

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Angina and its equivalent symptoms are a common presentation for outpatients, accounting for approximately 1–2% of hospital visits.1) However, optimal evaluation and accurate diagnosis is challenging given the wide range of possible etiologies of chest pain from benign to life-threatening conditions. Thus, millions of cardiac noninvasive tests have been performed to identify the origin of chest pain in clinical practice.2)3)
Invasive coronary angiography (ICA) is the final determining test in the diagnostic process of coronary artery disease (CAD) and may be followed by coronary revascularization procedures. Given the invasiveness of ICA and advances in the diagnostic accuracy of other non-invasive modalities to identify CAD, ICA should be reserved for patients with highly suspected CAD who require revascularization. Therefore, professional guidelines recommend the use of various cardiac noninvasive tests, such as the exercise treadmill test (TMT), functional tests including single-photon emission computed tomography (SPECT), and coronary computed tomography angiography (CCTA), for patients with stable chest pain due to suspected CAD prior to ICA.4)5)6) However, despite strategies to reduce unnecessary ICA in patients with suspected CAD, the diagnostic yield of significant CAD requiring revascularization was still low in previous studies.7)8)9)
Since the launch of the 64-detector row computed tomography (CT) scanner, CCTA has demonstrated excellent diagnostic accuracy in detecting obstructive CAD compared to other non-invasive imaging modalities.10) Furthermore, CCTA has improved gatekeeping capability compared to ICA, particularly in terms of reducing the rate of absence of significant CAD findings when ICA was performed in earlier prospective trials.11)12)13) Therefore, the increased use of CCTA as a gatekeeper for ICA and for preventing unnecessary ICA in patients with suspected CAD is expected in the real world. However, there is limited literature on real-world evidence showing trends in the utility of CCTA as a gatekeeper.
Thus, we sought to evaluate the trends in the utility of non-invasive gatekeeping studies, including CCTA, TMT, and SPECT among those with suspected CAD using the nationwide claims database of the National Health Insurance in Korea.
METHODS
Ethical statement
This study was approved by the Institutional Review Board (Chung-Ang University Hospital IRB No. 2103-003-19357), and the requirement for written informed consent was waived because all personal data were removed and coded as arbitrary numbers.
Data sources
Data from the Health Insurance Review and Assessment Service (HIRA)-National Patient Samples (NPS) were used. The HIRA has been receiving claims made by all medical institutions in Korea since 2000. The HIRA database includes personal and medical information, such as age, sex, diagnoses, and surgical or medical treatment of approximately 50 million Koreans. The diagnoses were coded according to the International Classification of Diseases, 10th Revision (ICD-10). The HIRA-NPS is a stratified random sample of 3% of the population in the HIRA data using 16 age groups and two sex groups. Each year, the data are newly extracted; thus, the data of individual patients could not be continuously followed up.
Study population
From the HIRA-NPS database between 2012 and 2018, we identified patients visiting outpatient clinic with clinical diagnoses of angina pectoris (I20), other symptoms and signs involving the circulatory and respiratory systems (R09), pain in throat and chest (R07), atherosclerosis (I70), and abnormalities of breathing (R06). Among them, we identified patients who performed any of the gatekeeping studies, including CCTA (HA474), TMT (E6543), and SPECT (HC292, HC297, HC298, HC301, HC302, HC303, HC304, and HC305) and those who directly performed ICA (HA670) without gatekeeping study. Then, we excluded patients <40 years because of a higher likelihood of congenital or nonatherosclerotic causes of obstructive CAD (n=9,721). Patients who had codes for previous coronary catheterization (HA670) or revascularization (percutaneous coronary intervention [PCI], M6561, M6562, M6563, M6564, M6565, M6566, and M6567; coronary artery bypass graft [CABG], O1640, O1641, O1642, O1647, O1648, O1649, OA640, OA641, OA642, OA647, OA648, and OA649) and for heart failure (I50) before the index tests and were also excluded (n=5,693). In addition, patients who underwent index tests in December were excluded as they may have undergone coronary procedures a year later (n=4,373). Finally, 71,401 patients were included in this study (Figure 1). Baseline information, including age and sex, was obtained, comorbid conditions were assessed based on ICD-10 codes, and the Charlson comorbidity index (CCI), a method of categorizing comorbidities of patients based on the ICD codes, was calculated.14) In addition, patients who underwent downstream ICA and revascularization procedures, including PCI and CABG, after the index tests were identified.
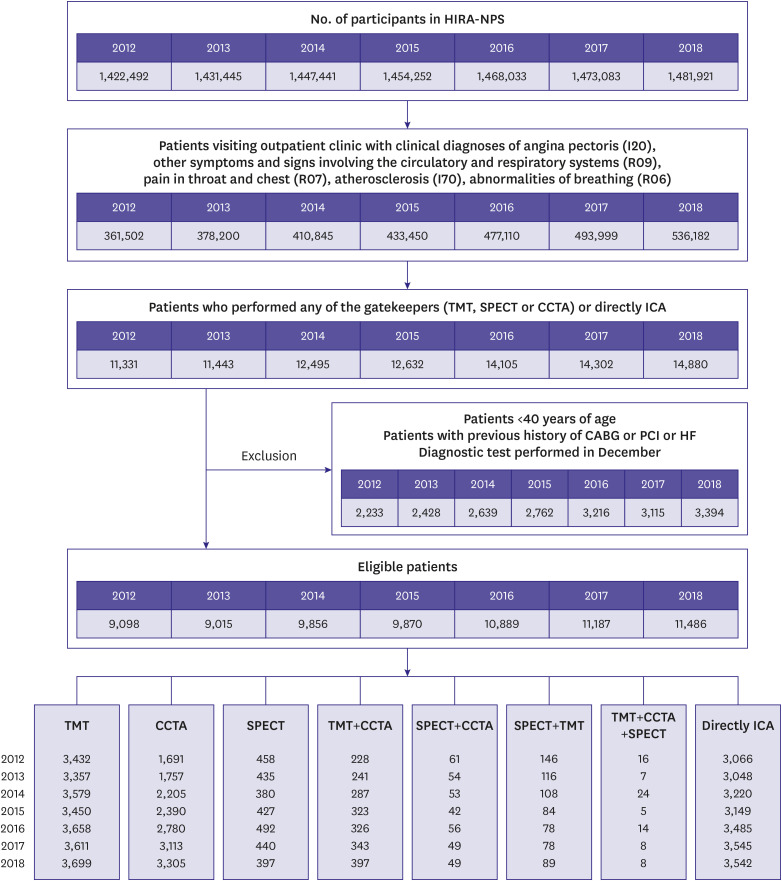
Figure 1
Identification of the study population.
CABG = coronary artery bypass grafting; CCTA = coronary computed tomography angiography; HF = heart failure; HIRA = Health Insurance Review and Assessment Service; ICA = invasive coronary angiography; NPS = National Patient Sample; PCI = percutaneous coronary intervention; SPECT = single-photon emission computed tomography; TMT = treadmill test.
![]()
Statistical analysis
Categorical variables are presented as percentages, and continuous variables are described as means with standard deviations. The χ2 tests and Fisher’s exact tests were performed to compare the baseline characteristics and rates of downstream ICA and coronary revascularization among the three gatekeeping tests. Student’s t-test and analysis of variance were used to compare the CCI. A simple linear regression analysis was used to show the time trends of each gatekeeper and ICA. Annual percent change and confidence interval (CI) were calculated using the Joinpoint software ver. 4.2.0.2 from the Surveillance Research Program of the United States National Cancer Institute. The estimated target population and frequency was validated by using PROC SURVEY-FREQ of SAS ver. 9.4. The survey procedure of SAS ver. 9.4 is used to calculate estimated number of target population, standard errors, and CI from the sample datasets. For SURVEY procedure, the sampling weights from HIRA-NPS Table 20 (general specifications) was used, which was used for the stratified sampling into a total of 32 strata (2 stratum of sex and 16 stratum of age). Statistical analyses were performed using SAS software (version 7.1; SAS Institute, Cary, NC, USA).
RESULTS
Baseline characteristics
The baseline characteristics of the patients who underwent TMT (n=24,786; 34.7%), SPECT (n=3,029; 4.2%), CCTA (n=17,241; 24.2%), both of CCTA and TMT (n=2,145; 3.0%), both of CCTA and SPECT (n=364; 0.5%), both of TMT and SPECT (n=699; 1.0%), and triple of TMT, CCTA and SPECT (n=82; 0.1%) as gatekeeping modalities, and those who directly underwent ICA without gatekeeping study (n=23,055; 32.3%) for suspected CAD are summarized in Table 1 and Supplementary Table 1. Among patients who underwent TMT, SPECT, CCTA, and directly ICA, the distribution of patients’ age, sex, comorbid conditions, and CCI differed significantly (p<0.001). The clinical diagnoses also differed significantly according to the utility and type of the gatekeepers (p<0.001). The time interval from index study to ICA did not differ significantly according to the gatekeeping modality (p=0.367).
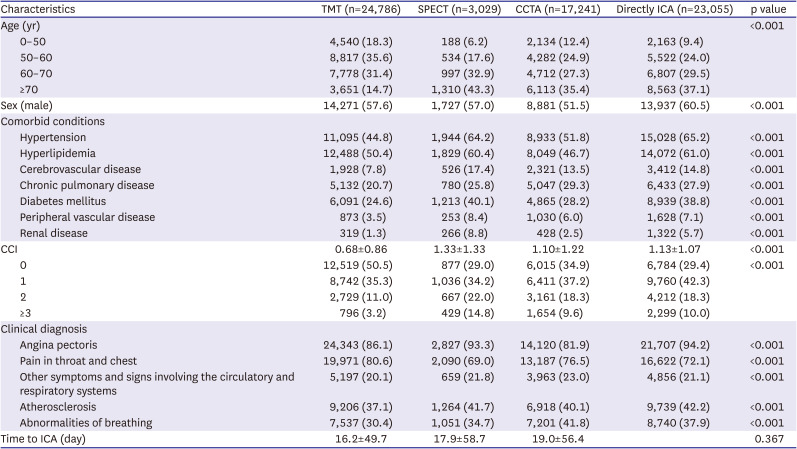
Table 1
Baseline characteristics of the patients according to the utility and type of gatekeeping modalities for suspected coronary artery disease
Values are presented as number (%) or mean ± standard deviation. ICD-10 codes for comorbid conditions and clinical diagnosis: Hypertension = I10, I11, I12, I13, I14, I15, Hyperlipidemia = E78, Cerebrovascular disease = G45, G46, I60, I61, I62, I63, I64, I65, I66, I67, I68, I69, chronic pulmonary disease = J40, J41, J42, J43, J44, J45, J46, J47, J60, J61, J62, J63, J64, J65, J66, J67, diabetes mellitus = E10, E11, E12, E13, E14, peripheral vascular disease = I70, I71, renal disease = N18, N19, Angina pectoris = I20, Pain in throat and chest = R07, Other symptoms and signs involving the circulatory and respiratory systems = R09, Atherosclerosis = I70, Abnormalities of breathing = R06.
CCI = Charlson comorbidity index; CCTA = coronary computed tomography angiography; ICA = invasive coronary angiography; ICD-10 = International Classification of Diseases, 10th Revision; SPECT = single-photon emission computed tomography; TMT = treadmill test.
![]()
In patients older than 65 years, the utility of CCTA (28.7%) was more common than those of SPECT (6.3%) and TMT (24.2%). On the contrary, TMT (45.7%) was the most frequently performed gatekeeper, followed by CCTA (22.7%) and SPECT (3.1%) in patients aged under 65 years. In terms of sex, CCTA showed relative female predominance compared to TMT and SPECT (p<0.001). The mean CCI of patients who underwent TMT (0.68±0.86) was the lowest, followed by those from CCTA (1.10±1.22) and SPECT (1.34±1.33), respectively (p<0.001) (Table 2).

Table 2
Comparison of the prevalence of gatekeeping studies according to the age, sex and CCI
The p value <0.013 is considered significant.
CCI = Charlson comorbidity index; CCTA = coronary computed tomography angiography; ICA = invasive coronary angiography; SPECT = single-photon emission computed tomography; TMT = treadmill test.
*Percentages were calculated with the total 100% per each age and sex group.
![]()
Temporal trends of the gatekeeping studies for stable chest pain
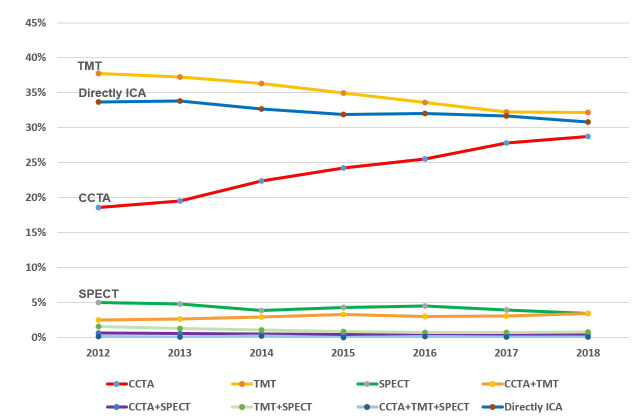
Table 3 summarizes the annual number of patients who underwent index studies. During the 7-year observational period, the number of patients who evaluated for suspected CAD has consistently increased significantly (9,098 in 2012 and 11,486 in 2018; β=447.9; p<0.001). Linear regression analyses showed that the number of CCTA (1,191 in 2012 and 3,305 in 2018; β=290.3; p<0.001), TMT (3,432 in 2012 and 3,699 in 2018; β=49.6; p=0.020), and direct ICA without gatekeeper (3,066 in 2012 and 3,542 in 2018; β=96.0; p=0.003) have been significantly increased. The number of SPECT, however, did not show significant change (p=0.787). The calculated annual percent changes were +1.81%p (95% CI, 1.62%p to 1.99%p) for CCTA, −1.04%p (95% CI, −1.15%p to −0.93%p) for TMT, −0.18%p (95% CI, −0.31%p to −0.05%p) for SPECT, and −0.50%p (95% CI, −0.65%p to −0.35%p) for directly ICA, respectively. In terms of the proportions of each study, CCTA showed an increasing linear trend as a gatekeeper (18.6% in 2012 and 28.8% in 2018; β=0.018; p<0.001). In contrast, the proportions of TMT (37.7% in 2012 and 32.2% in 2018; β=−0.010; p<0.001), SPECT (5.0% in 2012 and 3.5% in 2018; β=−0.002; p=0.03), and directly ICA (33.7% in 2012 and 30.8% in 2018; β=−0.005; p<0.001) decreased significantly during the observational period. For elderly population aged 65 and more, the trends for the utilization of diagnostic studies were consistently observed. The estimated number and proportion of target population for each year according to the gatekeeping modality is demonstrated in the Table 4 and Figure 2.15)
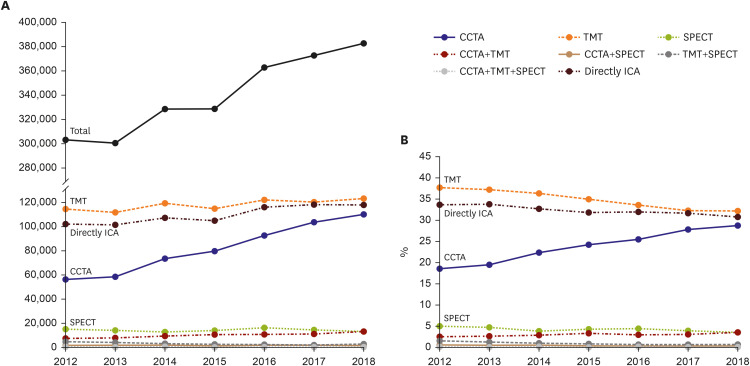
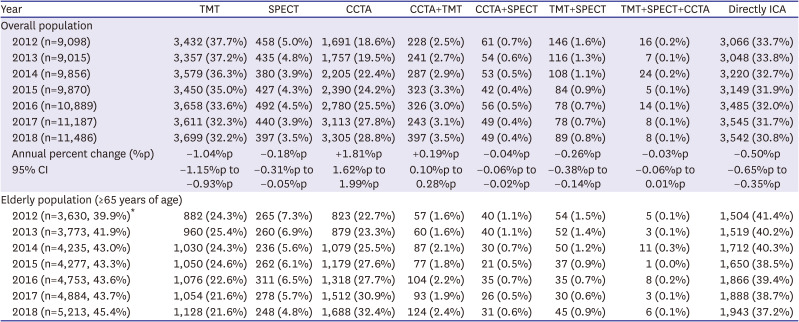
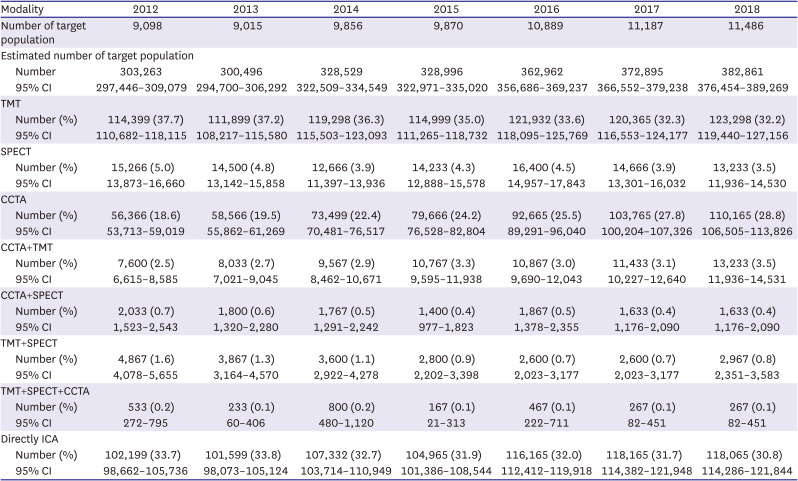
Figure 2
Annual trends of diagnostic testing among patients with suspected coronary artery disease from the HIRA-NPS between 2012 and 2018. Estimated number (A) and proportion (B) of diagnostic studies between 2012 and 2018.
CCTA = coronary computed tomography angiography; HIRA = Health Insurance Review and Assessment Service; ICA = invasive coronary angiography; NPS = National Patient Samples; SPECT = single-photon emission computed tomography; TMT = treadmill test.
![]()
Table 3
Trends of utility and type of gatekeeping modalities for patients with suspected coronary artery disease in Korea between 2012 and 2018
CCTA = coronary computed tomography angiography; ICA = invasive coronary angiography; TMT = treadmill test; SPECT = single-photon emission computed tomography.
*Annual percentage of elderly population among overall population.
![]()
Table 4
Estimated number of patients according to the utility and type of gatekeeping modalities for suspected coronary artery disease in Korea between 2012 and 2018
CI = confidence interval; CCTA = coronary computed tomography angiography; ICA = invasive coronary angiography; SPECT = single-photon emission computed tomography; TMT = treadmill test.
![]()
Downstream procedures and clinical outcome
Supplementary Table 2 summarizes the incidence of downstream ICA and revascularization according to the utility and type of gatekeeping studies. The overall incidence of downstream ICA after performing gatekeeping study was 13.8% (6,662/48,346). In addition, overall, 14.3% of patients eventually underwent coronary revascularization (13.7% for PCI [9,765/71,401] and 0.6% for CABG [462/71,401]) after ICA with or without gatekeeping study. The incidence of patients undergoing subsequent ICA differed significantly among patients who underwent TMT, SPECT, and CCTA (p<0.001). In addition, the incidence of coronary revascularization, including both PCI and CABG, differed significantly, among patients who underwent TMT, SPECT, CCTA, and directly ICA (p<0.001).
Comparison of coronary revascularization rate after ICA showed significant difference between those who performed gatekeeping study and those who did not. Patients who performed gatekeeper before ICA showed significantly higher rate of PCI (34.7% vs. 32.3%; p<0.001) and CABG (3.5% vs. 1.0%; p<0.001), compared to those who directly underwent ICA. Pairwise comparison of ICA and revascularization rate among TMT, SPECT, and CCTA as gatekeepers also differed significantly. SPECT was associated with higher rate of downstream ICA, compared to TMT and CCTA (both of p<0.001), and the rate of ICA was significantly higher in CCTA group than in TMT group (p=0.028). The coronary revascularization rate after ICA was significantly higher in patients who performed CCTA (PCI, 40.3%; CABG, 5.4%) as a gatekeeper, compared to SPECT (PCI, 37.3%; CABG, 1.8%) and TMT (PCI, 12.2%; CABG, 0.6%; p<0.016) (Tables 5 and 6).


Table 5
Comparison of coronary revascularization rate according to the utility of gatekeeper for downstream procedures
| Procedures | ICA after performing any gatekeeping studies (n=6,662) | Directly ICA without gatekeeping study (n=23,055) | p value |
|---|---|---|---|
| PCI | 2,315 (34.75%) | 7,450 (32.3%) | <0.001 |
| CABG | 235 (3.5%) | 227 (1.0%) | <0.001 |
CABG = coronary artery bypass graft; ICA = invasive coronary angiography; PCI = percutaneous coronary intervention.
![]()
Table 6
Pairwise comparison of downstream ICA and revascularization rate among TMT, SPECT, and CCTA for downstream procedures
CABG = coronary artery bypass graft; CCTA = coronary computed tomography angiography; ICA = invasive coronary angiography; PCI = percutaneous coronary intervention; SPECT = single-photon emission computed tomography; TMT = treadmill test.
*Pairwise comparison between 2 groups.
![]()
DISCUSSION
Our study demonstrated that the number of patients who underwent gatekeeping studies or ICA for suspected CAD is gradually increasing in outpatient settings using the nationwide database cohort. In particular, the proportion of CCTA as a gatekeeper for ICA was significantly increasing, in contrast to other modalities, such as TMT and SPECT, which were decreasing. The proportion of patients who directly underwent ICA without a gatekeeper was also decreasing. Overall, 13.8% of patients underwent ICA after noninvasive studies, and patients who performed SPECT showed higher rate of subsequent ICA, compared to those who performed TMT or CCTA. Coronary revascularization rate after ICA was significantly higher in patients who performed gatekeeping studies compared to those who did not, and CCTA was associated with higher revascularization rate after ICA among noninvasive studies.
Recent study by Reeves et al.16) have reported that the rate of CCTA utilization continue to increase in the United States from 2010 to 2019, but overall rates remain low compared with myocardial perfusion imaging. Several studies of emergency department also reported that the use of CCTA has increased rapidly, while rates of other cardiac stress testing modalities have decreased.17)18) The same cardiac imaging trends were observed in our database. Interestingly, the actual percentage for CCTA utilization among noninvasive cardiac studies was much higher in Korea, compared with other countries. Studies conducted in the United States and Canada reported that CCTA accounts for less than 1%, and still far more cardiac stress tests are being performed.2)16) Differences in the insurance and reimbursement policies across the countries might have influenced the utility of cardiac studies. Nonetheless, it is encouraging that the proportion of CCTA as a gatekeeper has been continuously increasing.
CCTA enables non-invasive assessment of CAD by directly imaging the coronary arteries. Many prospective studies and clinical trials have proven that CCTA is effective for both identification and exclusion of anatomic CAD, as well as for detection of high-risk plaques in patients with stable angina.19)20) Our results are in concordance with previous results revealing the highest revascularization rate after ICA in patients who underwent CCTA as a gatekeeper.21)22) Our data showed that CCTA resulted in fewer unnecessary ICAs and a higher yield of obstructive CAD at ICA leading to revascularization. Recently, the International Study of Comparative Health Effectiveness With Medical and Invasive Approaches (ISCHEMIA) trial has demonstrated that CAD severity assessed on CCTA, but not ischemia severity assessed on stress testing, predicted 4-year mortality and MI risk.23) The results provided evidence that CCTA may be superior to stress testing for risk prediction for patients with stable CAD. In addition to the degree of stenosis, comprehensive evaluation of the burden of atherosclerosis and plaque characteristics assessed on CCTA may aid selection of patients in need of revascularization.24)
Although the proportion of TMT as a gatekeeper consistently decreased, TMT was still the most widely utilized noninvasive cardiac test for patients with suspected CAD in our study. However, we observed that the prevalence of TMT was comparatively lower in the elderly population >65 years, probably due to the patients’ exercise ability and general condition. The data showed that patients who underwent TMT tended to be young and show lower CCIs. These results inversely emphasize the importance of other noninvasive studies, considering the ongoing aging of the world population. Regarding SPECT, SPECT showed higher rate of downstream ICA compared to other noninvasive cardiac tests. Clinicians might prefer SPECT in patients with highly suspected CAD. However, the high sensitivity or false positive rate of SPECT could also indiscriminately lead to downstream procedures, even for non-culprit lesions. Previous meta-analyses have suggested that SPECT is less accurate for ruling out hemodynamically significant CAD, compared to other myocardial perfusion imaging.25)26) On the other hand, there could be a high prevalence of myocardial infarction with non-obstructive coronary arteries or microvascular disease in the SPECT group, given the high burden of comorbidities and CCI in SPECT group.
Our study has several limitations. First, the data we used were separately extracted every year, thus we lacked continuous follow-up information of individual patients. In addition, medical history could be incomplete in some parts because of short follow-up period. Second, clinical data were unavailable from the database. Third, we did not deal with stress echocardiography and stress cardiac magnetic resonance imaging as an investigation modality. Finally, these results reflect the patterns of diagnoses and outcomes in Korea. Despite these limitations, this study included the national sample patients from claims data. Therefore, our findings reflect the real-world utilization of gatekeeping studies on a nationwide scale. To generalize the results, the establishment of a multi-regional database on gatekeepers for ICA can be considered.
In conclusion, this nationwide database cohort including outpatients demonstrated that patients who underwent studies for suspected CAD was increasing. The utilization of noninvasive gatekeeping studies for ICA has increased, and among them, the proportion of CCTA as a gatekeeper has shown significant increase, while those of TMT and SPECT have decreased. CCTA was associated with higher revascularization rate after ICA, among other gatekeepers.
 XML Download
XML Download