

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Anastomotic leakage (AL) is one of the most serious complications following colorectal surgery, with an incidence rate of 0%–20% [1]. AL can lead to higher morbidity and mortality and result in prolonged lengths of hospital stay and increased treatment costs [23]. Additional surgery due to AL might be required, leading to reduced quality of life [4]. Furthermore, AL may affect oncologic outcomes in cancer patients [567].
In rectal surgery, the rate of AL is up to 29%, which is higher than that of colon surgery [8]. Improvement of surgical techniques can achieve better sphincter preservation, and AL has become a more significant issue [9]. In rectal cancer, AL can lead to increase in local recurrence and affect overall survival (OS) through extraluminal implantation of cancer cells or delayed adjuvant treatments [810]. Many studies have been conducted on the relationship between AL and oncologic outcomes, but debate remains on this issue [671112]. Therefore, the prognostic impact of AL should be assessed after correcting for other factors that can affect oncologic outcomes. In particular, chemoradiotherapy is a major factor affecting oncologic outcomes in rectal cancer patients. Therefore, it is necessary to analyze the association between AL and oncologic outcomes according to performance of chemoradiotherapy.
In this study, we aimed to investigate the prognostic significance of AL using a propensity score-matched analysis for a large cohort of rectal cancer patients who underwent curative surgery, especially in terms of chemoradiotherapy.
METHODS
This study was approved by the Institutional Review Board of Samsung Medical Center (No. 2016-09-136). An individual consent for this analysis was not needed, because this retrospective study does not include patient identifiers.
Patients
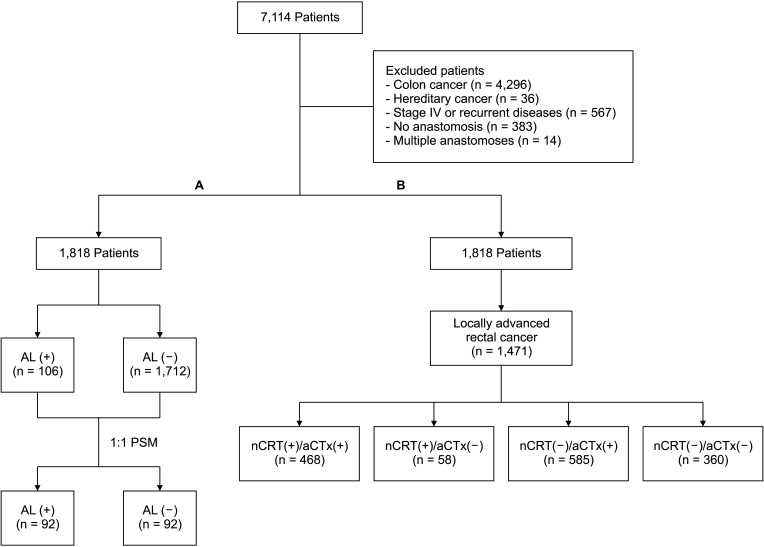
A total of 1,818 records of patients with rectal cancer who underwent curative surgery from January 2011 to December 2015 at a tertiary university-based hospital were retrospectively reviewed. All patients had histologically confirmed primary adenocarcinoma of the rectum located less than 15 cm from the anal verge and underwent low anterior resection or intersphincteric resection with or without protective loop ileostomy. Patients were excluded if they had a history of hereditary cancer, no anastomosis, multiple anastomoses due to combined resection of other lesions, recurrent diseases, or palliative surgery (Fig. 1).
Treatments
Patients with locally advanced rectal cancer were recommended to receive neoadjuvant chemoradiotherapy (nCRT) before surgery. Clinical TNM stage prior to nCRT was assessed radiologically using colonoscopy, endorectal ultrasonography, abdominopelvic computed tomography, pelvic magnetic resonance imaging, or positron emission tomography. nCRT consisted of radiotherapy at a total dose of 50.4 Gy and concomitant chemotherapy with either an intravenous 5-fluorouracil or oral capecitabine-based regimen. The patients underwent radical surgery between 6 and 10 weeks after completing nCRT. In contrast, patients with early rectal cancer or advanced rectal cancer without nCRT for any reason underwent radical surgery immediately without receiving nCRT. The 5-fluorouracil or oxaliplatin-based adjuvant chemotherapy (aCTx) was considered for either clinically or pathologically confirmed patients with locally advanced rectal cancer. Locally advanced rectal cancer included cases with clinical stage II–III (n = 1,321) or cases confirmed pathologically as stage II–III after surgery, even if they were clinical stage I (n = 150).
Anastomotic leakage
AL was defined as ‘any defect of intestinal wall integrity at the colorectal or coloanal anastomotic site (including suture and staple lines of neorectal reservoirs) leading to a communication between the intra- and extraluminal compartments,’ as proposed by the International Study Group of Rectal Cancer in 2010 [13]. AL was limited to cases occurring within 30 days after surgery. Diagnosis and management of AL followed protocols previously reported by our institution [14].
Patients were divided into AL (+) and AL (–) groups. We adjusted patient characteristics between groups and compared survival outcomes. In addition, we categorized locally advanced rectal cancer patients according to nCRT and aCTx and analyzed survival outcomes according to AL for each group. The primary endpoint of this study was disease-free survival (DFS) and OS according to AL, while the secondary endpoint was the prognostic impact of AL according to nCRT and aCTx in locally advanced rectal cancer patients.
Assessment of clinical outcomes
Postoperative surveillance for recurrence evaluation was performed every 3 months for the first 2 years after surgery and then every 6 months for up to 5 years. Most patients were evaluated with a physical examination and serum CEA level at each visit. Abdominopelvic and chest CTs were performed every 6 months. Colonoscopy and esophagogastroduodenoscopy were performed after the first year and then biennially.
Statistical analysis
Statistical analyses were carried out using IBM SPSS Statistics ver. 22.0 (IBM Corp., Armonk, NY, USA) and R software version 3.1.2 (R Foundation for Statistical Computing, Vienna, Austria; https://www.r-project.org). Categorical variables were compared using the chi-square test. A propensity score-matched analysis was performed to minimize confounding bias for oncologic outcomes between groups. Survival rates were analyzed using the Kaplan-Meier method and the log-rank test. Multivariate analyses for prognostic factors were performed using a Cox proportional hazard model. The P-values were derived from 2-tailed tests, and a P-value of ≤0.05 was considered statistically significant.
RESULTS
Patient characteristics
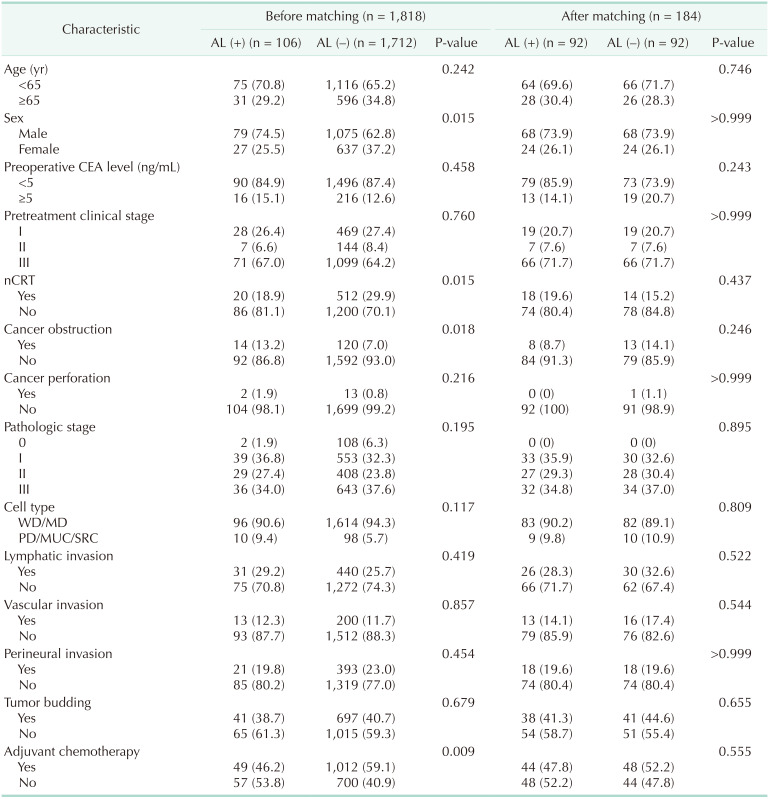
Patient characteristics according to AL are shown in Table 1. Of the 1,818 patients, 106 (5.8%) were in the AL (+) group and 1,712 (94.2%) were in the AL (–) group. There was no difference between groups in terms of age, preoperative CEA level, pretreatment clinical stage, cancer perforation, pathologic stage, cell type, lymphovascular invasion, perineural invasion, or tumor budding. AL occurred significantly more frequently in males and patients with cancer obstruction. Patients who received nCRT exhibited fewer AL than those who did not receive nCRT. This is because there was a significant difference in protective ileostomy, which was more common in patients who received nCRT (71.2% vs. 16.7%, P < 0.001). There was a difference between groups in aCTx. The AL (+) group received less frequent aCTx than the AL (–) group (46.2% vs. 59.1%, P = 0.009), and the interval from surgery to aCTx was longer in the AL (+) group (median: 39 days vs. 29 days, P < 0.001).
Prognostic impact of anastomotic leakage
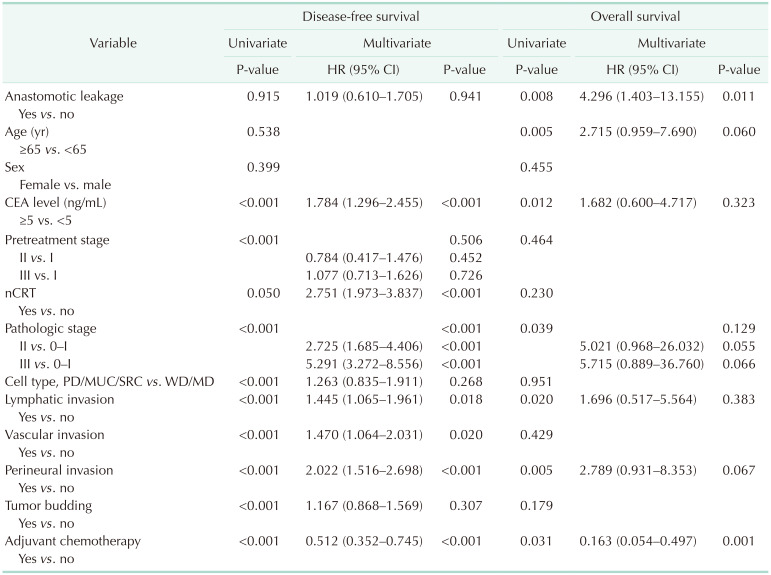
To identify the prognostic impact of AL, we analyzed DFS and OS according to AL. The median follow-up period was 49.2 months (range, 1.2–79.1 months). Before matching, there was no significant difference in DFS between the AL (+) group and AL (–) group (59.6 ± 2.0 months vs. 61.9 ± 0.6 months, P = 0.915). However, OS was significantly worse in the AL (+) group compared to the AL (–) group (67.2 ± 1.2 months vs. 70.6 ± 0.1 months, P = 0.004) (Fig. 2A). In multivariate analysis using the Cox proportional hazard model, AL was an independent prognostic factor for OS (P = 0.011) but not DFS (P = 0.941) (Table 2).
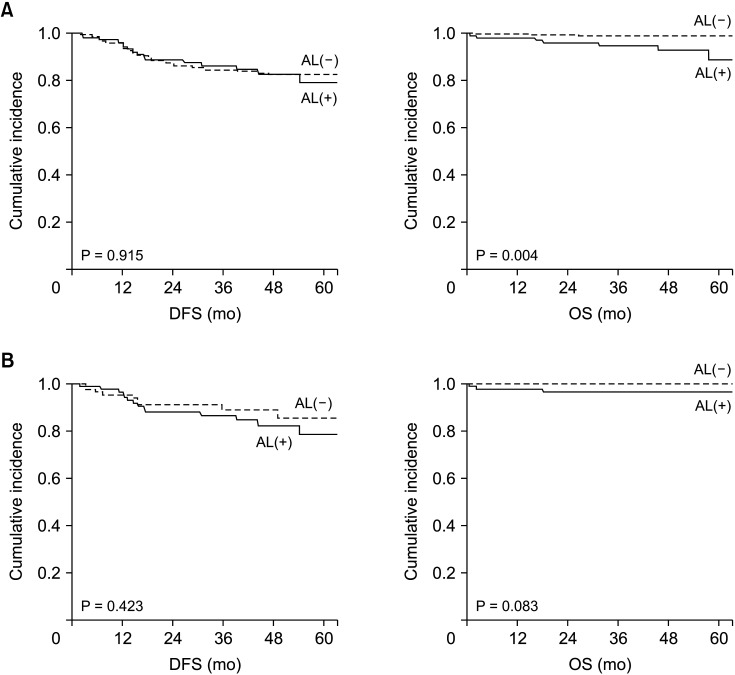
Fig. 2
Survival according to anastomotic leakage (AL) before and after matching. (A) Before matching, overall survival (OS) was significantly worse in the AL (+) group compared to the AL (–) group. (B) After matching, there were no differences in disease-free survival (DFS) and OS between the AL (+) and AL (–) groups.
![]()
Since patient characteristics according to AL were not equally distributed, a propensity score-matched analysis was performed for covariates affecting the survival outcomes. We adjusted the patients at a 1-to-1 ratio, with 92 patients in each group, and determined that all variables were equally distributed (Table 1). After matching, there were no differences in DFS and OS between the AL (+) and AL (–) groups (P = 0.423 and P = 0.083, respectively) (Fig. 2B).
Subgroup analysis according to neoadjuvant chemoradiotherapy and adjuvant chemotherapy
nCRT and aCTx are major factors affecting the survival outcomes in rectal cancer. Therefore, locally advanced rectal cancer patients were classified into 4 groups according to nCRT and aCTx: nCRT (+) and aCTx (+) group (n = 468); nCRT (+) and aCTx (–) group (n = 58); nCRT (–) and aCTx (+) group (n = 585); and nCRT (–) and aCTx (–) group (n = 360). We analyzed survival outcomes according to AL for each group. In the nCRT (–) and aCTx (+) group, patients with AL exhibited significantly worse DFS than patients without AL (44.7 ± 3.7 months vs. 57.7 ± 1.0 months, P = 0.040) (Fig. 3C). In the other 3 groups, however, we did not observe a significant difference in DFS according to AL (Fig. 3A, B, D). In the nCRT (–) and aCTx (+) group, distant recurrence occurred more frequently than local recurrence. However, local recurrence showed a more dominant tendency in patients with AL than patients without AL (18.8% vs. 9.8%). Patient characteristics of nCRT (–) and aCTx (+) group were showed in Supplementary Table 1. Also, for local recurrence, patients with AL exhibited significantly worse local recurrence-free survival than patients without AL in the nCRT (–) and aCTx (+) group (P = 0.043) (Supplementary Fig. 1). In conclusion, in locally advanced rectal cancer patients who received nCRT, there was no difference in survival outcome according to AL regardless of aCTx. In contrast, in locally advanced rectal cancer patients who did not receive nCRT, only those who received aCTx exhibited differences in survival outcomes according to AL. This finding might be due to the delay in start of aCTx in cases of AL as described above (median: 39 days vs. 29 days, P < 0.001).
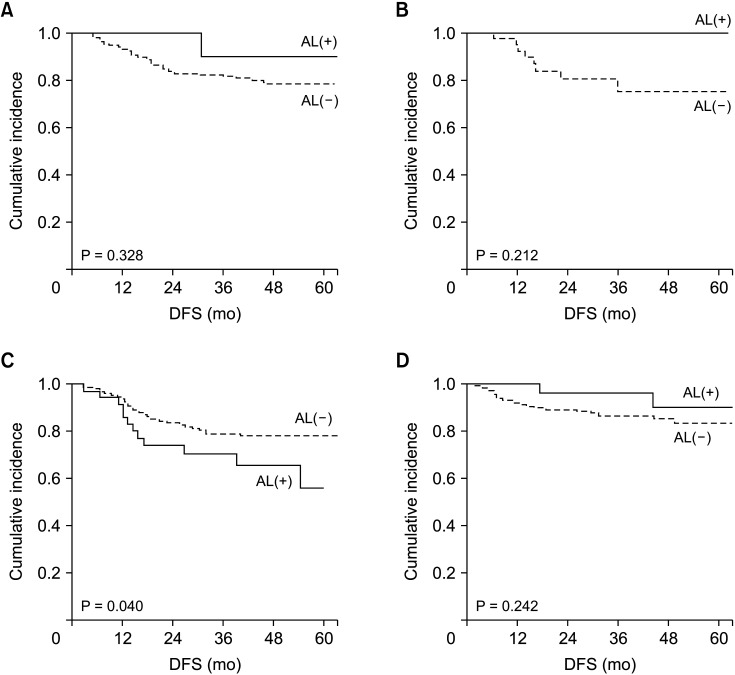
Fig. 3
Survival according to neoadjuvant chemoradiotherapy (nCRT) and adjuvant chemotherapy (aCTx) in locally advanced rectal cancer patients. (A) In the nCRT (+) and aCTx (+) group, there was no difference in disease-free survival (DFS) according to anastomotic leakage (AL). (B) In the nCRT (+) and aCTx (–) groups, there was no difference in DFS according to AL. (C) In the nCRT (–) and aCTx (+) group, patients with AL exhibited significantly worse DFS than patients without AL. (D) In the nCRT (–) and aCTx (–) groups, there was no difference in DFS according to AL.
![]()
DISCUSSION
In this study, we investigated the prognostic significance of AL for rectal cancer patients who underwent radical surgery using a propensity score-matched analysis. In matched patients, AL was not an independent poor prognostic factor for DFS or OS. In subgroup analysis for locally advanced rectal cancer patients, AL was a poor prognostic factor of DFS in patients who received aCTx without nCRT. There was no difference in DFS according to AL in patients receiving nCRT.
Many studies have investigated the prognostic impact of AL in colorectal cancer patients. Recently, a meta-analysis that included a total of 18 studies demonstrated that AL has a negative effect on oncologic outcomes in rectal cancer [12]. Another meta-analysis and other studies reported similar results [8101115]. On the other hand, there are studies that suggested no significant association between AL and oncologic outcomes [16171819]. Such debate might be due to many factors affecting the oncologic outcomes other than AL. In particular, chemoradiotherapy is a major factor affecting the oncologic outcomes in rectal cancer patients [2021]. Analyses considering these factors are necessary, but most previous studies have performed analyses without correction for these factors. A study reported that AL is not associated with oncologic outcomes in rectal cancer patients undergoing nCRT [22]. However, the study had a limitation in that patients who did not receive nCRT were not included in the analysis. In our study, we evaluated the prognostic impact of AL by correcting for the factors affecting oncologic outcomes and eliminating differences between groups. In addition, we tried to obtain a reliable result on the prognostic impact of AL by comparing between groups considering nCRT and aCTx.
In this study, we confirmed that AL was not an independent poor prognostic factor in rectal cancer. However, in patients with advanced rectal cancer, different results were shown depending on whether nCRT or aCTx was received. AL caused a decrease in survival outcomes due to delay in the start of aCTx in advanced rectal cancer patients who did not receive nCRT. However, there was no negative effect on survival outcomes due to delay in aCTx in patients who received nCRT. These findings might be due to the lower chance of local recurrence due to reduction in viable cancer cells by nCRT, even if aCTx is delayed. As many studies report, nCRT plays an important role in reducing local recurrence after surgery in rectal cancer patients by downstaging and controlling microfoci of cancer cells [232425]. Another suggestion is that radiotherapy activates the immune system so that there was no difference in survival outcomes according to AL in patients who received nCRT. Several studies have noted that radiotherapy improves tumor rejection through immunogenic modulation, which can affect tumor recurrence [262728].
There were some limitations in this study. This study was conducted retrospectively in a single institution. We did not analyze the effect of chemotherapy regimen or the degree of AL. In addition, the indications for ileostomy were not standardized. These could have caused confounding bias in this study, but we minimized this bias using a propensity score-matched analysis. In addition, we improved the reliability of the results by including a relatively large number of rectal cancer patients compared to previous studies. In particular, this study demonstrated clinical usefulness by analyzing the oncologic effects of AL according to nCRT and aCTx in rectal cancer.
In conclusion, AL contributed to adverse oncologic outcomes in patients receiving aCTx without nCRT even though it was not an independent poor prognostic factor in rectal cancer patients. Therefore, it is necessary to actively perform nCRT in patients with advanced rectal cancer.
 XML Download
XML Download