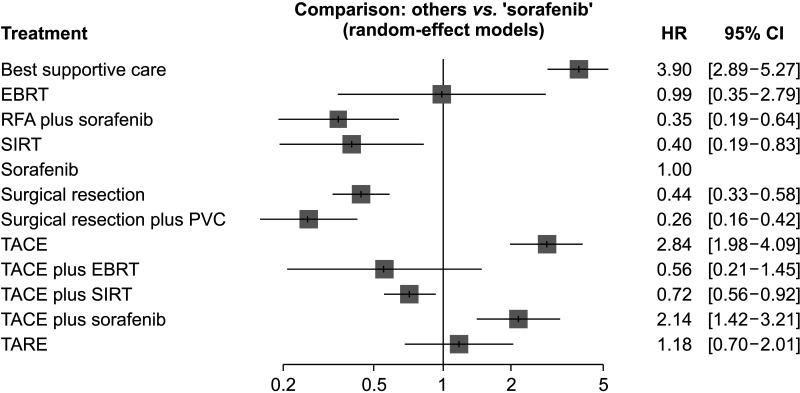
Results of random-effects network meta-analysis are summarized in Fig. 4. Indirect estimates of HRs comparing sorafenib therapy alone vs . other treatment regimens are presented in Fig. 4A. For OS, 4 treatment regimens had relatively higher efficiency than sorafenib therapy alone. Patients treated with SR (HR, 0.44; 95% CI, 0.33–0.58), SR followed by PVC (HR, 0.26; 95% CI, 0.16–0.42), RFA with sorafenib therapy (HR, 0.35; 95% CI, 0.19–0.64), and TACE combined with SIRT (HR, 0.72; 95% CI, 0.56–0.92) had significantly lower HR for OS than those with sorafenib therapy alone. SR followed by PVC was ranked the best treatment regimen for OS (P-score, 93.9%), followed by RFA with sorafenib therapy (P-score, 86.0%), SR (P-score, 77.1%), and TACE combined with SIRT (P-score, 55.9%). There was neither significant heterogeneity (I2 = 0%) nor inconsistency (Q = 0.91, P = 0.821) within treatment regimens compared.
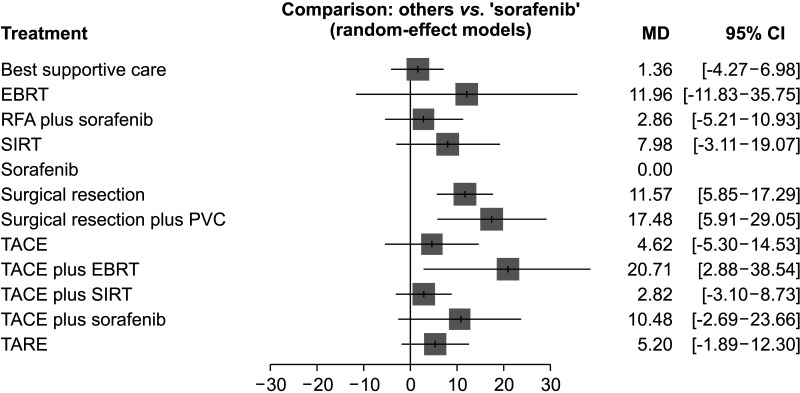
Further analyses were performed to estimate mean survival time difference according to each treatment regimen. It was conducted using RMST based on time-to-event data reconstructed from the KM curves in each original article. Patients treated with SR (MD, 11.57 months; 95% CI, 5.85–17.29 months), SR followed by PVC (MD, 17.48 months; 95% CI, 5.91–29.05 months), and TACE combined with EBRT (MD, 20.71 months; 95% CI, 2.88–38.54 months) had significantly longer survival than those treated with sorafenib therapy alone (Fig. 5). Significant heterogeneity (I2 = 86.5%) and inconsistency (Q = 35.26, P < 0.001) existed among original studies.
DISCUSSION
Although the standard practical guidelines such as the BCLC and American Association for the Study of Liver Diseases recommend systemic target therapy to treat HCC accompanied by PVTT [2122], recent studies have stated that patients treated with aggressive locoregional therapeutic modalities such as TARE, TACE/SIRT, and SR have better prognosis than those treated with sorafenib therapy alone [1623]. These guidelines have a limitation in that they do not distinguish between HCC with gross vascular invasion and those with extrahepatic metastasis, considering them as the same class. However, it would be reasonable to conduct a study for HCC accompanied by PVTT excluding extrahepatic metastasis because they have a chance of being cured with aggressive locoregional treatment regimens. Our work indirectly but comprehensively compared survival outcomes of various treatment regimens using network meta-analysis, in which locoregional therapeutic modalities demonstrated better outcomes than systematic therapy with sorafenib alone. This statistical analysis method could suggest which treatment regimen is most effective for patients with HCC accompanied by PVTT without extrahepatic metastasis. According to our study, SR followed by PVC was ranked the best treatment regimen for those patients. To the best of our knowledge, the work demonstrated here is the first network meta-analysis of comparative efficiency of various treatment regimens for HCC accompanied by PVTT without extrahepatic metastasis.
SR has not been considered an absolute contraindication for patients with HCC accompanied by PVTT [18], but a possible treatment option for selected ones. It has brought great improvement in survival outcomes for patients with HCC accompanied by PVTT due to advanced surgical techniques and establishment of methods for patient selection [24]. One study has demonstrated that the median OS is 20.7 months in the SR group and 11.6 months in the sorafenib group [7]. However, more than 80% of patients appeared to have unresectable HCC at the time of diagnosis. Only a limited group of patients can be candidates for SR. In addition, SR is associated with risk of hospital mortality and postoperative complications. Patients should be carefully selected for SR according to their performance status and remnant liver function reserve. If PVTT is confined to segmental or sectional branches of the portal vein, anatomical resection can secure tumor-free margins. When the PVTT extends to the major branch or the main portal vein, en-bloc resection of portal vein or a concomitant thrombectomy could be performed [25].
Despite surgical management, owing to its poor prognosis and high recurrence rate, the need for adjuvant therapy for PVTT has been advocated. Various adjuvant treatments have been investigated and some of them have been reported to be able to prolong OS. Peng et al. [26] have assessed postoperative TACE with a randomized comparative trial. Sun et al. [27] have carried out a randomized controlled trial for postoperative adjuvant intensity modulated radiation therapy. Both studies showed better survival outcome of the treatment group than that of the control group [2627]. However, studies comparing superiority of adjuvant treatment have not been reported yet. A multicenter randomized control is needed. In our study, PVC was performed as adjuvant therapy. It was ranked as the best treatment for HCC accompanied by PVTT. However, PVC is technically not feasible under some circumstances. Thus, its practical application is limited. More investigation is needed to validate the most proper postoperative management.
TACE has been widely used for unresectable HCC. Its technical development has helped more patients achieve better survival outcome. TACE is one of the locoregional treatments that carry anticancer agents directly to cancer through tumor feeding artery. Previously, TACE was perceived as a contraindication to patients with HCC accompanied by PVTT, especially when thrombosis was present in the main portal vein [45]. It is attributed to theory that TACE has an embolization effect, which can worsen the liver function by reducing blood supply. However, some studies have stated that if collateral circulation is intact, TACE is applicable regardless of PVTT type without severe complications [28]. In addition, liver necrosis rarely occurs after TACE. There are limited treatment options for HCC accompanied by PVTT. Considering the safety of TACE, it is commonly chosen for patients with HCC accompanied by PVTT in practice. Based on recent studies, TACE is obviously superior to the best supportive care [19]. However, compared to sorafenib, its superiority is not clearly identified. Instead, combinations of various treatments can lead to a better prognosis than TACE alone. Especially, combination treatment of TACE and sorafenib and combination treatment of TACE and EBRT offered better survival outcomes than sorafenib alone in our study.
Another treatment option for HCC accompanied by PVTT is EBRT. Most concerns about radiation therapy in HCC are assertions that HCC is a radio-resistant tumor and that serious complications can occur due to radiation-induced liver disease. However, multiple studies have shown that EBRT is a safe and effective treatment option for unresectable HCC. With the improvement of radiation delivery techniques that enable us to localize tumor, radiation therapy is playing an important role in multidisciplinary treatment for HCC accompanied by PVTT. One retrospective study using propensity score matching has argued that EBRT should be the first-line therapy, especially for HCC accompanied by PVTT, rather than sorafenib since EBRT can lead to longer survival time [29]. However, serious unsolved problems such as radiation-induced lung disease and bowel toxicity limit the application of EBRT [30]. Further studies on effectiveness and safety of EBRT are needed.
This study has several limitations. First, only 1 prospective randomized trial was included. Other included studies were all retrospective ones. However, we selected retrospective studies with propensity score matching to reduce bias. Second, newly introduced chemotherapeutic agents were not included in this study. Recently, according to the BCLC guideline published in 2022, atezolizumab combined with bevicizumab or durvalumab combined with tremelimumab was newly recommended for 1st line therapy in patients with advanced stage of HCC. However, published studies comparing sorafenib and other chemotherapeutic agents included patients with advanced stage HCC including extrahepatic metastasis. These articles were excluded because our study targeted patients with HCC accompanied by PVTT without extrahepatic metastasis. Third, the results of this study cannot be uniformly applied to all patients with HCC accompanied by PVTT. Most of the patients included in this study had compensated liver cirrhosis for whom aggressive locoregional treatments were possible. Lastly, since a wide variety of treatment regimens are applied to HCC accompanied by PVTT, network meta-analysis with all regimens is virtually impossible. Therefore, further study comparing the different treatment regimens classified based on the mainstay treatment such as SR, TACE, and stereotactic body radiation therapy is necessary.
In conclusion, results of our study support that aggressive locoregional treatment with or without combination of systemic therapy can bring better survival outcomes for patients with HCC accompanied by PVTT rather than systemic treatment with sorafenib alone. Thus, we propose that aggressive locoregional treatments such as SR or TACE combined with EBRT should be considered for patients with HCC accompanied by PVTT.
 XML Download
XML Download