

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The burden of cardiovascular diseases (CVDs) has remained the leading cause of global deaths and disability despite the considerable effort of mitigation.1) Sustainable Development Goals from the United Nation aimed to reduce premature deaths from non-communicable diseases including CVDs by 2030, and CVD mortality rates had substantially decreased over the past decades.2) Population aging and growth, however, have offset these improvements as age is highly associated with a greater incidence and fatality of CVDs.3)4) The mortality appears to be stagnant or slightly increased in recent years.5)6)
This static global rate masked wide regional variation of CVD incidence and mortality.2)7) The CVD mortality in Africa was lower than in other regions and continued to decrease. On the contrary, the figures in Europe and America had been the most significant and increased again following the substantial reduction until the early 2010s. The burden in the Asia region was aggravated from 175.49 deaths per 100,000 population in 1990 to 237.85 per 100,000 in 2019.7) These different trends reflect changes in its underlying causes in regions such as the prevalence of CVD risk factors and access to health care along with population structure.5)8)
Geographical variations in CVD mortality have also been reported within a country9): for instance, notable differences in deaths from CVDs were observed between counties in the United States while presenting a higher burden in certain regions.10) China showed a concentrated CVD mortality in the northern part (Beijing) compared to the southern part (Shanghai and Guangzhou).9)11) Likewise, northern England and southeastern Spain showed higher death rates from CVDs than other regions in each country.12)13)
In Korea, the CVD burden is still high: heart diseases and cerebrovascular diseases had accounted for most of the deaths following cancer.14) A previous study illustrated the 36-year trend of CVD death rates. Between 1983 and 2019, CVD mortality in Korea had remarkably improved, but continuous monitoring of the trends is still needed to reduce the health burden.15) However, little research has focused on regional disparity in CVD mortality, and no study, to our knowledge, has illustrated its spatiotemporal trends. Although one study showed the cross-sectional geographic variation in CVD deaths in Korea, it was conducted using the combined data from 2011 to 2015.16)
This study aimed to investigate the trends of CVD mortality according to the different regions in Korea from 1983 to 2019.
METHODS
Ethical statement
The study protocol was approved by the Institutional Review Board (IRB) of the Yonsei University College of Medicine (4-2020-0207). Informed consent was waived by the IRB.
Data sources and variables
We used deidentified data on mortality from the Korean Statistical Information Service and Microdata Integrated Service provided by Statistics Korea. The annual mortality by cause was obtained along with information on sex, age, and address of the deceased.14)
The underlying cause of death described in the death certificate was supplemented and used as the cause of death in the death statistics.14) They were coded and classified into 22 chapters and 267 blocks by the Korean Standard Classification of Diseases and Causes of Death (KCD-7).14)17) It was developed based on the International Statistical Classification of Diseases, 10th revision.17) This study analyzed a selected category, all diseases of the circulatory system (I00–I99), along with the following 6 subcategories which were not mutually exclusive: total heart disease which excluded cerebrovascular diseases from all circulatory diseases (I00–I13 and I20–I51), hypertensive heart disease (I10–I13), ischemic heart disease (IHD, I20–I25), myocardial infarction (MI, I21–I23), heart failure (HF, I50), and cerebrovascular disease including non-traumatic hemorrhagic stroke, infarction, and cerebral artery diseases (I60–I69). The codes of particulars in each category are presented in the Supplementary Figure 1.
South Korea comprises 17 first-tier administrative divisions. It includes 8 metropolitan cities (Seoul, Busan, Daegu, Incheon, Gwangju, Daejeon, Ulsan, and Sejong) and 9 provinces (Gyeonggi, Gangwon, Chungbuk, Chungnam, Jeonbuk, Jeonnam, Gyeongbuk, Gyeongnam, and Jeju). Sejong city was deliberately designated as a special self-governing city in 2012 to ease congestion in Seoul, the current capital, rather than its population size or urbanicity. For the analytical reason, we merged Sejong city with Chungnam province as previously classified.18)19) We categorized deaths into 17 regions based on the resident registration address of the deceased.14)
Statistical analysis
The sex and age-standardized mortality rates were calculated using the direct standardization method. The 2019 Korean population structure was used as the standard population. We analyzed the region-specific CVD mortality rates of 17 divisions from 1983 to 2019. For an intuitive comparison of geographic disparity in CVD deaths, we calculated standardized mortality ratio (SMR) in each region using indirect adjustment. The ratio of the total number of deaths in other regions to the total deaths in Seoul was compared by year.
RESULTS
Mortality from all diseases of the circulatory system
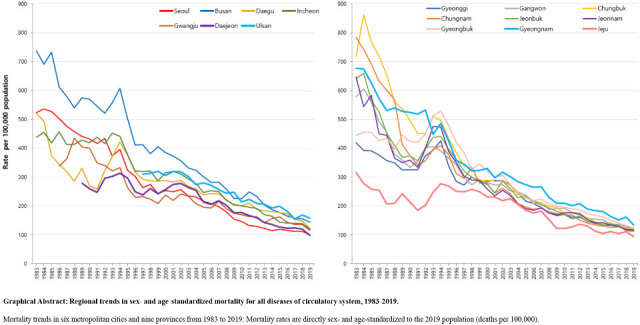
Mortality from all diseases of the circulatory system showed a substantial decline in all regions in Korea (Figure 1A). The spike in the mid-1990s was observed nationwide, although there is a difference in its degree. At the beginning of the study period, the death rates were high in Busan, Chungbuk, and Chungnam, while Gyeonggi and Jeju showed low figures. The mortality rates in regions, however, gradually converged over time. The narrowing discrepancy was also observed in the comparison of SMRs. Figure 1B shows that Incheon, Gyeonggi, and Gyeongbuk, which had lower mortality rates than Seoul in 1983, increased over time and surpassed it. Southeastern regions such as Busan, Ulsan, and Gyeongnam regions had shown higher CVD deaths than other regions since 1983, while Jeju had been the lowest.
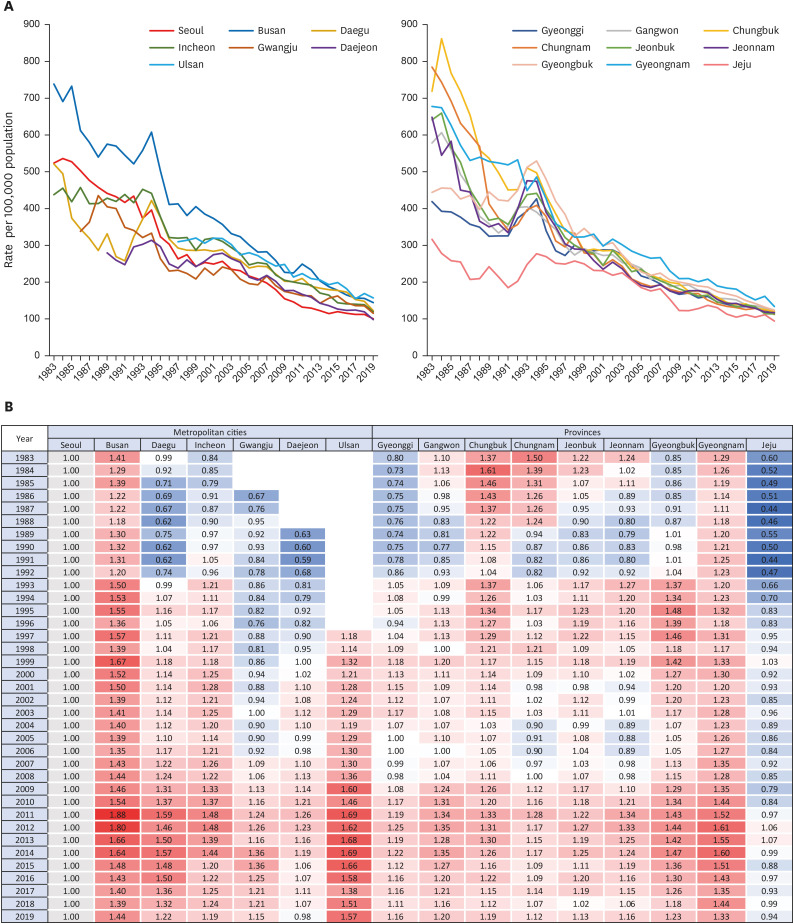
Figure 1
Regional trends in sex- and age-standardized mortality for all diseases of circulatory system, 1983–2019. (A) Mortality trends in 6 metropolitan cities and 9 provinces from 1983 to 2019: mortality rates are directly sex- and age-standardized to the 2019 population (deaths per 100,000). (B) The ratio of mortality rates in other regions to Seoul (reference, light grey): blue indicates a lower rate than Seoul and red indicates a higher rate.
![]()
Mortality from total heart diseases and hypertensive heart diseases
Except for Busan, all regions showed a sharp decrease in mortality from total heart diseases until the late 1990s, and those remained stable (Figure 2A). In Busan, the spike in the mid-1990s was more prominent, and the decline occurred slowly. Even when sex and age-standardized mortality in other regions was stabilized after the late 1990s presenting 100 deaths per 100,000, Busan had almost 200. Likewise, the mortality from hypertensive heart diseases was stabilized following the decrease until the late 1990s (Figure 3A). At the beginning of the study period, Chungbuk, Chungnam, and Jeonnam showed relatively high values in mortality rates due to total heart diseases and hypertensive heart diseases in Figures 2B and 3B, but gradually decreased and became stable in the late 1990s. Meanwhile, Busan, Ulsan, and Gyeongnam had shown higher mortality rates than others throughout the study period.
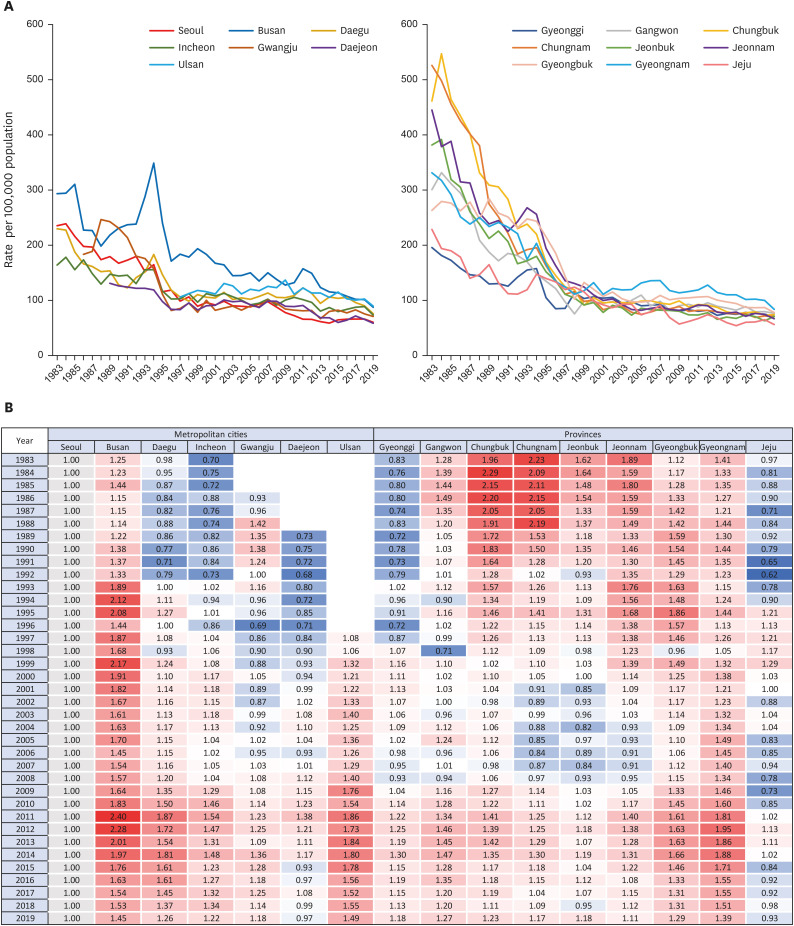
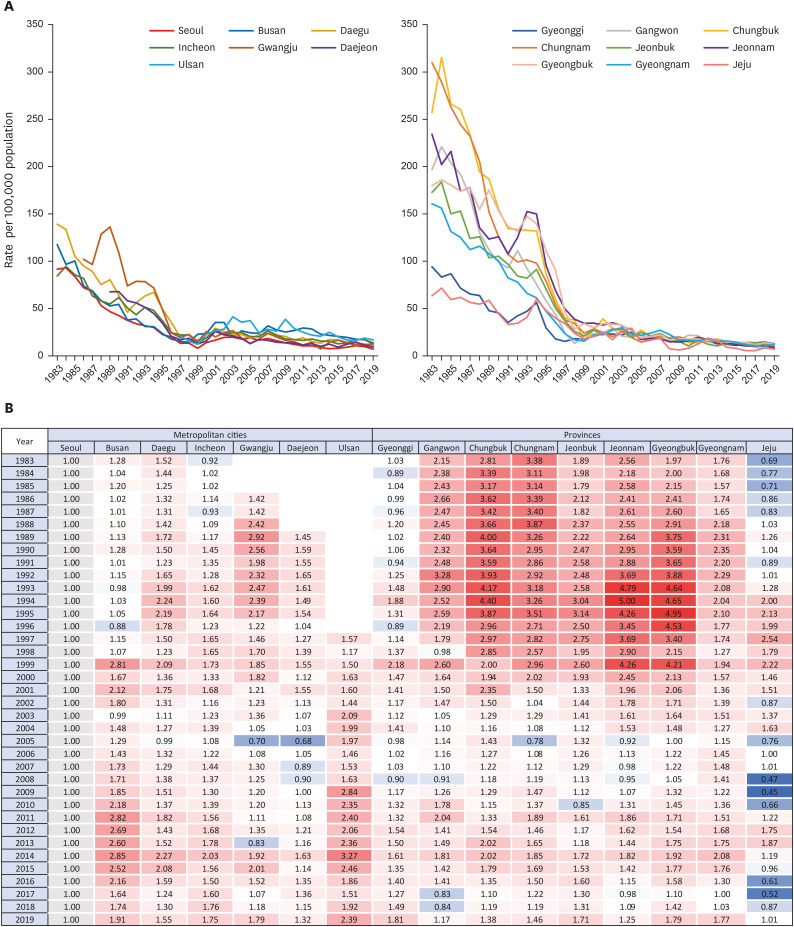
Figure 2
Regional trends in sex- and age-standardized mortality for total heart diseases, 1983–2019. (A) Mortality trends in 6 metropolitan cities and 9 provinces from 1983 to 2019: mortality rates are directly sex- and age-standardized to the 2019 population (deaths per 100,000). (B) The ratio of mortality rates in other regions to Seoul (reference, light grey): blue indicates a lower rate than Seoul and red indicates a higher rate.
![]()
Figure 3
Regional trends in sex- and age-standardized mortality for hypertensive heart diseases, 1983–2019. (A) Mortality trends in 6 metropolitan cities and 9 provinces from 1983 to 2019: mortality rates are directly sex- and age-standardized to the 2019 population (deaths per 100,000). (B) The ratio of mortality rates in other regions to Seoul (reference, light grey): blue indicates a lower rate than Seoul and red indicates a higher rate.
![]()
Mortality from myocardial infarction and ischemic heart diseases
The sex and age-standardized death rate from MI rose across all regions until the mid-2000s and then declined to show an inverted ‘U’ shape in Figure 4A. In the mid-2000s, the peak of the figure in other regions was below 60 deaths per 100,000 people, but it in Busan exceeded 80 and was prolonged. Also, it is notable that Daegu was one of the lowest mortality due to MI in 1983, but it was ranked first among 17 regions in 2019. A large portion of deaths from IHD is attributable to MI. Deaths due to IHD showed a similar trend to MI where the rates decreased after its peak in the mid-2000s (Supplementary Figure 2). Compared to Seoul, the death rates from MI and IHD were lower in all regions except Busan until the early 1980s (Figure 4B, Supplementary Figure 2). The recent mortality was, however, lower only in Daejeon and Jeju, compared to Seoul. The MI death rate in Busan had been the highest from 1995 to 2015, although the discrepancy was narrowing in recent years.
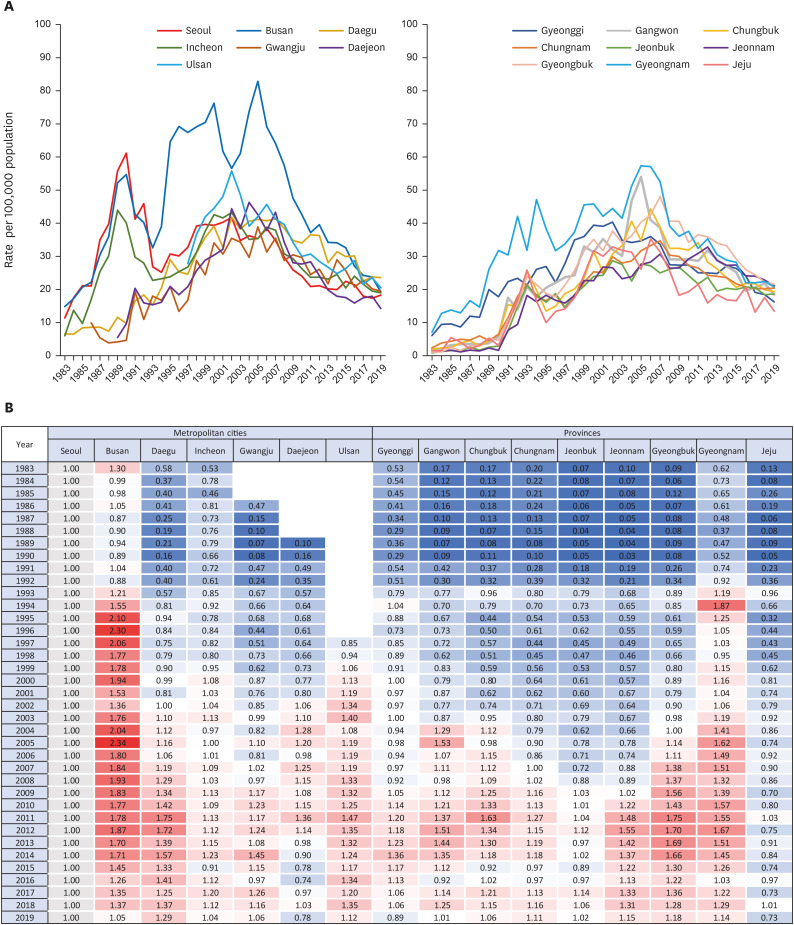
Figure 4
Regional trends in sex- and age-standardized mortality for myocardial infarction, 1983–2019. (A) Mortality trends in 6 metropolitan cities and 9 provinces from 1983 to 2019: mortality rates are directly sex- and age-standardized to the 2019 population (deaths per 100,000). (B) The ratio of mortality rates in other regions to Seoul (reference, light grey): blue indicates a lower rate than Seoul and red indicates a higher rate.
![]()
Mortality from heart failure
Figure 5A illustrates an overall upward trend across all regions regarding HF mortality. The figures in Busan, Gyeongnam, and Chungbuk were more prominent than in other regions. The spike in the mid-1990s was observed across all regions, but it in Busan was more substantial and lasted longer than in others. This greater rise in deaths in Busan was estimated as a SMR, of 5.69 in 1995 (Figure 5B). Also, the ratio in Busan peaked at 10.98 in 2001 when the mortality rates in other regions were low. Another upsurge in 2011 was observed in Busan and Ulsan. Other regions with a mortality ratio of less than 1 at the beginning of the study showed higher values than Seoul in recent years. Particularly Gangwon, Chungbuk, and Gyeongbuk recorded the highest in 2019.

Figure 5
Regional trends in sex- and age-standardized mortality for heart failure, 1983–2019. (A) Mortality trends in 6 metropolitan cities and 9 provinces from 1983 to 2019: mortality rates are directly sex- and age-standardized to the 2019 population (deaths per 100,000). (B) The ratio of mortality rates in other regions to Seoul (reference, light grey): blue indicates a lower rate than Seoul and red indicates a higher rate.
![]()
Mortality from cerebrovascular diseases
Deaths from cerebrovascular disease in some regions continued to decline, whereas others rose until the mid-1990s (Figure 6). Since then, there had been a downward trend in all regions. Nevertheless, Busan and Ulsan regions still had the highest mortality rate in recent years than any other region. The disparity between this southeastern part and other regions was not prominent in cerebrovascular disease-related deaths as much as it in other CVD deaths. Meanwhile, Jeju remained the lowest mortality from cerebrovascular diseases, although it increased and the discrepancy with Seoul became less apparent.

Figure 6
Regional trends in sex- and age-standardized mortality for cerebrovascular diseases, 1983–2019. (A) Mortality trends in 6 metropolitan cities and 9 provinces from 1983 to 2019: mortality rates are directly sex- and age-standardized to the 2019 population (deaths per 100,000). (B) The ratio of mortality rates in other regions to Seoul (reference, light grey): blue indicates a lower rate than Seoul and red indicates a higher rate.
![]()
DISCUSSION
The overall trend of mortality from each CVD was similar across all regions. Mortality of HF increased across all regions; other CVD death rates showed a decreasing trend nationwide. Regional disparity in mortality was substantial in the early 1980s but converged over time. In all types of cardiovascular mortality, Busan, Ulsan and Gyeongnam remained at the top of the 17 regions, although they showed a downward trend like others. On the other hand, Jeju continued to have a relatively low CVD mortality rate while gradually closing the gap with other regions. Mortality in Seoul and other regions fluctuated and steadily converged. In most CVD-related deaths, other regions showed lower or similar rates than Seoul at the beginning of the observation but surpassed Seoul over time. Mortality from hypertensive heart diseases in other regions was much higher than in Seoul and Jeju at first. Despite the narrowing gap, rates in other regions remained higher. Both trends resulted in relatively lower burdens of deaths from the circulatory system in Seoul and Jeju in recent data.
There is little research on geographic variation in cardiovascular health or death in Korea. They have focused on the associations between CVD-related outcomes and regional characteristics such as urbanization and community economic status, rather than the region itself.20) Ro and colleagues21) analyzed the survival rate and the distribution of risk factors of out-of-hospital cardiac arrest according to urbanization. The rates for return of spontaneous circulation and survival were higher in metropolitan, urban, and rural areas in that order, whereas the age- and sex-adjusted incidence rates were higher in rural areas. The risk factors aggravating the survival rate were also greater in rural areas: no bystander cardiopulmonary resuscitation, longer medians of the response interval, and transportation to a lower-level emergency department.21) Another study also identified rural disadvantages in the treatment and fatality rate of acute MI. Compared to Seoul, the odds ratio of receiving higher-quality medical management and invasive procedures in patients hospitalized with acute MI was estimated lower in other cities and rural areas in that order.22)
The socioeconomic level of a community appears to have an impact on cardiovascular health-related mortality.23)24) One study found that regions with a large number of basic livelihood recipients per 100,000 persons had a significant positive association with the standardized mortality from hypertensive disease.25) Furthermore, populations in districts with a higher supply of health care resources, for instance, hospital beds, computed tomography scanners, and magnetic resonance imaging units, and greater utilization of local healthcare services had higher hospital admissions for CVD.16) Given the different patterns in a correlation between CVD morbidity and mortality by 245 local districts, it implies that health care resources and utilization may affect the regional disparity in leading CVD morbidity to mortality.
While considering these implications of urbanization and community economic level for cardiovascular health, it is crucial to investigate the disparity in mortality by the administrative district as a target unit for national policymaking and intervention development. This analysis reveals varying degrees of CVD burden by region that were not observed when deaths in all regions were taken together. In particular, Busan, Ulsan, and Gyeongnam showed high mortality rates for all types of CVDs. This is consistent with a study showing regionally biased CVD mortality in certain regions of the United States: deaths from CVDs, IHD, hypertensive heart diseases, and cerebrovascular diseases were concentrated in Southeastern Oklahoma and Eastern Kentucky.10) A range of possible causes was suggested including environmental exposures related to coal and metal mining, housing density, and access to health care.10) Also, one study linked data from the surveillance system of behavioral risk factors and state-level coronary heart disease and stroke mortality data. They found significant state-level variation in the prevalence of poor cardiovascular health. It was partly attributable to median household income, taxes on soda drinks and cigarettes, and food and physical activity environments in a region.26)
However, there is a considerable knowledge gap to fully explain the higher rates in Busan, Ulsan, and Gyeongnam or the relatively lower rate in Seoul and Jeju. Most regions in Korea are a combination of urban and rural areas and cannot be simply defined by community economic level. Each province has unique region-specific characteristics such as environment, lifestyle, and medical resources.27) A Korean study suggested that regional disparity of CVD mortality results from the differences in the determinants such as regional socioeconomic level, physical environment, and health-related resources.27) These factors may affect the CVD incidence and lead to a concentrated burden in Busan, Ulsan, and Gyeongnam. Previous studies reported that Busan had a high age-standardized incidence rate of acute MI.28) CVD incidence, however, is not necessarily related to higher mortality. For instance, the incidence rate in Jeju was greater than in Busan, but the mortality rate was reversed showing a lower figure in Jeju.28) This inconsistency may result from regional differences in risk-modifying factors linking incidence to mortality. In addition, misclassification when reporting the CVD diagnosis or the cause of death should be taken into consideration. With a thorough examination of the surveillance system especially in southeastern regions, further study can help us understand mortality disparity by regions in Korea. It needs to elucidate (1) exposure to metabolic, behavioral, and environmental risks, (2) delivery of interventions to modify CVD risk factors, and (3) access or utilization of high-quality medical care to improve outcomes when a CVD event occurs.10)
Also, our study found that Busan showed multiple extreme surges in mortality. Except deaths from hypertensive heart disease and cerebrovascular disease, CVD-related mortality in Busan sharply increased and then decreased, particularly spikes in HF were noteworthy. A possible explanation for the surges is the misclassification of the cause of death. As mentioned, the mortality was higher than the incidence in Busan, and the death rates were extreme in the mid-1990s and the mid-2000s.28) Given that, it is highly likely that there was misclassification in the diagnosis or coding system. To clarify the cause of the higher CVD burden in Busan, Ulsan, and Gyeongnam, the surveillance system on CVD should be strengthened at the local government and national levels in addition to the academic effort to determine risk factors in these regions.
Our study is the first study, to our knowledge, to examine long-term changes in the geographical variation of CVD mortality for the long period, of 36 years. The scope of previous studies investigating regional disparity was focused on regional characteristics or had a shorter period. Several limitations should also be considered. First, temporal analysis of mortality statistics based on death certificates is vulnerable to misclassification or diagnosis accuracy. During the study period, the KCD was revised 5 times.17) Major revision in the coding system may have affected the mortality rate for each disease. Furthermore, since the cause of CVD death is mostly recorded by doctors, it may affect overreport or underreport according to doctors’ coding patterns, especially in rural regions where the number of hospitals is limited.29) For instance, a study compared the causes of death in medical records with those in death certificates issued by a university hospital in 2003, and an accuracy of 61% was reported.30) However, since the issued death certificate was supplemented and corrected by a standardized method, the accuracy rate of the cause of death in the published death statistics increased to 92%.30) With the development and diagnostic tools over time, diseases that were previously difficult to be detected are properly classified, which may have affected the trends. Second, the limitation of analysis based on administrative divisions should be taken into account. It is not necessarily classified on the basis of population size or urbanization. For instance, Sejong city was designated as a metropolitan city in 2012 to ease the congestion of the capital. Also, null data were observed before 1986 for Gwangju, 1989 for Daejeon, and 1997 for Ulsan when they were subordinate to Jeonnam, Chungnam, and Gyeongnam, correspondingly.
In conclusion, a decline in cardiovascular mortality was experienced across all regions in Korea for 36 years. The regional disparity had substantially decreased compared to the 1980s. However, the relatively high burden of Busan, Ulsan, and Gyeongnam has not been resolved. To reduce premature CVD deaths, these regions call for action in terms of prevention and management of CVD, while facilitating the reduction of death rates in other regions.
 XML Download
XML Download