

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The identification of the recurrent laryngeal nerve (RLN) and the dissection of the nerve through its entry point is still the gold standard in preventing nerve injury and decreasing the rate of RLN palsy [1234]. Intraoperative nerve monitoring (IONM) is also very helpful to search, identify and dissect the nerve through its course during thyroid surgery [5]. Continuous IONM (CIONM) has the additional benefit of providing real-time information about the function of the RLN during thyroid surgery [67]. For the identification and dissection of the RLN, most endocrine surgeons use the lateral approach under the guidance of the IONM. However, after the definition of the transoral endoscopic thyroidectomy vestibular approach (TOETVA) technique, the identification and dissection of the RLN had to be changed to the craniocaudal approach in patients who undergo this procedure [8]. There are only a few studies in the literature that evaluated the morbidity rates of the craniocaudal approach or that compared the morbidity rates of craniocaudal and lateral approaches in open thyroidectomy (OT) [910111213]. The aims of our study were to compare the rates of adverse electromyographic (EMG) changes, loss of signal (LOS), and RLN injury in craniocaudal and lateral approaches to the RLN during thyroidectomy under CIONM, and to evaluate the clinicopathological and anatomical features which affected the occurrence of adverse EMG changes and LOS.
METHODS
This study was approved by the Ethics Committee of Sisli Hamidiye Etfal Training and Research Hospital (No. 935) and registered on ClinicalTrials.gov (NCT04379804). Informed consent was obtained from each patient.
Study design and patients
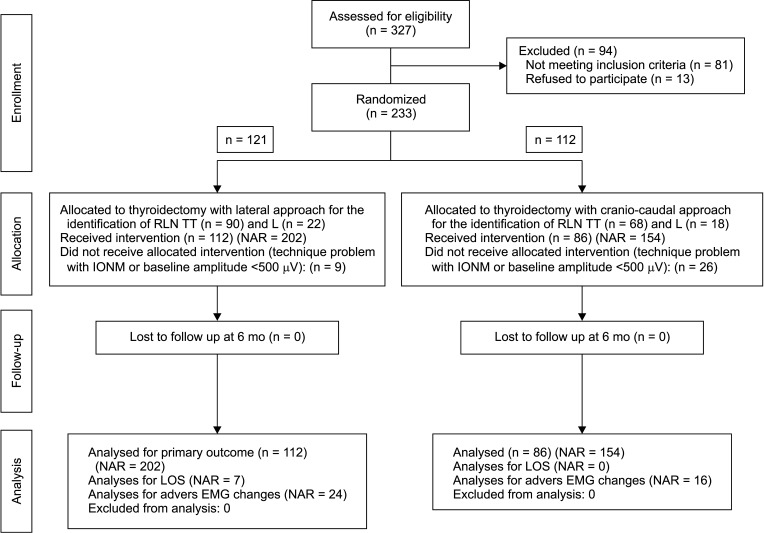
This prospective study was conducted in 2 tertiary referral centers of endocrine surgery. A total of 327 patients who were referred to undergo thyroid surgery between June 2018 and November 2019 were assessed for eligibility to participate in the study. Of these 327 patients, 233 were considered to be eligible for the study (Fig. 1). Exclusion criteria included previous thyroid or parathyroid surgery, substernal goiter, preoperative vocal cord palsy (VCP), evidence of lateral lymph node metastasis, intentional transection of the RLN due to tumor invasion, failure to assess real-time RLN functioning due to equipment issues with the IONM setup, presurgical dissection amplitude of <500 µV, and patient’s refusal to participate in the study. The equipment setup, anesthesia, standards of IONM, EMG definitions, and data interpretation of IONM were applied in accordance with the International Intraoperative Neural Monitoring Study Group (INMSG) guideline [2]. A small dose of a nondepolarizing muscle relaxant (e.g., rocuronium and atracurium at 0.5 mg/kg) was used at intubation [2]. At the onset of surgery, the stimulator probe was tested on the strap muscles to observe muscle twitching and to assure the absence of ongoing effects of the paralytic agent; otherwise, we used sugammadex to reverse neuromuscular blockade. It takes approximately 15 minutes after the skin incision to check V1, depending on the size of the thyroid gland on the operative side.
Age, sex, body mass index (BMI), the indications for surgery, presence of hyperthyroidism, evidence of autoimmune thyroid disease (ATD), and thyroid lobe volume were recorded in all patients, preoperatively. Thyroid lobe volume was calculated by using the dimensions (length [L], width [W], thickness [T]) of each thyroid lobe measured by ultrasonography according to the following formula; [14].
The patients were randomized to have RLNs identified by lateral (n = 121) or craniocaudal approach (n = 112) (Fig. 1). Simple randomization was performed by using computer-generated random numbers. The numbers were written on cards that were concealed in opaque envelopes. On the morning of the operation, 1 envelope was opened before the operation and, depending on the parity of the number, RLNs of the patient were dissected either by craniocaudal or lateral dissection during the operation. The patients and the nerves at risk (NARs) in the lateral and craniocaudal approach groups were classified as groups 1 and 2, respectively. In groups 1 and 2, 9 and 26 patients were further excluded intraoperatively, respectively, owing to failure to assess RLN functioning due to equipment issues with the IONM setup (n = 2) or presurgical dissection amplitude of <500 µV (n = 33). Failure to assess real-time RLN functioning due to equipment problems with the IONM setup was encountered in 2 patients. These problems included a stimulation side problem due to a blown-out fuse inside the connector box in 1 patient and poor stimulation due to a mismatch between a very thin vagus nerve and the automated periodic stimulation electrode in another patient.
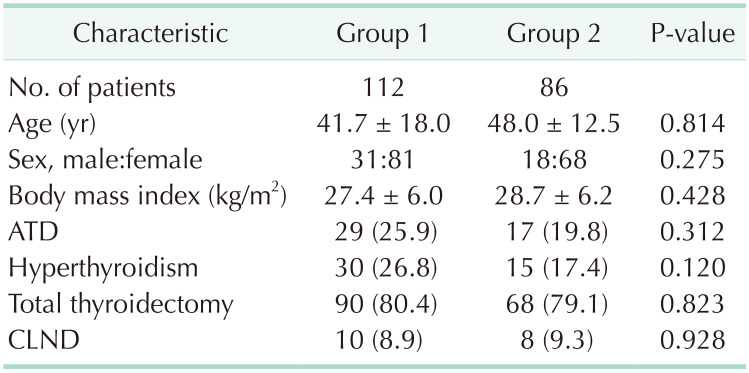
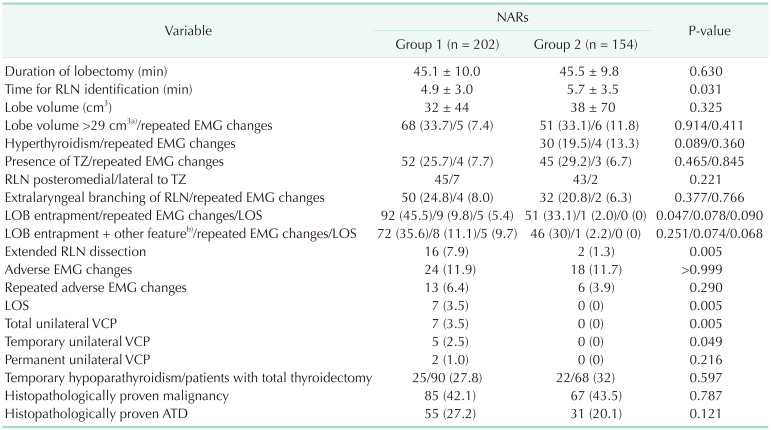
Of the remaining 198 patients, 112 were in the lateral approach group (group 1) and 86 in the craniocaudal approach group (group 2). The types of thyroid surgery in both groups are summarized in Table 1. Groups 1 and 2 consisted of 202 (56.7%) and 154 (43.3%) NARs, respectively (Table 2).
All NARs were dissected by using CIONM including vagal response evaluation at the beginning and at the end of the operation (IONM: L1, V1, R1, R2, V2, L2) according to the recommendations by the INMSG [7]. CIONM had been carried out with 1 of the 2 following commercially available neuromonitoring devices: (1) NIM 3.0 Nerve Monitoring Systems (Medtronic Xomed, Jacksonville, FL, USA) or (2) Avalanche SI (Dr. Langer Medical GmbH, Waldkirch, Germany).
All patients underwent pre- and postoperative laryngoscopic examination within 2 days after surgery and repeated serially if abnormal (L1, L2). All operations were performed by experienced endocrine surgeons. The length of RLN dissection was defined as extended if the nerve was dissected for 5 cm or greater. Duration of lobectomy for each site, period of time for RLN identification, the relationship of the RLN to the ligament of Berry (LOB) and to the tubercle of Zuckerkandl (TZ), extralaryngeal branching of the RLN, length of RLN dissection, adverse EMG changes and LOS were recorded in all patients. The rates of postthyroidectomy hypoparathyroidism and VCP were recorded. Final histopathological diagnosis was documented in all patients, postoperatively.
The primary endpoint of the study was RLN injury and the secondary endpoints included the effect of clinicopathological features, anatomic variations, and adverse EMG changes on the occurrence of RLN injury.
Thyroid surgery and continuous intraoperative nerve monitoring technique
The first 2 steps of thyroidectomy were the same in both groups of patients. Following skin incision and creation of skin flaps, the strap muscles were split in the midline. The first step of thyroidectomy was the division of the isthmus. Then, the strap muscles were dissected away from the thryoid lobe and retracted laterally. The middle thyroid vein was ligated and an automated periodic stimulation electrode was placed on the vagus in both groups of patients. In the second step, the upper pole of the thyroid gland was retracted laterally in order to proceed with dissection in the avascular space between the lobe and the cricothyroid muscle. At this step, the external branch of the superior laryngeal nerve (EBSLN) was identified visually and/or by using a neuromonitoring hand probe prior to dissection of the upper pole vessels. The branches of upper pole vessels were ligated individually on the thyroid capsule away from the course of the EBSLN. Further steps of thyroidectomy differed in craniocaudal and lateral approach groups.
Craniocaudal approach
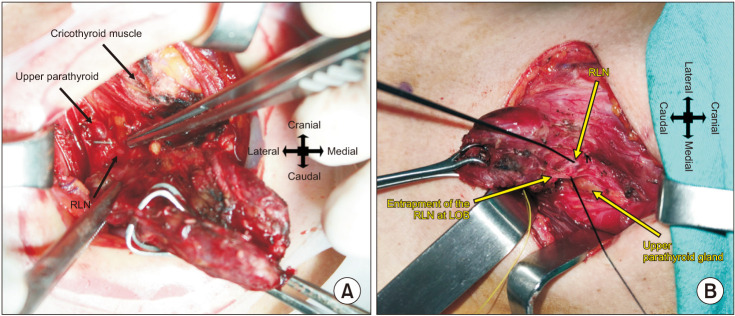
In the third step, the upper pole was retracted gently in the anterolateral direction in order to expose the cricothyroid and cricopharyngeal muscles. The RLN passes deep to the lower border of the cricopharyngeal muscle and behind the cricothyroid joint, and finally enters into the larynx. We reached the lower part of the cricopharyngeal muscle. The upper parathyroid gland was identified and dissected away from the thyroid gland by capsular dissection and by preserving the vascular supply. At this step, we used a neuromonitoring hand probe to help the detection of the RLN prior to visual identification at the lower border of the cricopharyngeal muscle and the posterior aspect of the upper parathyroid gland (Fig. 2A). There are often numerous arterial branches and fascial bands close to the nerve at the point of laryngeal entry and the nerve courses between the fascial layers of LOB caudally. Nerve monitoring was very helpful in distinguishing the RLN from arterial branches and fascial bands and safely mapping the course of the nerve between the fibrous and fascial layers of the LOB (Fig. 2B). The RLN was subsequently identified visually by capsular dissection on the posterior surface of the thyroid lobe. Then, the fibrous and vascular layers of LOB were dissected step by step in the anteromedial aspect of the RLN. The RLN dissection was proceeded craniocaudally through the level of inferior thyroid artery (ITA). As the last step, the inferior vessels of the thyroid gland were dissected and ligated (Fig. 2D). Then, the lobe was dissected from the trachea, and lobectomy was completed.
Lateral approach
At the third step, the thyroid lobe was mobilized anteromedially and the strap muscles were retracted laterally. Then, the RLN was sought within the Beahrs’ triangle which is bounded by the common carotid artery as base, ITA superiorly, and RLN as the third side [15]. The RLN was initially detected and mapped by using a neuromonitoring hand probe. Subsequently, the tissue within the Beahrs’ triangle was dissected gently parallel to the direction of the nerve until the nerve is identified visually. After the visual identification of the RLN, the inferior thyroid vessels were ligated. The nerve was dissected along its course to the laryngeal entry point. As the last step, the thyroid lobe was totally dissected from the trachea and the lobectomy was completed.
Identification and preservation of all parathyroid glands and their vascular supply were tried in all cases by performing capsular dissection of the thyroid gland. In case of incidental parathyroidectomy or totally compromised vascularity of the parathyroid glands, autotransplantation into the sternocleidomastoid muscle was performed.
During the operations, adverse EMG parameters were defined as an amplitude decrease of 50% or more of the baseline value, or a latency increase of 10% or more [2]. A combined event (CE) was defined as a concordant amplitude decrease of more than 50% and latency increase of more than 10% regarding baseline values [2]. The surgical maneuver was immediately altered and the traction was released if adverse EMG changes were noted during surgery and delayed to achieve recovery of EMG changes. Recovery was defined as amplitude recovery to >50% of the initial baseline amplitude. LOS was defined as an amplitude of <100 µV [16]. In the case of LOS during the surgery of the initial site, contralateral surgery was aborted if the amplitude did not recover to greater than 50% of the initial baseline amplitude within 20 minutes of the initial decline.
Statistical analyses
The IBM SPSS Statistics ver. 21.0 (IBM Corp., Armonk, NY, USA) was used for statistical analysis. The continuous variables are summarized as mean ± standard deviation. The differences between the groups were assessed using the Student t-test and a Mann-Whitney U-test for normally distributed and nonnormally distributed data, respectively. The univariate analysis by chi-square test and Fisher exact test were performed to test differences in proportions. Receiver operating characteristic (ROC) analysis was performed to determine the cutoff value of the thyroid lobe volume between the NARs with and without repeated adverse EMG changes. Statistically significant results obtained from the univariate analysis were subjected to multivariate logistic regression. A P-value of <0.05 was considered to be statistically significant.
RESULTS
Preoperative findings
The indications for surgery were nodular goiter with compressive symptoms in 95 (48.0%), indeterminate, suspicious for malignancy or malignant cytology in 58 (29.3%), Graves disease in 26 (13.1%), multinodular toxic goiter in 15 (7.6%), and toxic adenoma in 4 patients (2.0%). Preoperative laryngoscopy revealed normal vocal cord function in all patients. Groups 1 and 2 showed no significant difference in the aspect of demographic data, BMI, the rates of hyperthyroidism, ATD, and the extent of thyroid surgery (Table 1). The mean volume of individual thyroid lobes in groups 1 and 2 was calculated as 32 ± 44 cm3 and 38 ± 70 cm3, respectively (P = 0.300) (Table 2).
Intraoperative findings
Duration of lobectomy was similar in both groups but the mean period for RLN identification was significantly longer in group 2 compared to group 1 (P = 0.030) (Table 2). TZ was identified in 97 of 356 excised lobes (27.2%) and the RLN was located in the posteromedial aspect of TZ in 88 of 97 TZ (90.7%), and lateral to the TZ in the remaining 9 lobes (9.3%). The rates of TZ and the relationship of TZ to RLN showed no significant difference between groups 1 and 2 (P = 0.500 and P = 0.100, respectively) (Table 2). Extralaryngeal branching of RLN was found in 82 of 356 NARs (23.3%) and the rate of extralaryngeal branching in groups 1 and 2 was not significantly different (P = 0.300) (Table 2). Entrapment of RLN by vascular structures or fibrous bands at the LOB was detected in 143 of 356 NARs (40.2%), and the rate of RLN entrapment was significantly higher in group 1 compared to group 2 (P = 0.047) (Table 2). Extended RLN dissection was performed in 16 (7.9%) and 2 NARs (1.3%) in groups 1 and 2, respectively (P = 0.005).
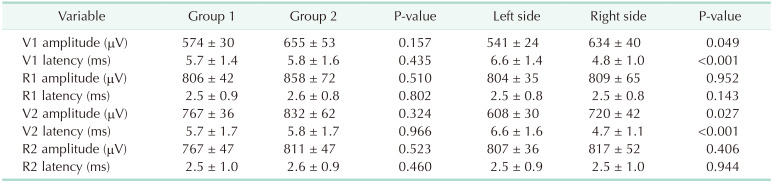
The mean values of presurgical and postsurgical dissection amplitude and latency were not significantly different between groups 1 and 2 (Table 3). The mean V1 and V2 latencies of the right vagus nerve were significantly shorter than the V1 and V2 latencies of the left vagus nerve (P < 0.001) (Table 3). The mean V1 and V2 amplitudes of the right vagus nerve was significantly higher than the V1 and V2 amplitudes of the left vagus nerve (P = 0.049 and P = 0.027, respectively) (Table 3). The mean R1 and R2 latencies and amplitudes showed no significant difference between the right and the left RLN.
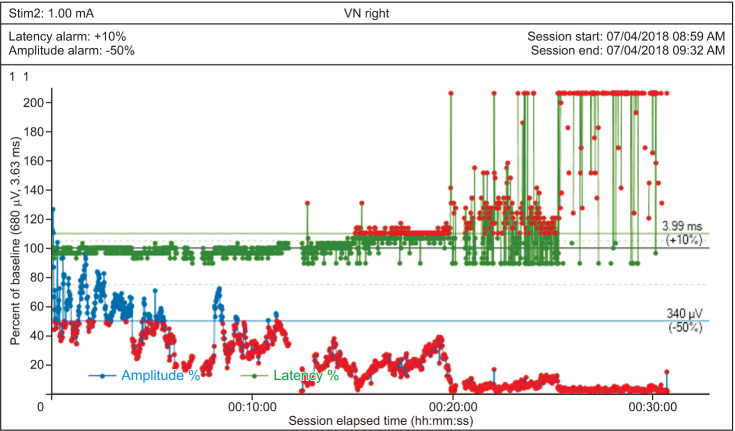
LOS occurred in 7 of 356 NARs (2.0%). Adverse EMG changes were encountered in 42 NARs (11.8%) during lobectomy and recovered after the release of traction in all of these 42 NARs. The mean recovery time was 2.2 ± 1.7 minutes. Of these 42 NARs that achieved recovery, 19 (45.2%) developed repeated adverse EMG changes and CE during further dissection, despite the alteration of surgical maneuver and release of traction. LOS occurred in 7 of these 19 NARs (36.8%) (Fig. 3). The mechanism of RLN injury in 7 NARs was considered to be stretching of the nerve because none of the LOS was associated with inadvertent ligation or clamping of the RLN or thermal injury. Of the 7 NARs with LOS, LOS occurred during the initial site of surgery in 1, and staged thyroidectomy was performed in this patient 3 months after primary surgery when vocal cord function was verified to have recovered by laryngoscopic examination.
Correlation between the adverse electromyographic changes, loss of signal, and clinicopathological and anatomical features
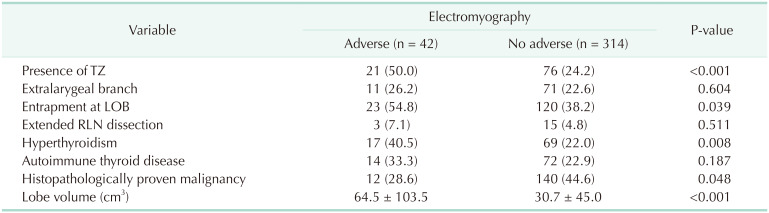
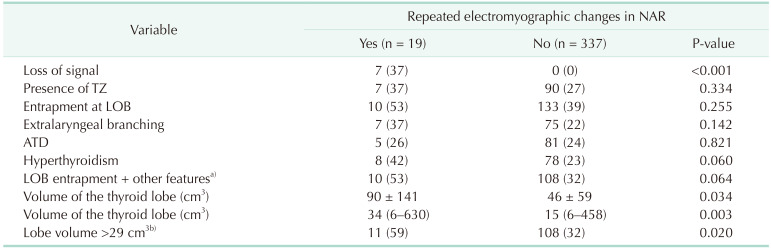
The presence of TZ, RLN entrapment at the LOB, hyperthyroidism and large thyroid volume were significantly correlated with the occurrence of adverse EMG changes when the NARs with and without adverse EMG changes were compared by univariate analysis (Table 4). Extralaryngeal branching, ATD, and extended RLN dissection were found to have no significant correlation with the occurrence of adverse EMG changes (Table 4). Binominal logistic regression analysis revealed that the presence of TZ and high thyroid volume were the most significant factors associated with adverse EMG changes. Repeated adverse EMG changes and CE were significantly correlated with LOS (P = 0.001) (Table 5). When we compared the NARs with and without repeated adverse EMG changes, the median thyroid lobe volume was found as significantly higher in 19 NARs with repeated adverse EMG changes compared to those 337 with no repeated adverse EMG changes (34 cm3
vs. 15 cm3, respectively; P = 0.003) (Table 5). The ROC curve analysis identified lobe volume >29 cm3 (ROC area, 0.701; standard error, 0.003) as the cutoff value with maximum accuracy to predict repeated adverse EMG changes. The rate of the thyroid lobes with a volume of >29 cm3 was significantly higher in the NARs with repeated adverse EMG changes compared to those without repeated adverse EMG changes (59% vs. 2%, respectively; P = 0.020) (Table 5).
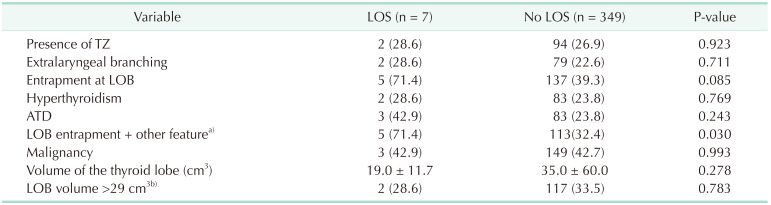
The rate of the nerve entrapment at the LOB alone or accompanied by 1 or more of other clinicopathological or anatomical features (including TZ, extralaryngeal branching, hyperthyroidism, ATD, or lobe volume of >29 cm3) was higher in the NARs with repeated adverse EMG changes compared those with no repeated adverse EMG changes, but the difference was not statistically significant (Table 5). However, the NARs with LOS had a significantly higher rate of entrapment at the LOB which was accompanied by 1 or more of the other clinicopathological or anatomical features compared to those with no LOS (71.4% vs. 32.4%, P = 0.020) (Table 6).
Adverse electromyographic changes and loss of signal in lateral and craniocaudal approach groups
The rates of adverse and repeated adverse EMG changes were similar in groups 1 and 2, but the rate of LOS was significantly higher in group 1 (Table 2). There were 7 LOSs (3.5%) in group 1 while no LOS was recorded in group 2. The rates of repeated adverse EMG changes in the NARs of the patients with and without hyperthyroidism, ATD, extralaryngeal branching, TZ, and lobe volume of >29 cm3 were similar in groups 1 and 2 (Table 2). In group 1, of the 13 NARs which developed repeated adverse EMG changes, 9 (69.2%) had entrapment at the LOB. Eight of these 9 NARs (88.9%) also had 1 or more clinicopathological or anatomic features which accompanied the LOB entrapment, and LOS was recorded in 5 of these 8 NARs (62.5%). In group 2, of the 6 NARs that developed repeated adverse EMG changes, 1 (16.7%) had entrapment at the LOB that was accompanied by TZ and extralaryngeal branching, and no LOS was recorded in these 6 NARs in group 2 (Table 2). The rate of the NARs with entrapment at the LOB that is accompanied by other clinicopathological or anatomical features was not significantly different between groups 1 and 2 (35.6% vs. 29.9%, respectively; P = 0.200) (Table 2). However, the rate of repeated adverse EMG changes and LOS in the NARs with LOB entrapment accompanied by other clinicopathological and anatomical features was higher in group 1 compared to those in group 2, but the difference did not achieve statistical significance (11.1% vs. 2.2%, respectively and 9.7% vs. 0%, respectively; P = 0.070) (Table 2).
Postoperative results
Temporary hypoparathyroidism was found in 47 of 158 patients (29.7%) who underwent total thyroidectomy. The rate of temporary hypoparathyroidism showed no significant difference between the patients in groups 1 and 2 (28% vs. 32%, respectively; P = 0.500) (Table 2). The total rate of unilateral VCP was 3.5% in 198 patients and 2.0% in 356 NARs. Unilateral VCP was detected by L2 in all 7 patients with intraoperative LOS. Vocal cord function recovered in 5 of these 7 patients within 4 months after surgery. The rates of temporary and permanent VCP were 2.5% and 1.0% in 198 patients; and 1.4% and 0.6% in 356 NARs. All of the 7 LOS and unilateral VCP occurred in the patients in group 1. The total rate of VCP was significantly higher in NARs in the lateral approach group compared to those in the craniocaudal approach group (3.5% vs. 0%, respectively; P = 0.005) (Table 2). The rate of permanent VCP showed no significant difference between the groups 1 and 2 (0.9% vs. 0%, respectively; P = 0.100) (Table 2).
DISCUSSION
The approaches to identify the RLN during thyroid surgery include lateral, inferior, superior, and medial approaches, and the method of RLN dissection may vary according to the circumstances and surgeon preference. The lateral approach is the most common method for dissection of the RLN during routine thyroidectomy, but the superior approach is seldom used [17]. Recently, TOETVA was introduced as a natural orifice and non-scar thyroidectomy technique [8]. In OT, the approach to the RLN might be selected or changed intraoperatively according to the surgeon’s preference or characteristics of thyroid disease or thyroid gland anatomy. However, TOETVA procedure is performed with a top-down approach and the RLN is first identified at its insertion point and dissected in a craniocaudal manner [18].
A revision of studies including large numbers of patients revealed that the rates of permanent RLN injury and hypoparathyroidism following thyroidectomy in experienced hands ranged from 0.2% to 6.6% and to 3%, respectively [19]. There are few studies in the literature evaluating morbidity rate related to the craniocaudal approach to RLN in OT [910111213]. In these studies, the rate of permanent VCP and hypoparathyroidism was reported to range between 0%–0.4%, and 0%–3%, respectively [910111213]. Page et al. [20] suggested that the superior approach could be useful in cases of the presence of fibrous adherences in reoperations, large goiters with retrosternal extension, morphological variations as short neck, or lack of neck extension which obscures the identification of RLN at the level of ITA. There is a prospective study in the literature that compared the morbidity rates in patients who received superior-inferior or inferior-superior approach to the RLN during thyroidectomy without using IONM [10]. In a study by Veyseller et al. [10], the authors reported a significantly higher rate of complications in the inferior-superior approach group compared to the superior-inferior approach group.
The mechanisms of RLN injury include thermal trauma, transection, ligation, clamping, traction, or compression. Routine nerve identification and the use of IONM as a supplement revealed that traction injury was the most common cause of RLN injury [21]. The most common sites for potential traction injury include LOB and the level of ITA or in case of adhesions to the tumor or goiter capsule [2223]. The development of RLN injury due to stretching is affected by the degree, duration, and direction of the traction [2425]. Phelan et al. [6] and Schneider et al. [7] documented a significantly increased risk of VCP when CE occurred for 40 seconds or longer. These adverse EMG changes were found to be reversible in 70%–80% of the patients when the traction was released immediately at the onset of CE [6]. However, multiple CEs were found to result in LOS and VCP in 50% of such patients [67]. CIONM may reveal an imminent injury timely enough to allow the surgeon to stop harmful dissection and allow the nerve to recover [67].
The region of Berry ligament was found to be the area of greatest risk for RLN injury in many studies [262728]. Chiang et al. [22] documented that 75% of LOS resulted from overstretching of the nerve at the level of LOB and stated that excessive traction on the thyroid could not be avoided particularly in RLNs which coursed through the LOB. Large-sized TZ was also reported as another significant risk factor that increased the rate of transient RLN palsy during thyroid surgery [212223242526272829].
In our study, we found that the presence of TZ, RLN entrapment at the LOB, hyperthyroidism, and large thyroid lobe volume were significantly correlated with the occurrence of intraoperative adverse EMG changes. The presence of TZ and high thyroid lobe volume were the most significant factors associated with adverse EMG changes. High thyroid lobe volume was also significantly associated with repeated adverse EMG changes and CE. The ROC curve analysis identified lob volume of >29 cm3 as the cutoff value with maximum accuracy to predict the repeated adverse EMG changes. Although the rate of fibrous or vascular entrapment at the LOB was about 2-fold higher in the NARs with LOS compared to those without LOS, the difference was not statistically significant. However, we observed that RLN entrapment at the LOB that was accompanied by 1 or more of the other features, including TZ, extralaryngeal branching, hyperthyroidism, ATD, or lobe volume of >29 cm3, significantly increased the risk of LOS.
To our knowledge, our study is the first study in the literature that evaluated the real-time EMG parameters and the rate of RLN injury in craniocaudal and lateral approaches to the RLN by using CIONM. In our study, real-time EMG parameters revealed no significant difference in the rate of adverse or repeated adverse EMG changes between craniocaudal and lateral approaches to the RLN, but the rate of LOS was significantly higher in the lateral approach group. Repeated adverse EMG changes and CE were significantly associated with LOS. We showed that a lateral approach to the NARs with entrapment at the LOB resulted in an approximately 5-fold higher rate of repeated adverse EMG changes compared to the craniocaudal approach. The rate of LOS in the NARs with LOB entrapment accompanied by 1 or more of the other features, such as TZ, extralaryngeal branching, hyperthyroidism, ATD, or lobe volume of >29 cm3, was 9.7% in the lateral approach group whereas none of the NARs with these features developed LOS in the craniocaudal approach group. The total rate of VCP was significantly higher in the lateral approach group compared to the craniocaudal approach group, but the rate of permanent VCP showed no significance between the 2 groups. This finding is compatible with the findings of a previous study which found a higher rate of VCP after the inferior-superior approach vs. the superior-inferior approach to the RLN [10]. However, the effect of these 2 approaches on the rate of RLN injury was not evaluated in terms of the real-time EMG changes associated with the presence of clinicopathological and anatomical variations in that study.
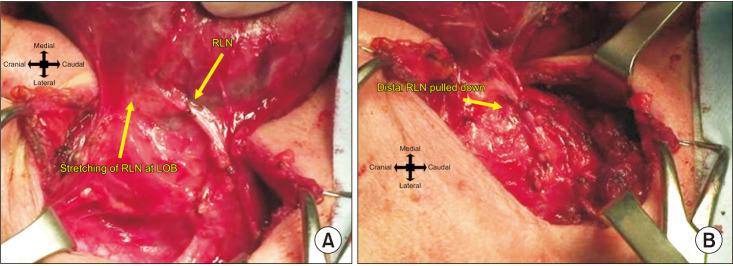
The findings of our study suggest that the craniocaudal approach is safer than the lateral approach in respect of RLN injury in NARs with LOB entrapment alone or coexistent with other clinicopathological and anatomical features. In the RLNs with entrapment at the LOB, a stretch injury may develop by direct distress of the stretching ligament on the RLN or by pulling down the distal part of the RLN which is already excessively stretched through the LOB during anteromedial retraction of the thyroid lobe [22232425262728] (Fig. 4). We thought that entrapment at the LOB caused excessive traction to the RLN at the points of fixation when the thyroid lobe is retracted anteromedially in the lateral approach technique and resulted in a higher rate of LOS compared to the craniocaudal approach. The craniocaudal approach to the RLN allows initial identification of the nerve at a constant anatomical landmark. The position of the RLN is fixed at the cricothyroid junction and is not affected by anatomical variations. Contrary to the lateral approach, craniocaudal dissection of the RLN can be achieved under vision through the anteromedial plane of the nerve with no need for any significant anteromedial mobilization or retraction of the thyroid lobe.
The RLN is anatomically positioned in a course between the 2 fixed points. The first fixed point of the RLN is at the level of laryngeal entry and the second one is at the level of its loop around the right subclavian artery on the right side or around the aortic arch on the left side. The RLN courses along in a plane posterior to LOB and then turns medially and forms an anatomical ‘genu’ while entering the larynx at the superior aspect of the ligamentous tissue [12]. Serpell et al. [30] made a computer model which represented the formation of an artificial RLN genu during thyroidectomy when the thyroid lobe is rotated anteromedially. The authors demonstrated that the maximal tension was located at the genu and the final 2-cm segment of the nerve when the RLN was laterally retracted by 2 cm at a point 2 cm from a fixed end. Higher rates of RLN injury associated with the lateral approach may be possibly explained by greater tension applied to the distal segment of the nerve, which lies between the 2 fixed points when the thyroid lobe is retracted. In the craniocaudal approach, the nerve is initially released from the thyroid gland at the site of laryngeal entry and 1 of the 2 fixed points is eliminated as a first step. Early release of the nerve at the distal fixed point, where the RLN is most vulnerable to injury, might decrease the tension applied to the nerve at this point during anteromedial retraction of the thyroid lobe and might result in decreased risk of RLN injury, especially in NARs with LOB entrapment.
Another potential advantage of the craniocaudal approach includes less risk of impairing the blood supply to the inferior parathyroid gland. Although a previous study [10] found a significantly lower rate of hypoparathyroidism after the superior-inferior approach to the RLN compared to the inferior-superior approach, the rates of hypoparathyroidism were similar after both approaches in our study.
The period for RLN identification was longer in the craniocaudal approach than in the lateral approach in our study. There are often small arterial branches that are placed in close proximity to the RLN at the point of laryngeal entry which interferes with the identification of the RLN. Meticulous dissection should be performed to avoid bleeding from these small vessels. RLN injury may occur during hemostasis of the bleeding from these small vessels, which are very close to the RLN. It may be difficult to identify the RLN between the fibrous and vascular layers of the LOB. Therefore, we think that teaching craniocaudal dissection is more difficult than the lateral approach and the use of a neuromonitoring hand probe is very helpful in the craniocaudal approach in order to distinguish these small vessels from the RLN, to map the nerve, and to provide safe hemostasis. We also think that it is best to use nerve monitoring while teaching the craniocaudal approach to surgeons who are not familiar with this technique, as this will provide better anatomical orientation and safer RLN dissection.
In conclusion, although the real-time EMG changes during craniocaudal and lateral approaches to the RLN revealed no significant difference in terms of adverse or repeated adverse EMG changes, the rate of RLN injury was higher in the lateral approach compared to the craniocaudal approach. The presence of TZ, entrapment at the LOB, hyperthyroidism, and high thyroid lobe volume significantly increased the rate of adverse EMG changes. The coexistence of LOB entrapment with the TZ, extralaryngeal branching, hyperthyroidism, ATD, or high lobe volume significantly increased the rate of LOS. In NARs with entrapment at the LOB, the lateral approach resulted in a higher rate of RLN injury compared to the craniocaudal approach. A higher rate of injury in NARs with entrapment at the LOB may be explained by greater tension applied to the distal segment of the nerve by anteromedial retraction of the thyroid lobe during the lateral approach. We suggest that the use of the craniocaudal approach to the RLN might decrease the rate of repeated adverse EMG changes and nerve injury in RLNs with entrapment at the LOB alone or combined with other clinicopathological features or anatomical variations.
 XML Download
XML Download