

 PDF
PDF Citation
Citation Print
Print



A 38-year-old woman of unremarkable past health presented with dyspnea, chest pain and fever 5 days after her first BNT162b2 coronavirus disease 2019 (COVID-19) vaccine. Transthoracic echocardiogram showed mild concentric left ventricular wall thickening and trace pericardial effusion. Cardiovascular magnetic resonance (CMR) demonstrated on 4-chamber view diffuse myocardial edema (Figure 1A) and non-ischemic late gadolinium enhancement (LGE) (Figure 1B). Troponin level rose to 8,995 ng/L (normal <15 ng/L). Coronary angiogram was normal. Endomyocardial biopsy confirmed lymphocytic myocarditis (Figure 1C). Extensive autoimmune and microbiological investigation including human immunodeficiency virus, coxsackie virus and parvovirus titer was unrevealing. Shortly after she developed biventricular failure, cardiogenic shock and acute renal failure. A decision was made to initiate biventricular Impella support with Impella RP in the right and Impella CP in the left ventricles respectively (Figure 1D), with marked hemodynamic improvement. She also received empirical intravenous immunoglobulin and continuous renal replacement therapy. She weaned from mechanical circulatory support and was discharged a month later with complete renal recovery. A repeat CMR at 6 months showed resolution of edema with normal T2 mapping (Figure 1E). Subepicardial LGE was evident on basal and mid-ventricular lateral walls (Figure 1F). Native T1, T2 and extracellular volume (ECV) values were normal. Transthoracic echocardiogram showed normal global longitudinal strain (Figure 1G).
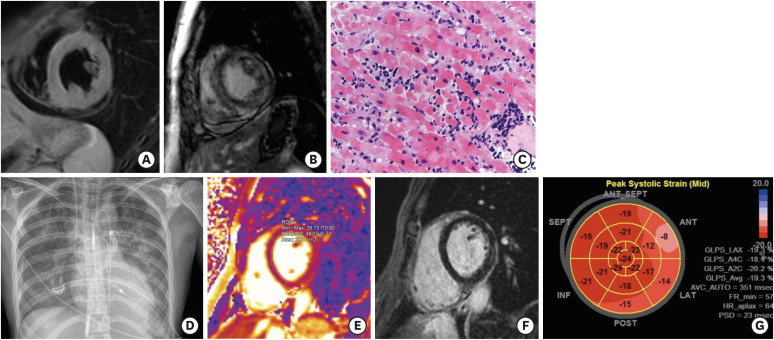 | Figure 1(A) Diffuse myocardial edema on T2-weighted CMR. (B) Diffuse non-ischemic pattern of late gadolinium enhancement on CMR. (C) Endomyocardial biopsy showed lymphocytic myocarditis. (D) Impella support with Impella RP in the right and Impella CP in the left ventricles respectively. (E) CMR at 6 months showed resolution of edema on T2 mapping. (F) Subepicardial LGE was evident on basal and mid-ventricular lateral walls. (G) Transthoracic echocardiogram at 6months showed normal left ventricular global longitudinal strain.CMR = cardiac magnetic resonance; LGE = late gadolinium enhancement.
|
Fulminant myocarditis after first dose of mRNA COVID-19 vaccine in adult female is very rare. This case shows persistent LGE 6 months after initial insult. Contrary to previous reports,1)2) a higher incidence of COVID-19 mRNA vaccine related myocarditis is reported in a largely ethnic Chinese adolescent population.3) Long term prognosis of these patients remains to be ascertained.
Patient’s informed consent was waived by the Research Ethics Committee of Kowloon East Cluster, Hospital Authority.
 XML Download
XML Download