

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cryptogenic stroke refers to the development of cerebral embolism that is not attributed to large artery atherosclerosis, small vessel disease (lacunar infarcts), cardioembolism, or other determined cause.1) Cryptogenic strokes are thought to comprise approximately 25% of all ischemic strokes. Most cryptogenic strokes are thought to be an embolic stroke of unspecified source (ESUS), some of which are caused by right to left shunt, and patent foramen ovale (PFO) is thought to be an important cause.2)
PFO is a remnant of the fetal circulation characterized by a slit-like structure between the superior limb of the septum secundum on the right atrium side and the septum primum on the left atrium side. There is communication between the right and left atrium, particularly clinical situation that cause a sudden rise and fall in intrathoracic pressure, such as sneezing, coughing or straining. Cohnheim et al.3) first reported on a potential causal relationship of a PFO and stroke in 1877. They postulated that a blood clot from the peripheral veins had migrated from the venous system into the systemic circulation through the PFO and blocked the cerebral artery. PFO was found a prevalence of 27.3% in an autopsy study of 965 normal hearts.4) Although PFO is incidentally detected for the majority of people, some PFOs provide a conduit for material such as thrombi. In this situation, percutaneous PFO closure provides a practical solution in carefully selected patients.
Therefore, it is very important to understand the characteristics of ischemic stroke caused by the PFO and selectively treat the PFO directly related to the occurrence of ischemic stroke. In this paper, we focused on the evidence for PFO closure, discuss which patients should be considered for percutaneous PFO closure.
CHARACTERISITICS OF PFO-ASSOCIATED STROKE
Recently, the term of cryptogenic stroke in the presence of PFO has changed into PFO-associated stroke.5) Stroke is the most common manifestation of paradoxical embolism. The process of blood clots entering arterial circulation through right-to-left shunt is essential to cause paradoxical embolism. Therefore, small sized cerebral cortical infarction lesions are observed in PFO-associated stroke, mainly because small blood clots are embolized into the brain through the PFO. In addition, Valsalva maneuver not only transiently increases the blood flow through the right-to-left shunt, but also relatively increases the blood flow to the posterior circulation system. Therefore, it is known that PFO-associate stroke during the Valsalva maneuver frequently occurs in the posterior circulation.6)
In general, stroke patients caused by atherosclerosis occur in elderly patients, who have risk factors such as high blood pressure, diabetes mellitus, dyslipidemia, smoking history and prior transient ischemic attack (TIA) or stroke history. In contrast, patients with PFO-associated stroke do not have many of these risk factors because they are not caused by atherosclerosis.
PATIENT SELECTION
Because of the high prevalence of PFO (around 25%),7) physicians often have to decide whether PFO had a causal role for stroke, and whether PFO closure can reduce the recurrent event. However, optimal patient selection for percutaneous PFO closure has not been clarified.
Two scoring system have been proposed to assess the possibility of the PFO-associated strokes to date. A 10-point scale of a risk of paradoxical embolism (RoPE) score has been developed using the patient age, absence of vascular risk factors and brain imaging findings, and the possibility of cerebral infarction caused by an PFO could be estimated.8) Those with a RoPE score greater than 6 are considered high risk with a PFO attributable fraction between 62–88% and Kaplan-Meier estimated stroke/TIA 2-year recurrence rates decreased from 20% (95% confidential interval [CI], 12–28%) in the lowest RoPE score stratum to 2% (95% CI, 0–4%) in the highest (Table 1). More recently, PFO-Associated Stroke Causal Likelihood (PASCAL) classification system also suggested. PASCAL scores combined the RoPE score with the presence or absence of high risk PFO features including large shunt and atrial septal aneurysm, to determine the likelihood that the PFO-associated stroke (Figure 1).
Table 1
PFO-attributable fraction and estimated 2-year risk of stroke/TIA by RoPE score8)
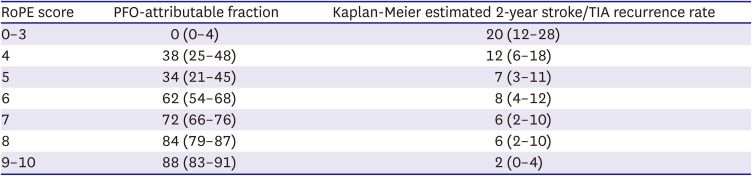
Figure 1
RoPE and PASCAL scoring system.9)
ASA = atrial septal aneurysm; LS = large shunt; PASCAL = Patent Foramen Ovale-Associated Stroke Causal Likelihood; PFO = patent foramen ovale; RoPE = risk of paradoxical embolism; TIA = transient ischemic attack.
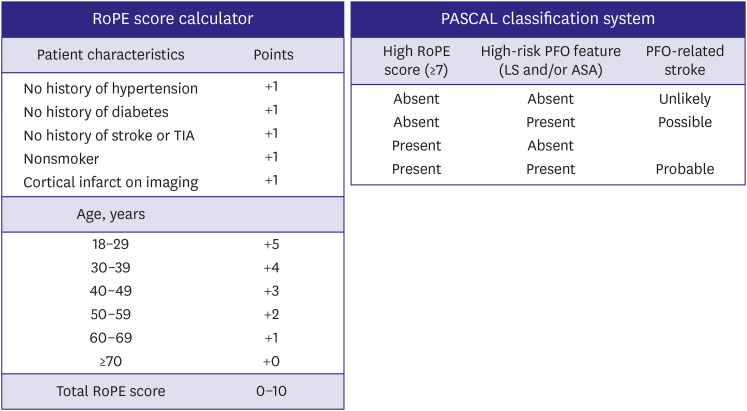
In the PASCAL scoring system, large shunt size was defined in the database as ≥20 bubbles in the left atrium on transesophageal echocardiography and atrial septal aneurysm was defined as ≥10 mm of excursion from midline.9) Among 1,383 patients for whom the PASCAL algorithm classified the PFO as having had a probable causal role in the stroke, there was a significant 90% relative reduction in the recurrent stroke over a median follow-up of 57 months. On the other hands, among 547 patients with stroke unrelated to the PFO, PFO closure was not associated with risk reduction of recurrent stroke but was associated with the higher rates of device-related atrial fibrillation. Patients classified as unlikely, possible, and probable using the PASCAL classification system had hazard ratios (HRs) 1.14 (95% CI, 0.53–2.46), 0.38 (95% CI, 0.22–0.65), and 0.10 (95% CI, 0.03–0.35), respectively. The 2-year absolute risk reduction was −0.7% (95% CI, −4.0–2.6%), 2.1% (95% CI, 0.6–3.6%), and 2.1% (95% CI, 0.9–3.4%) in the unlikely, possible, and probable PASCAL categories, respectively. Based on these results, physicians can apply the PASCAL scoring system to distinguish the patients whose PFO closure may be helpful from those who are unlikely among the patients aged 18 to 60 years.
Elderly patients over 60 years excluded from most of the randomized trials. However, previous study has shown that there is a relationship between older age and risk of recurrent stroke in patients with PFO. Recently, a multicenter study was published to evaluate the early- and long-term outcomes of percutaneous PFO closure in elderly (>60 years) patients with PFO-associated strokes.10) The study included the 388 and 883 patients with PFO closure at age over 60 (mean 67 years) and no more than 60 (mean 44 years), respectively. Patients over the age of 60 not only had a high burden on cardiovascular risk factors but also had a high incidence of large shunt and atrial septal aneurysm. PFO closure was safely performed in elderly patients, and the incidence of thromboembolism was relatively low during follow-up. However, compared to younger patients, the risk of stroke recurrence was higher in elderly patients.
As the patients get older, the incidence of atrial fibrillation increases rapidly. Therefore, extended rhythm monitoring through implantable loop recorders is important in elderly patients before considering PFO closure in patients who have experienced strokes over the age of 65. Nevertheless, the beneficial effect of PFO closure has been identified in selected patients through several observation studies to date. The clinical evidence of the potential benefit of PFO closure has limited in elderly patients and needs to be investigated with further clinical studies.
EVIDENCE FOR PERCUTANEOUS PFO CLOSURE
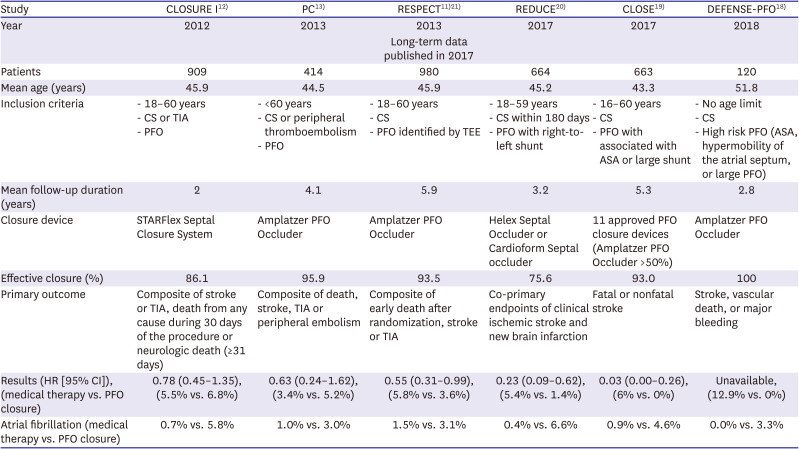
Six randomized clinical trials comparing the recurrent rate of ischemic stroke after percutaneous PFO closure compared to the medical treatment in patients with cryptogenic stroke have been published to date (Table 2). Initial 3 studies (CLOSURE I, PC, RESPECT) in 2012 and 2013 failed to show a benefit of PFO closure with an excess of complications in the interventional arm.11)12)13) The causes of these failure are as follow: inadequate patient selection (large number of patients with TIAs), a high rate of procedural failure, limited follow-up period and inadequate study design.14)
Table 2
Results of randomized clinical trials of PFO closure
| Study | CLOSURE I12) | PC13) | RESPECT11)21) | REDUCE20) | CLOSE19) | DEFENSE-PFO18) |
|---|---|---|---|---|---|---|
| Year | 2012 | 2013 | 2013 | 2017 | 2017 | 2018 |
| Long-term data published in 2017 | ||||||
| Patients | 909 | 414 | 980 | 664 | 663 | 120 |
| Mean age (years) | 45.9 | 44.5 | 45.9 | 45.2 | 43.3 | 51.8 |
| Inclusion criteria | - 18–60 years | - <60 years | - 18–60 years | - 18–59 years | - 16–60 years | - No age limit |
| - CS or TIA | - CS or peripheral thromboembolism | - CS | - CS within 180 days | - CS | - CS | |
| - PFO | - PFO | - PFO identified by TEE | - PFO with right-to-left shunt | - PFO with associated with ASA or large shunt | - High risk PFO (ASA, hypermobility of the atrial septum, or large PFO) | |
| Mean follow-up duration (years) | 2 | 4.1 | 5.9 | 3.2 | 5.3 | 2.8 |
| Closure device | STARFlex Septal Closure System | Amplatzer PFO Occluder | Amplatzer PFO Occluder | Helex Septal Occluder or Cardioform Septal occluder | 11 approved PFO closure devices (Amplatzer PFO Occluder >50%) | Amplatzer PFO Occluder |
| Effective closure (%) | 86.1 | 95.9 | 93.5 | 75.6 | 93.0 | 100 |
| Primary outcome | Composite of stroke or TIA, death from any cause during 30 days of the procedure or neurologic death (≥31 days) | Composite of death, stroke, TIA or peripheral embolism | Composite of early death after randomization, stroke or TIA | Co-primary endpoints of clinical ischemic stroke and new brain infarction | Fatal or nonfatal stroke | Stroke, vascular death, or major bleeding |
| Results (HR [95% CI]), (medical therapy vs. PFO closure) | 0.78 (0.45–1.35), (5.5% vs. 6.8%) | 0.63 (0.24–1.62), (3.4% vs. 5.2%) | 0.55 (0.31–0.99), (5.8% vs. 3.6%) | 0.23 (0.09–0.62), (5.4% vs. 1.4%) | 0.03 (0.00–0.26), (6% vs. 0%) | Unavailable, (12.9% vs. 0%) |
| Atrial fibrillation (medical therapy vs. PFO closure) | 0.7% vs. 5.8% | 1.0% vs. 3.0% | 1.5% vs. 3.1% | 0.4% vs. 6.6% | 0.9% vs. 4.6% | 0.0% vs. 3.3% |
However, as treated analyses in the pooled analysis of individual participant data from previous 3 randomized trials produced that percutaneous PFO closure showed the significant reduction of recurrent strokes than medical therapy.15) Furthermore, meta-analysis of randomized trials have reported that percutaneous PFO closure may be beneficial in reducing the risk of recurrent events when compared to medical treatment in patients with cryptogenic stroke, especially with Amplatzer device.16)17) Based on these results, 3 additional studies (REDUCE, CLOSE and DEFENSE-PFO) were conducted and published along with the results of long-term follow-up data of RESPECT trial. In the 3 new trials, they included the patients with index strokes more likely secondary to paradoxical embolism or higher-risk PFOs. REDUCE, CLOSE and DEFENSE-PFO trials showed a significant reduction in recurrent stroke in the PFO closure group.18)19)20) In addition, RESPECT with longer-term results (median follow-up duration of 5.9 years) also showed the increasing benefit over time in the patients treated with percutaneous PFO closure.21) The most recently published DEFENSE-PFO study was conducted in South Korea, and followed up for 2.8 years in 120 patients with cryptogenic stroke and high-risk PFO (PFO with atrial septal aneurysm, hypermobility, PFO size ≥2 mm). No stroke occurred in the closure group at all, but in 12.9% of the medical treatment group. During the follow-up period, magnetic resonance imaging was performed after 6 months, and a symptomatic ischemic stroke was more observed in the medical therapy group, but was not statistically significant (closure vs. medical therapy; 8.8% vs. 18.4%, p=0.24).18)
FUTURE PERSPECTIVES
Through the discrepancy of early and later studies results, we learned a group of patients with a high risk of recurrence of paradoxical embolism. By excluding other identified causes of stroke, we can reduce the recurrence of ischemic stroke through procedures in patients with PFO. Strict selection of patients for PFO closure can ensure that percutaneous PFO closure in guidelines can be changed to what is recommended as first-line therapy.
There is a lack of data comparing the effects of PFO closure or antiplatelet agents and oral anticoagulants to prevent recurrent stroke. The CLOSE trial was the only one in which patients were randomized to PFO closure, oral anticoagulation or antiplatelet therapy. However, the study was underpowered as many patients had contraindications to oral anticoagulation. The CLOSE trial showed a nonsignificant 56% risk reduction in the recurrent stroke in patients treated to oral anticoagulants compared with patients with antiplatelet therapy. Unfortunately, none of the recently published NAVIGATE-ESUS trial comparing aspirin 100 mg and rivaroxaban 15 mg, and RE-SPECT ESUS trial comparing 110 mg or 150 mg of dabigatran in patients with ESUS demonstrated the superiority of oral anticoagulants in preventing recurrent stroke against aspirin. Major bleeding increased in Rivaroxaban group, but dabigatran had no significant difference from aspirin.22)23) In the future, a well-designed study comparing PFO and oral anticoagulation through randomized trial is needed.
Additional studies will be needed on longer than 10 years of long-term clinical data related to the occurrence of AF and recurrence of stroke, and the optimal regimen and duration of antiplatelet agents after PFO closure. Optimal patient selection for PFO closure may require further research on the ethnic difference in thrombogenicity and response to oral antithrombotic therapy.24)25) In the distant future, we will also have to discuss PFO closure for primary prevention in some selected patients.
CONCLUSIONS
Percutaneous PFO closure in patients between the ages of 18 and 60 with a prior PFO-associated stroke reduced the stroke recurrence compared to the antiplatelet therapy alone. Considering that PFO closure cannot completely prevent stroke recurrence and that complications including atrial fibrillation, we should be selectively performed in patients with high-risk PFO.
 XML Download
XML Download