

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
High blood pressure (BP) is associated with increased cardio-, cerebro-, and renovascular complications.1) Its prevalence is increasing worldwide, and more than 50% of adults aged >60 years have hypertension in Korea.2) There is a large body of evidence that lowering BP reduces vascular events,3) and recently, even lower BP targets have been proposed.4)5) However, more than half of hypertensive patients do not achieve the required target BP.6) Although drug adherence is most crucial to achieve blood pressure control, only less than half of all hypertensive patients are considered adherent.7) Therefore, increasing drug adherence may alleviate the BP control rate.
Self-monitoring of blood pressure (SMBP) is known to reduce BP, although the exact mechanisms have not been elucidated.8) Possible explanations include increased awareness leading to better drug adherence and life-style modification by the patients themselves.8) Therefore, SMBP is recommended by the hypertension practice guidelines.9)
Although SMBP can reliably measure daily BP, the patient may not know the adequate response to the measured blood pressure value obtained. Tucker et al.10) showed in a systematic review and an individual patient data meta-analysis that SMBP alone could not achieve clinically significant BP control, unless it was accompanied by adequate co-interventions such as drug adjustment by the health care providers.
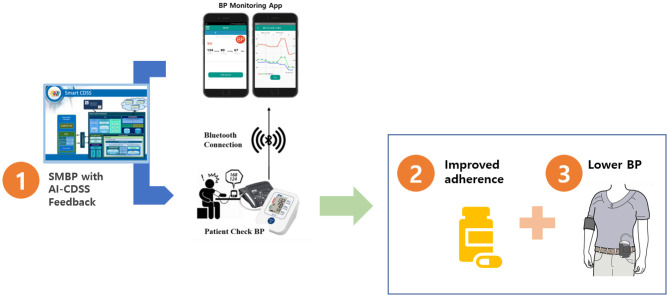
Although the direct intervention by health care professionals is the most effective means, it is also the most expensive one. Mobile health is a flexible platform with a low cost and an easy distribution. We developed a mobile health platform to provide tailored recommendations for hypertensive patients; the app gives an alert for BP measurement, records BP, and gives specific recommendations in response to the obtained value. In this prospective, randomized, open-label study, we will evaluate whether the mobile health app can help to reduce BP, to reach the BP target, and to increase the drug adherence compared to SMBP alone in hypertensive patients.
METHODS
Ethical statement
This clinical trial was approved by the institutional review board or ethics committee at each of the 5 participating hospitals; they are Seoul National University Bundang Hospital, Kyung Hee University Hospital, Korea University Guro Hospital, Samsung Medical Center, and Hallym University Medical Center. The investigation will conform to the principles outlined in the Declaration of Helsinki. The study protocol has been registered in ClinicalTrials.gov (NCT04470284). All the authors are responsible for the study design, data acquisition, data analysis, and manuscript writing and editing. CONSORT checklist are included in the Supplementary Data 1.
Overview
The study flow is presented in Figure 1. This trial is a prospective, randomized, open-label, multicenter trial to evaluate the efficacy of SMBP with a mobile application-based feed-back algorithm (SMBP-App) compared with SMBP alone.
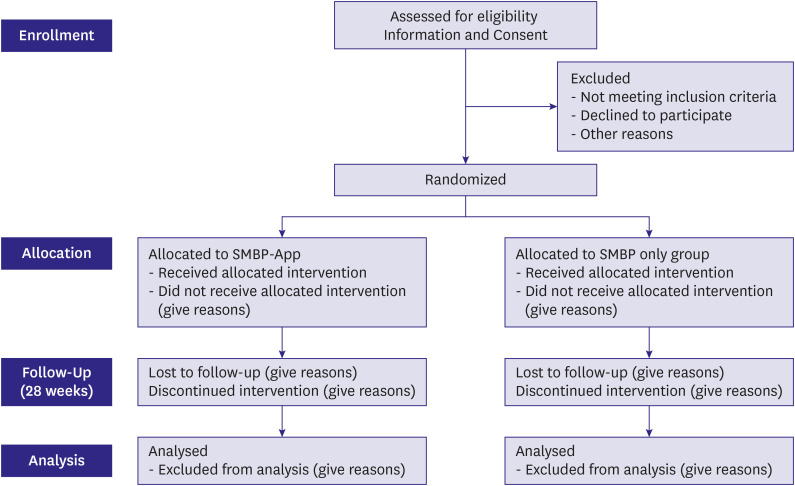
Patients with hypertension will be randomly assigned to the SMBP-App (intervention) group and SMBP-alone (control) groups. In the SMBP-alone group, the patients will perform home BP measurement and will receive the standard care. In the SMBP-App group, the patients will perform home BP measurement and will receive instructions from the mobile application in response to the obtained BP value.
The aim of this study will be to evaluate whether SMBP-App is superior to SMBP-alone in terms of BP reduction and drug adherence in patients with hypertension.
The trial has been approved by the relevant institutional review boards of each center. The protocol of this trial has been registered on Clinicaltrials.gov (registration number: NCT04470284). The study will comply with the Declaration of Helsinki.
Patients
We will enroll patients with uncomplicated essential hypertension aged 19 years or older with a systolic BP of 140 mmHg or greater and a diastolic BP of 90 mmHg or greater while receiving at least one anti-hypertensive drug. The detailed inclusion and exclusion criteria are listed in Table 1.
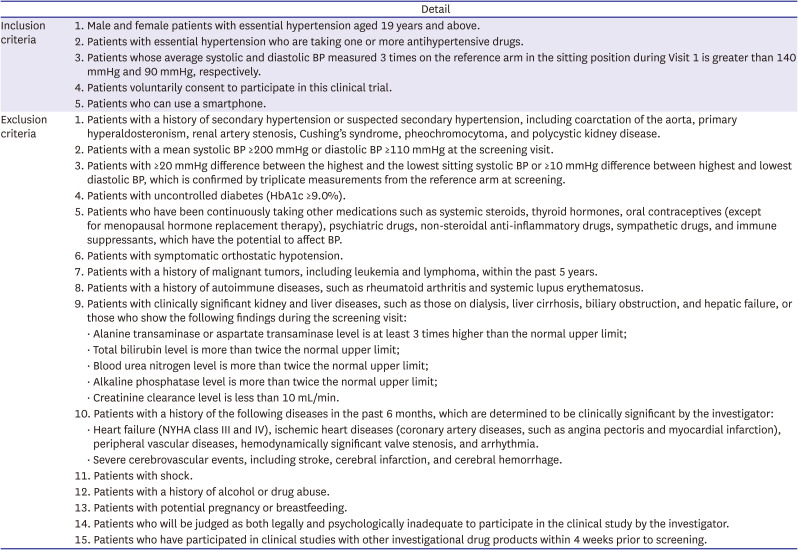
Table 1
Inclusion and exclusion criteria
![]()
Blood pressure measurement device and mobile application
For the current study, we will use a Bluetooth-enabled BP monitor UA-651BLE (A&D medical, Sidney, Australia). UA-651BLE is a commercially available BP cuff that has been approved for home use because of its high accuracy.11)
We have developed the SMBP platform with a mobile application that can be downloaded from Google play-store and a lightweight web application eCRF-Lite System for physicians to observe the patients’ BP status (Figure 2A). The platform consists of four parts: the i) BP Recorder, ii) Knowledge Base Reasoner, iii) Database Lite, and iv) eCRF – Lite System (Supplementary Data 1). The “BP Recorder” connects the smartphone with the BP cuff via Bluetooth. Patients check their BP using the UA-651BLE BP monitor and system’s core component. The “Knowledge Base Reasoner” asks the users about drug intake and symptoms (e.g., dizziness) based on BP values. The embedded algorithm in the Knowledge Base Reasoner analyzes the data input and generates recommendation for the users, e.g., an alarm message, if an abnormal BP is detected. “Database” uses the SQLite database for the mobile app and the SQL Server for permanent storage on a cloud, and it stores the patients’ information using Data Model Manager, which controls the schema, whereas Data Access Object Management stores, modifies, and deletes data in form of instances. The details of the SMBP platform are explained in the Supplementary Data 1 of the manuscript. The application illustrates the trend of recorded BP in days and weeks (Figure 2B).
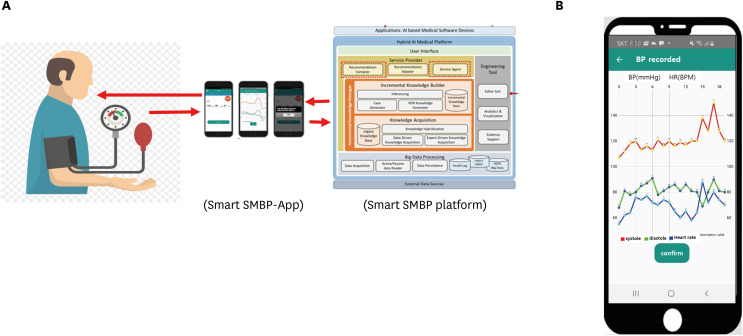
Figure 2
SMBP platform. (A) SMBP platform connects the smartphone with the BP cuff via Bluetooth and gives instructions in response to the measured BP value according to the embedded algorithm. (B) The application illustrates the trend of the recorded BP in days and weeks.
BP = blood pressure; SMBP = self-monitoring of blood pressure.
![]()
Study process
This trial is a prospective, randomized, open-label, multicenter trial to evaluate the efficacy of SMBP-App compared with SMBP alone. Patients with hypertension will be randomly assigned to the SMBP-App (intervention) and SMBP alone (control) groups at 5 tertiary hospitals in Korea. After randomization, both groups will download the mobile application from the Google Play-Store and install it on their smartphones After installation of the software, the application pairs automatically with the Bluetooth BP monitor. The difference in the mobile Apps is that the patients in the SMBP-App group will receive instructions from the mobile application in response to the obtained BP value. To be more specific, the SMBP-App will ask the patient’s opinion whether the measured BP is high, normal, or low, and whether the patients took the prescribed BP medication to enhance the awareness, vigilance, and drug adherence. In the SMBP-alone group, the patients will perform home BP measurement and receive the standard care.
Patients will continue their current antihypertensive drug for 24 weeks. Follow-up visits will be scheduled at 12 and 24 weeks after randomization. If BP value is not within the target range, the BP medication can be modified at the discretion of the treating physicians.
Study endpoints
The primary endpoint of the study is the mean home systolic BP change from randomization to 24 weeks. The key secondary endpoint is drug adherence from randomization to 24 weeks. Other secondary endpoints include the home diastolic BP from randomization to 12 weeks; 24-hour ambulatory systolic and diastolic BP reduction from 12 weeks to 24 weeks; sitting office systolic and diastolic BP at 24 weeks; home systolic and diastolic BP at 12 and 24 weeks; and drug adherence at 12 and 24 months.
Randomization
Randomization will be performed according to a pre-designed block randomization method. The randomization block will be generated by an independent statistician who is unrelated to this study using the SAS randomization program. Randomization will be performed in a 1:1 ratio, following the consecutive order.
Measurement of drug adherence
The drug adherence will be assessed with the “pill-count.” The patients will bring the remaining tablets to each scheduled visit during the clinical follow-up period. Examiners will count the number of returned drugs and calculate the drug adherence as follows:

If a discrepancy is present, the examiners will record the reason for the difference. The overall medication adherence should be at least 75% or more during the trial. Participants who will not satisfy this criterion will be excluded from the per-protocol (PP) analysis.
Statistical analysis
Data will be presented as numbers and frequencies for categorical variables and means ± standard deviations or median with interquartile range for continuous variables. For comparisons between the SMBP-App group and SMBP-only group, the χ2 test or Fisher’s exact test will be used for the categorical variables, and the unpaired Student t-test for the continuous variables, as appropriate. Fisher’s exact test will be used when the expected frequencies is less than 5. In addition, analysis of covariance will also be conducted to analyze the BP change from baseline and follow-up.
The data will be primarily analyzed according to the intention-to-treat rule including all randomized participants. We also plan a PP analysis for patients with drug adherence of 75% or less. One-sided p values <0.05 will be considered statistically significant. The analyses will be performed by a professional statistician.
DISCUSSION
We developed a mobile health platform for a tailored intervention in hypertensive patients. The mobile application provides alerts for BP measurement reminders, tracks the BP and other biometric measurement, and visualizes the BP trend in easy-to-interpret graphs. It also provides specific instruction in response to the measured BP value, such as taking medication, if a high BP is measured. In this prospective, randomized, open-label study, we will evaluate whether SMBP-App can reduce BP and increase the drug adherence compared to SMBP alone.
Hypertension is identified as the leading risk factor for death and disability-adjusted life-years lost in 2010 according to the Global Burden of Disease Study.14) Hypertension is a modifiable risk factor and controlling hypertension is highly effective to prevent cardiovascular disease.5)15)16)17)18)
Self-monitoring of blood pressure alone
SMBP will increase the patients’ awareness; nonetheless, if the patients have an abnormal BP value, the patients may not know how to respond to the measured BP. Previous studies showed that SMBP increased the drug adherence; however, it happened only in combination with other adherence-enhancing strategies such as patient counseling by nurses, pharmacists, or a telephone-linked system.19)
Self-monitoring of blood pressure with the mobile health application
Currently, smartphones are available to most people, and there are many mobile health apps for the management of BP. These apps have similar interfaces including features of recording, tracking, analyzing, visualizing the results with intuitive graphics and tables, and even sharing the BP information using other mobile devices. Nonetheless, they do not provide pertinent instruction on how to act in response to the obtained BP value. Usually, the patients need to bring the BP data to the physician encounters to receive “feedback,” i.e., an appropriate response. This may take days, weeks, and even months, depending on the time interval for the routine clinic visit. Theoretically, the visualization of captured BP value and their temporal changes can alert the patients and change their behavior, such as improved drug adherence. However, the effect of the mobile health app on BP control was rather disappointing. Morawski et al.20) showed in a randomized, controlled study with 411 patients that patients randomized to use a smartphone app had only a slight improvement in self-reported medication adherence, but no change in the systolic BP was found compared with controls. By contrast, there was a greater reduction in BP when patients with SMBP were connected with health care professionals who may send text messages, or nurses who give treatment recommendations.21) Although this type of interaction between patients and health care professionals may be the ideal situation, it may not be realizable due to the high cost and shortage of healthcare providers.
Self-monitoring of blood pressure with the mobile application-based feed-back algorithm
With enormous advancements in information and communication technologies artificial intelligence (AI) and clinical decision support system (CDSS) have proven efficacy. Our group developed AI-CDSS for diagnosis of heart failure with high diagnostic accuracy.22) In line with the application of information technology in medical practice, we developed a mobile application-based feed-back algorithm for BP control. The conventional time interval between daily BP measurement and receiving feedback in the clinic is so long that the value of daily BP measurement can be questioned. To provide immediate feedback, a “call center” can be operated that can monitor and respond to SMBP value by phone. However, its operation is very expensive. Here, we seek to determine whether the interaction between patients and health care professionals may be replaced by SMBP with the mobile application-based feed-back algorithm. Mobile health app is a simple and cost-effective method, which is suitable for broad utilization and implementation among hypertension patients to monitor and record their BP at home. The SMBP-app will take over the “call center function” but provides immediate feedback at a low cost. Nonetheless, the interventions by CDSS application are simple. The SMBP-App captures, archives, and visualize the BP value like other conventional SMBP mobile health app; in addition, it educates the patients and reminds of taking their BP medication. These simple interventions will increase the alertness, awareness, and drug adherence substantially, eventually leading to better clinical outcomes. In addition, the SMBP app may have potential long-term cost benefit. It is well known that each 10 mmHg systolic BP reduction leads to 10% reduction in all-cause deaths, and 20% reduction heart failure. Heart failure is the leading cause for hospitalization and main health care burden in the modern society.23) To the best of our knowledge, our study is the first of its kind that evaluates the effectiveness of SMBP in conjunction with a designated mobile health app, which has a dedicated algorithm and a knowledge base to improve the BP control. If we can confirm its efficacy in this randomized controlled study, SMBP in conjunction with an appropriate mobile health app may be an effective solution to control hypertension.
Limitations
There are several limitations. The major limitation is that the newly developed algorithm that makes recommendations based on BP values has not been validated in the effectiveness and safety, which are also the main objective of these study. In addition, since we will only enroll patients who have a smartphone and are able to use it, the results of our trial may not be generalizable to other populations of individuals with poorly controlled hypertension, who may have different sociodemographic and comorbidity characteristics.
 XML Download
XML Download