

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Despite the widespread introduction of percutaneous coronary intervention (PCI) into clinical practice, the mortality rate in patients with ST-segment elevation myocardial infarction (STEMI) remains high and averages 5–7%.1)2)3)4) This state of affairs is due to the fact that drugs used to treat acute myocardial infarction (AMI) do not have a significant effect on the mortality rate in patients with AMI.5)6) Investigators have been developing pharmacological agents that can increase cardiac tolerance to ischemia/reperfusion (I/R) for about 50 years. In studies that were carried out in the 70s and 90s, compounds were injected before coronary artery occlusion (CAO) and reperfusion in animals. Currently, many investigators believe that reperfusion injury is responsible for up to 50% of infarct size.7)8) For this reason, pharmacological agents are now increasingly administered to animals after cardiac ischemia. Such studies are close to real clinical practice since patients with AMI are admitted with ischemic cardiac injury. Death of cardiomyocytes in the ischemic zone is almost complete 6 hours after CAO.9) Therefore, reperfusion reduces infarct size only if it is performed no later than 6 hours after the onset of AMI.
In recent years, studies have appeared in which it has been shown that in I/R cardiac injury can be involved platelets.10)11)12) Purpose of this review article: to summarize and analyze articles on the cardioprotective effect of pharmacological agents affecting the functional state of platelets, in animals with I/R of the heart and in patients with AMI.
PLATELETS
It is known that platelets are activated in acute coronary syndrome.13)14) In parallel with activation, an increase in P-selectin expression by platelets is observed.13)14)
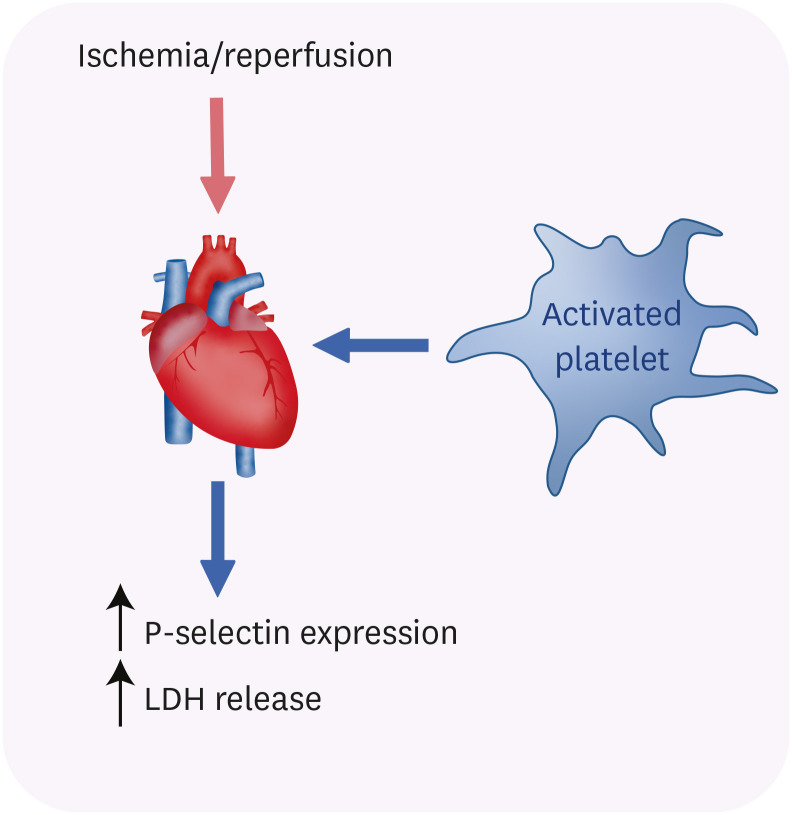
Platelets aggravated ischemic/reperfusion injury of the heart. In 2002, it was hypothesized that the effect of platelets on the myocardium depends on their activation.12) Pig platelets were obtained 48 minutes before CAO, 10 minutes after reperfusion and after a 60-minute sham operation. The expression of P-selectin was higher in platelets isolated during reperfusion than in platelets isolated before ischemia or after the sham operation. The isolated perfused rat heart was subjected to global I/R, 5 minutes before global ischemia, platelets were added to a solution, which was used for perfusion of the isolated rat hearts. Lactate dehydrogenase (LDH) release during reperfusion was similar in hearts perfused with a solution containing platelets isolated before CAO or after a sham operation. However, LDH release increased if platelets were isolated from blood of pigs during reperfusion. Platelet activation by thrombin increased P-selectin expression and LDH release from the isolated rat heart (Figure 1). A close correlation was established between P-selectin expression and LDH release and platelet accumulation in the myocardium. Investigators concluded12) that the pathogenic effect of platelets on the reperfused heart depended on their activation, which is characterized by P-selectin expression. This expression is enhanced in response to I/R. The evidence suggests that platelets play an important role in cardiac I/R injury.
Figure 1
Effects of platelet activation during ischemia/reperfusion.
The pathogenic effect of platelets on the reperfused heart depends on their activation, which causes the expression of P-selectin and LDH release.
LDH = lactate dehydrogenase.
Platelets protect the heart against I/R. However, platelets can not only exacerbate I/R cardiac injury but also enhance cardiac tolerance to I/R. The isolated perfused rat heart was subjected to global ischemia (30 minutes) and reperfusion (60 minutes).15) Platelets of healthy volunteers were added to Krebs-Henseleit solution 10 minutes before the onset of ischemia. It was detected that platelets promoted the infarct size reduction by about 15%.15) Platelets of diabetic patients had no effect on infarct size. It was demonstrated that platelets of healthy volunteers induced phosphorylation of extracellular signal-regulated kinases 1/2 (ERK1/2). Platelets of diabetic patients did not trigger phosphorylation of ERK1/2. It was detected that inhibition of ERK1/2, protein kinase C (PKC), phosphatidylinositol (4,5)-bisphosphate 3-kinase (PI3K) abolished the infarct-sparing effect of platelets.15) It should be noted that ERK1/2, PI3K, and PKC are involved in the cardioprotective effect of ischemic pre- and postconditioning.16)17)18) These data indicate that some cardioprotective substances could be released from platelets and increase cardiac tolerance to I/R.
Purinergic P2Y12 (adenosine diphosphate agonist) receptor is a receptor that is expressed in platelets. P2Y12 receptor blockers (cangrelor, ticlopidine, clopidogrel, prasugrel, ticagrelor) are platelet aggregation inhibitors that are used to restore coronary perfusion and prevent recurrent ischemic events in AMI.10)11) In recent years, evidence has emerged that the P2Y12 receptor antagonist cangrelor can not only inhibit platelet aggregation but also reduces infarct size in rabbits.19) According to Yang et al.,19) cangrelor reduces infarct size when it is administered intravenously before reperfusion, it acts in a situation as close as possible to clinical practice. It was reported that the infarct-limiting effect of cangrelor does not occur in studies in the isolated perfused rabbit heart.19) It is indirect evidence of platelets involvement in the development of the cardioprotective effect of cangrelor. However, the protective effect of cangrelor does not appear to be associated with a change in platelet aggregation. Aspirin also inhibits platelet aggregation. However, pretreatment with aspirin before CAO did not affect infarct size in rabbits.19) It was reported that administration of aspirin at reperfusion of the heart had no effect on infarct size in rats.20)21) There is no evidence that single administration of aspirin alone can decrease infarct size in patients with AMI and reperfusion therapy. The P2Y12 receptor antagonist ticagrelor demonstrated the infarct-reducing effect when it was administered to rats 5 minutes before reperfusion.22) The aforementioned studies suggest an important role of platelet P2Y12 receptors is in regulating cardiac resistance to reperfusion.
These experimental findings indicate that platelets play the important role in cardiac reperfusion injury.
THE P2Y12 RECEPTOR ANTAGONISTS
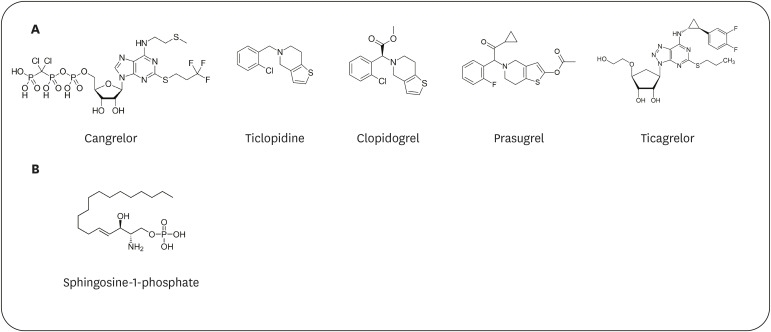
Purinergic P2Y12 receptor belongs to G-protein-coupled receptors and can interact with Gi-protein.23) P2Y12 receptor is expressed by cardiomyocytes and platelets. Its agonists are nucleotides such as ATP, ADP, UTP, UDP, and some other compounds.24) Its antagonists are: cangrelor, ticlopidine, clopidogrel, prasugrel, and ticagrelor (Figure 2A).24) Clopidogrel, ticagrelor and prasugrel, like thienopyridines, require hepatic cytochrome P450-mediated conversion of prodrug to its active metabolite inhibiting the P2Y12 receptor.23)25) Cangrelor is not thienopyridine and therefore does not require activation of hepatic conversion to an active compound.25) Clopidogrel irreversibly inhibits the P2Y12 receptor.10)25) Cangrelor and ticagrelor are reversible antagonists of the P2Y12 receptor.11)23) The cardiovascular effects of P2Y12 receptor antagonists are usually associated with platelet aggregation blockade.23)25)
Figure 2
P2Y12 receptor inhibitors. (A) Chemical structure of P2Y12 receptor antagonists (B) Chemical structure of S1P.
S1P = sphingosine-1-phosphate.
Experimental data
The molecular mechanism of cardioprotective effect of P2Y12 antagonists (Table 1). The isolated perfused rat heart was subjected to global ischemia (40 minutes) and reperfusion (60 minutes).26) Platelets obtained from patients with AMI or platelets of healthy volunteers were added to the perfusion solution. Platelets of patients with AMI exacerbated I/R cardiac injury, and platelets of healthy volunteers did not affect cardiac resistance to I/R. If platelets of patients with AMI were preliminarily incubated with cangrelor, the pathogenic effect of platelets disappeared. Investigators concluded that activated platelets in patients with AMI exacerbate I/R cardiac injury, while P2Y12 receptor blockade eliminates their negative effect on the heart. It has been demonstrated that intravenous administration of cangrelor to rabbits 10 minutes before reperfusion contributes to a 45% reduction in the infarct size/area at risk (IS/AAR) ratio.27) The administration of ticagrelor to rabbits 1 hour before CAO also contributed to a 45% decrease in the IS/AAR ratio. Inhibitors of PKC and PI3K eliminated an infarct-reducing effect of ticagrelor. The infarct-sparing effect of ticagrelor has been confirmed in other studies.28)29) It was found that ticagrelor is an inhibitor of equilibrative nucleoside transporter 1 (ENT-1) (Ki=41 nmol/L),30) thereby investigators suggested that the infarct-reducing effect of ticagrelor could be mediated via an increase in adenosine content in myocardial tissue. It was found that the infarct-reducing effect of ticagrelor was associated with an increase in the adenosine level in myocardial tissue.22) Adenosine receptor antagonists did not use, thus it remains unclear whether adenosine is involved in the cardioprotective effect of ticagrelor.22) The isolated perfused rat heart was subjected to global ischemia (40 minutes) and reperfusion (2 hours).31) Ticagrelor was added to a perfusion solution at a final concentration of 3 µM or 10 µM. This concentration was enough to inhibit platelet aggregation in vitro. Ticagrelor had no effect on infarct size. Investigators concluded that adenosine is not involved in the cardioprotective effect of ticagrelor. If the cardioprotective effect of ticagrelor was mediated through an increase of the adenosine level in myocardial tissue, ticagrelor could protect the isolated rat heart against I/R.31) Ticagrelor had a high (Ki=190 nmol/L) affinity for the adenosine A3 receptor.32) However, if the A3 receptor is involved in the cardioprotective effect of ticagrelor, this P2Y12 inhibitor could increase tolerance of the isolated heart to I/R. In a study carried out on macaques, cangrelor also had an infarct-limiting effect when administered before reperfusion.32) This data suggests that cangrelor may have an infarct-reducing effect in a situation very similar to clinical practice. In a study performed in rabbits with CAO and reperfusion, it was detected that cangrelor has an infarct-limiting effect if it was administered before reperfusion and it does not affect the IS/AAR ratio if it is administered after 10 minutes of reperfusion.19) Therefore, it has been suggested that P2Y12 receptor antagonists should be administered to patients with AMI before PCI. Aspirin, which also inhibits platelet aggregation, did not affect infarct size.19)20)21) Consequently, the infarct-reducing effect of cangrelor is not a direct result of inhibition of platelet aggregation. Rats underwent CAO (30 minutes) and reperfusion (2 hours).27) Cangrelor was injected as a bolus 10 minutes before reperfusion and then infused in reperfusion. Cangrelor reduced infarct size by 45%. A combination of cangrelor and ischemic preconditioning did not trigger an additive cardioprotective effect.27) Co-administration of cariporide and cangrelor did not result in the additive effect. Ticagrelor reduced infarct size by 25%. It was found that PKC, PI3K are involved in the infarct-reducing effect of ticagrelor.27) These findings demonstrated that the signaling mechanism of the cardioprotective effect of P2Y12 receptor antagonists and ischemic preconditioning is similar. The infarct-sparing effect of cangrelor could not be demonstrated in a study with the isolated perfused rat heart,19) that indicates the involvement of some blood components in its development. In a study performed in rats with CAO and reperfusion, clopidogrel and ticagrelor were administered intraperitoneally 5 minutes before reperfusion.22) Ticagrelor had an infarct-limiting effect, clopidogrel did not affect the IS/AAR ratio. It can be supposed that this difference could be due to slower clopidogrel absorption from the abdominal cavity. Ticagrelor is known to inhibit platelet aggregation faster than clopidogrel.25) It can be hypothesized that because it acts faster than clopidogrel that it increases cardiac resistance to reperfusion. Rats underwent CAO (45 minutes) and reperfusion.33) Ticagrelor was administered intragastrically after the onset of reperfusion. This P2Y12 antagonist reduced infarct sized and decreased the mRNA levels of transcription factor nuclear factor-κB (NF-κB), interleukin-6 (IL-6), and tumor necrosis factor-α (TNF-α) in the area at risk 24 hours 3 and 7 days after the onset of reperfusion.33) Ticagrelor reduced plasma C-reactive protein (CRP) and N-terminal prohormone of brain natriuretic peptide levels at 24 hours and 3 days after reperfusion.33) These findings indicate that ticagrelor can prevent a delayed reperfusion injury of the heart,34) through inhibition of the pro-inflammatory NF-κB-dependent pathway. It was reported that ticagrelor (when administered to rats for 4 weeks) prevents post-infarction remodeling of the heart, clopidogrel does not possess similar properties.22)
Table 1
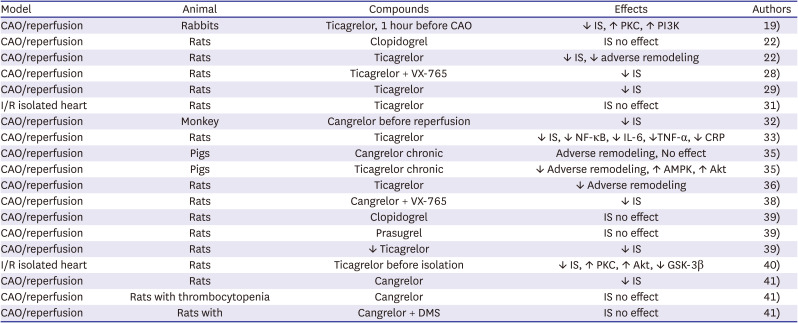
The molecular mechanism of cardioprotective effects of P2Y12 antagonists in experimental studies
| Model | Animal | Compounds | Effects | Authors |
|---|---|---|---|---|
| CAO/reperfusion | Rabbits | Ticagrelor, 1 hour before CAO | ↓ IS, ↑ PKC, ↑ PI3K | 19) |
| CAO/reperfusion | Rats | Clopidogrel | IS no effect | 22) |
| CAO/reperfusion | Rats | Ticagrelor | ↓ IS, ↓ adverse remodeling | 22) |
| CAO/reperfusion | Rats | Ticagrelor + VX-765 | ↓ IS | 28) |
| CAO/reperfusion | Rats | Ticagrelor | ↓ IS | 29) |
| I/R isolated heart | Rats | Ticagrelor | IS no effect | 31) |
| CAO/reperfusion | Monkey | Cangrelor before reperfusion | ↓ IS | 32) |
| CAO/reperfusion | Rats | Ticagrelor | ↓ IS, ↓ NF-κB, ↓ IL-6, ↓TNF-α, ↓ CRP | 33) |
| CAO/reperfusion | Pigs | Cangrelor chronic | Adverse remodeling, No effect | 35) |
| CAO/reperfusion | Pigs | Ticagrelor chronic | ↓ Adverse remodeling, ↑ AMPK, ↑ Akt | 35) |
| CAO/reperfusion | Rats | Ticagrelor | ↓ Adverse remodeling | 36) |
| CAO/reperfusion | Rats | Cangrelor + VX-765 | ↓ IS | 38) |
| CAO/reperfusion | Rats | Clopidogrel | IS no effect | 39) |
| CAO/reperfusion | Rats | Prasugrel | IS no effect | 39) |
| CAO/reperfusion | Rats | ↓ Ticagrelor | ↓ IS | 39) |
| I/R isolated heart | Rats | Ticagrelor before isolation | ↓ IS, ↑ PKC, ↑ Akt, ↓ GSK-3β | 40) |
| CAO/reperfusion | Rats | Cangrelor | ↓ IS | 41) |
| CAO/reperfusion | Rats with thrombocytopenia | Cangrelor | IS no effect | 41) |
| CAO/reperfusion | Rats with | Cangrelor + DMS | IS no effect | 41) |
AMI = acute myocardial infarction; AMPK = AMP-activated protein kinase; CAO = coronary artery occlusion; IS = infarct size; CRP = C-reactive protein; DMS = dimethylsphingosine = a sphingosine kinase inhibitor; GSK-3β = glycogen synthase kinase-3β; I/R = ischemia/reperfusion; IL-6 = interleukin-6; NF-κB = nuclear factor-κB; PI3K = phosphatidylinositol (4,5)-bisphosphate kinase; PKC = protein kinase C; TNF-α = tumor necrosis factor-α; VX-765 = caspase-1 inhibitor.
P2Y12 antagonists attenuate adverse post-infarction remodeling of the heart. Pigs underwent CAO (1 hour) and reperfusion (42 days).35) It was used chronic administration of placebo, clopidogrel, ticagrelor. It was found that ticagrelor improved contractile function of the heart. Clopidogrel had no effect. Ticagrelor increased phosphorylated Akt and AMP-activated protein kinase (AMPK) content in myocardial tissue. It was suggested that ticagrelor attenuated adverse post-infarction myocardial remodeling through activation of Akt and AMPK.35) Chronic administration of clopidogrel attenuated fibrosis of the rat heart 4 weeks after CAO and reperfusion.22) Ticagrelor, but not clopidogrel, reduced an increase in TNF-α, IL-1β, and IL-18 in myocardial tissue after reperfusion.22) Rats underwent CAO (40 minutes) and reperfusion.36) Ticagrelor, aspirin, ticagrelor + aspirin, and prasugrel were administered daily beginning 7 days after the onset of reperfusion. All compounds and a combination of ticagrelor and aspirin reduced platelet aggregation by about 50%. Ticagrelor, aspirin, ticagrelor + aspirin reduced the plasma CRP level, prasugrel had no effect. Ticagrelor and aspirin attenuated cardiac hypertrophy 28 days after I/R and prevented a decrease in left ventricular ejection fraction. Ticagrelor and aspirin reduced a number of TUNEL positive (apoptotic) cells, decreased the fibrosis area, attenuated an increase in mRNA content of atrial natriuretic peptide, brain natriuretic peptide, collagen-I and collagen-III in myocardial tissue. It was surprising, but prasugrel and a combination of ticagrelor and aspirin did not prevent adverse myocardial remodeling. Investigators suggested that ticagrelor- and aspirin-triggered attenuation of adverse myocardial remodeling is a result of increased 15-epi-lipoxin A4 production that exhibited cardioprotective properties.36) It remains unclear why ticagrelor + aspirin and prasugrel had no effect on the level of this eicosanoid. The use of ticagrelor on a long-term basis in patients with AMI could be effective in preventing post-infarction cardiac remodeling. However, acute administration of all P2Y12 receptor antagonists can induce bleeding. Chronic administration of these compounds will also induce bleeding.
The combined use of P2Y12 antagonists. Currently, a combination of drugs, for example, aspirin, statins, β-adrenergic receptor blockers, angiotensin receptor blockers are used to treat AMI.37) Investigators continue the search for combinations of drugs which can increase the effectiveness of treatment of AMI. In a study performed in rats with CAO (60 minutes) and reperfusion (2 hours), it was demonstrated that pretreatment with the caspase-1 inhibitor VX-765 can decrease infarct size by about 50%.38) Cangrelor was injected 10 minutes prior to reperfusion followed by 6 µg/kg/min continuous infusion. It decreased infarct size by approximately 40%. Combined administration of VX-765 and cangrelor can decrease infarct size by 80%.38) It is a very strong cardioprotective effect. Consequently, both compounds act as synergists. It was demonstrated that administration of ticagrelor prior to reperfusion of the rat heart promotes a decrease in infarct size by 29%, injection of VX-765 prior to reperfusion reduced infarct size by 52%.28) Combined administration of VX-765 and ticagrelor promoted the infarct size reduction by 71%. Consequently, these compounds act also as synergists. In 2021, Hjortbak et al.39) confirmed the infarct-reducing effect of ticagrelor in rats with CAO (30 min) and reperfusion (2 hours). They found that Pretreatment with cangrelor or prasugrel did not reduce infarct size in rats.39) The isolated perfused rat heart was subjected to global ischemia (30 minutes) and reperfusion (60 minutes).40) Ticagrelor (150 mg/kg) was orally administered to rats for three consecutive days before isolation of the heart. The hearts were pretreated with the NOD-like receptor pyrin domain containing 3 (NLRP3) inflammasome inhibitor ethyl 2-((2-chlorophenyl)(hydroxy)methyl)acrylate (INF) in vitro. In addition, it was used a combination of ticagrelor + INF. It was detected that ticagrelor decreased infarct size by 29%, INF reduced infarct size by 45%. The combined use of compounds did not induce an additive effect. If ticagrelor was added to a perfusion solution before I/R of the isolated heart, it did not affect infarct size. Both ticagrelor or INF increased the levels of phosphorylated Akt, phosphorylated (activated) protein kinase C (p-PKC), and phosphorylated (inhibited) glycogen synthase kinase-3β (GSK-3β) in myocardial tissue.40) It should be noted activation of Akt, PKC, and inhibition of GSK-3β are involved in the cardioprotective effect of ischemic pre- and postconditioning.16)
Consequently, the cardioprotective effect of ticagrelor is likely mediated via inhibition of the P2Y12 receptor of platelets. The same kinases are involved in the signaling mechanism of the cardioprotective effect of ticagrelor and INF. Apparently, for this reason, for the additive effect was not detected.
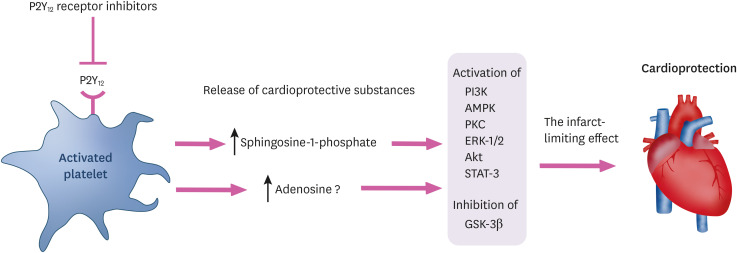
The hypothetical mechanism of the cardioprotective effect of P2Y12 receptor inhibitors
The role of sphingosine-1-phosphate (S1P) and adenosine in the cardioprotective effect of P2Y12 antagonists (Table 2). Studies now being performed are aimed at clarifying the mechanism of the infarct-reducing effect of cangrelor in vivo. As previously cited, cangrelor was not able to increase resistance of the isolated perfused heart to I/R. Consequently, it is reasonable to suppose that blood cells or platelets can participate in its cardioprotective effect. It was hypothesized that platelets may be the source of cardioprotective substances.41) A study was performed utilizing rats with CAO and reperfusion. Thrombocytopenia was induced with antibodies to platelets. Thrombocytopenia did not affect the IS/AAR ratio, thus confirming that a disturbance of platelet aggregation is not cardioprotective. Cangrelor did not affect infarct size in rats with thrombocytopenia.41) These findings indicate that cangrelor can initiate the release of cardioprotective substances from platelets. It is possible that one of these substances is S1P (Figure 2B), which increases cardiac resistance to I/R.42)43)44) The isolated murine heart was subjected to global ischemia (20 minutes) and reperfusion (30 minutes).45) Pretreatment with S1P reduced creatine kinase (CK) release and infarct size. PKCε knockout did not eliminate the cardioprotective effect of S1P.45) Mice underwent CAO (1 hour) and reperfusion.46) The infarct size was increased by >50% in S1P(2,3) receptor double-knockout mice.46) The isolated rat heart was subjected global ischemia (40 minutes) and reperfusion (40 minutes).47) S1P reduced infarct size by about 80%. Pretreatment with the PI3K inhibitor wortmannin, the PKC inhibitor chelerythrine, the S1P1 and S1P3 receptor antagonist VPC23019 abolished this effect of S1P.47) The isolated rat heart was subjected to global ischemia (30 minutes) and reperfusion (90 minutes).48) FTY720, a S1P1/3 receptor agonist, improved recovery of contractile function of the heart in reperfusion. In addition, FTY720 reduced a number of TUNEL positive cells, increased phosphorylation of ERK1/2.48) There is evidence that S1P is involved in ischemic preconditioning of the heart.49) In a study with H9C2 cells subjected to the impact of bacterial lipopolysaccharide, it was demonstrated an anti-inflammatory effect of S1P.50) S1P binds and activates five receptor subtypes: S1P1, S1P2, S1P3, S1P4, S1P5, widely expressed in different organs, tissues, and cells.51) The S1P1 receptor was found in the heart, the S1P3 receptor was detected in vessels.51) Inhibition of sphingosine kinase by dimethylsphingosine eliminates the cardioprotective effect of cangrelor.41) Thus, the protective mechanism of cangrelor seems to be associated with enhancement of S1P synthesis and its release from platelets (Figure 3).44) S1P resulted in the cardioprotective effect in a study utilizing the isolated perfused rat heart.52) Moreover, S1P is able to prevent cardiac reperfusion injury in vivo.53) Ye et al.22) performed a comparative analysis of the cardioprotective effect of clopidogrel and ticagrelor in rats. Both compounds were injected 5 minutes before reperfusion. Ticagrelor demonstrated the infarct-limiting effect, decreased a number of apoptotic cells in the myocardium and clopidogrel did not reduce infarct size and apoptosis. The authors found that only ticagrelor induced an increase in the adenosine level in myocardial tissue. They hypothesized that endogenous adenosine is involved in the cardioprotective effect of ticagrelor. However, these investigators did not use adenosine receptor antagonists. Therefore, their hypothesis did not confirm before. There is evidence that PKC, GSK-3β, Akt-kinase, and PI3K are involved in the cardioprotective effect of ticagrelor.27)40) If S1P is the main trigger of the infarct-reducing effect of P2Y12 receptor antagonists, it must stimulate indicated kinases. Indeed, S1P increased PKC activity in myocardial tissue.54) In a study performed with CCL39 cells, it was demonstrated that S1P can activate ERK, PI3K, and PKC.55) It was demonstrated that S1P reduced infarct size in mice with CAO and reperfusion via activation of Akt and signal transducer and activator of transcription 3 (STAT-3) in mice.56) S1P did not affect infarct size in STAT-3 knockout mice. The infarct-reducing effect of S1P was abolished by AG490, an inhibitor of epidermal growth factor receptor, Janus kinase-1/2, and STAT3. The PI3K inhibitor wortmannin eliminated an infarct-limiting effect of S1P. PD98059, an inhibitor of mitogen-activated protein kinase kinase and ERK1/2, had no effect on S1P-induced cardioprotection.56) It was concluded that PI3K and STAT3 are involved in the cardioprotective effect of S1P.56) In a study with wild-type and S1P receptor-1 knockout mice it was demonstrated that the S1P receptor-1 loss aggravated adverse post-infarction remodeling of the heart.57) It was reported that S1P can prevent reperfusion cardiac injury via Akt and GSK-3β phosphorylation in rats.53) PI3K is involved in the infarct-sparing effect of S1P in reperfusion.53) Consequently, there is every reason to believe that S1P could be a molecule, which mediates the infarct-reducing effect of P2Y12 receptor antagonists.
Table 2
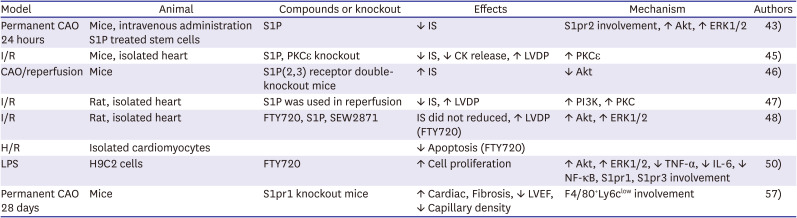
The molecular mechanism of cardioprotective effects S1P
| Model | Animal | Compounds or knockout | Effects | Mechanism | Authors |
|---|---|---|---|---|---|
| Permanent CAO 24 hours | Mice, intravenous administration S1P treated stem cells | S1P | ↓ IS | S1pr2 involvement, ↑ Akt, ↑ ERK1/2 | 43) |
| I/R | Mice, isolated heart | S1P, PKCε knockout | ↓ IS, ↓ CK release, ↑ LVDP | ↑ PKCε | 45) |
| CAO/reperfusion | Mice | S1P(2,3) receptor double-knockout mice | ↑ IS | ↓ Akt | 46) |
| I/R | Rat, isolated heart | S1P was used in reperfusion | ↓ IS, ↑ LVDP | ↑ PI3K, ↑ PKC | 47) |
| I/R | Rat, isolated heart | FTY720, S1P, SEW2871 | IS did not reduced, ↑ LVDP (FTY720) | ↑ Akt, ↑ ERK1/2 | 48) |
| H/R | Isolated cardiomyocytes | ↓ Apoptosis (FTY720) | |||
| LPS | H9C2 cells | FTY720 | ↑ Cell proliferation | ↑ Akt, ↑ ERK1/2, ↓ TNF-α, ↓ IL-6, ↓ NF-κB, S1pr1, S1pr3 involvement | 50) |
| Permanent CAO 28 days | Mice | S1pr1 knockout mice | ↑ Cardiac, Fibrosis, ↓ LVEF, ↓ Capillary density | F4/80+Ly6clow involvement | 57) |
Akt = Akt kinase; CAO = coronary artery occlusion; CK = creatine kinase; ERK1/2 = extracellular signal-regulated kinases; FTY720 = a S1P1/3 receptor agonist; F4/80+Ly6clow = reparative macrophage; IL-6 = interleukin-6; I/R = ischemia/reperfusion; IS = infarct size; LVDP = left ventricular developed pressure; LVEF = left ventricular ejection fraction; LPS = lipopolysaccharide; PI3K = phosphatidylinositol (4,5)-bisphosphate kinase; PKC = protein kinase C; S1P = sphingosine-1-phosphate; S1pr1 = sphingosine 1-phosphate receptor 1 = S1pr2 = the sphingosine 1-phosphate receptor 2 = SEW2871 = S1pr1 agonist; TNF-α = tumor necrosis factor-α.
Figure 3
The hypothetical mechanism of the cardioprotective effect of P2Y12 receptor inhibitors.
Inhibition of P2Y12 receptors results in the release of cardioprotective substance S1P from activated platelets. S1P increases PKC activity in myocardial tissue and can activate ERKs, PI3K, AMPK and PKC. S1P reduces infarct size in ischemia/reperfusion by activating Akt and STAT-3. S1P may prevent reperfusion injury of the heart through activation of Akt and inhibition of GSK-3β phosphorylation.
Inhibitors of P2Y12 receptors induce an increase in the level of adenosine in myocardial tissue. There is evidence that they can activate the A3 adenosine receptor. However, there is no evidence that endogenous adenosine or adenosine receptors are involved in reducing the infarction of inhibitors of P2Y12 receptors in vivo.
Akt = Akt kinase; AMPK = AMP-activated protein kinase; ERK = extracellular signal-regulated kinases; GSK-3β = glycogen synthase kinase-3β; PI3K = phosphatidylinositol (4,5)-bisphosphate 3-kinase; PKC = protein kinase C; S1P = sphingosine-1-phosphate; STAT-3 = signal transducer and activator of transcription 3.
Thus, convincing evidence has been obtained that cangrelor and ticagrelor have an infarct-reducing effect in vivo, which is not associated with inhibition of platelet aggregation. Cangrelor has been shown to cause the release of a cardioprotective substance from platelets. It now seems likely that this substance is S1P. It cannot be ruled out that the P2Y12 receptor antagonists may induce the release from platelets not only S1P and other substances which can increase cardiac tolerance to I/R. The aforementioned data indicate the feasibility of implementation of the clinical trial of combined therapy of AMI with P2Y12 receptor antagonists and VX-765.
Clinical data
The Clopidogrel in Unstable Angina to Prevent Recurrent Events (CURE) study included 12,562 patients with acute coronary syndrome (ACS) without ST-segment elevation who had PCI.58) The duration of this study was 1 year. All patients received aspirin. Some of them received clopidogrel (300 mg immediately, and then 75 mg once a day), while the other half received placebo. It was detected that in the clopidogrel group adverse events (death due to cardiovascular causes, myocardial infarction, stroke) were observed in 9.3% of cases, and in the placebo group, adverse events were observed in 11.4% (p<0.001). Treatment with clopidogrel reduced the incidence of heart failure within 12 months after STEMI.58) In a placebo-controlled multicenter study (Clopidogrel and Metoprolol in Myocardial Infarction Trial; COMMIT), 45,852 patients with AMI were included, some of them received clopidogrel (75 mg daily) in addition to aspirin, the other half received only placebo and aspirin.59) It was demonstrated that patients receiving clopidogrel had a low mortality rate (7.5%, p=0.03), and the rate of adverse events was reduced by 9% (p=0.002) (Table 3). In a multicenter, placebo-controlled study (The PCI-Clopidogrel as Adjunctive Reperfusion Therapy [CLARITY] study) included 3,491 patients with STEMI who underwent fibrinolysis after admission, and after 2–8 days of PCI.60) All patients received aspirin. Patients who received clopidogrel had a significantly lower death rate (p=0.03) in comparison to the placebo (aspirin) group. The rate of adverse events (death, re-infarction, stroke) after PCI in the clopidogrel group was 3.6%, and in the placebo group was 6.2% (p=0.008). These studies suggest that clopidogrel was highly effective in preventing the occurrence of adverse events in patients with AMI. In the CURE trial were included 12,562 patients with Non-STEMI ACSs.61) The patients were undergoing PCI or fibrinolytic therapy. All patients received aspirin. It was found that in-hospital mortality in patients undergoing PCI was low in the clopidogrel + aspirin group in comparison to the aspirin group. These groups are not different in the incidence of life-treating bleedings.61) The Harmonizing Outcomes with Revascularization of Acute Myocardial Infarction (HORIZONS-AMI) trial, published in 2009, included patients with STEMI (n=3,602) and PCI.62) All patients received glycoprotein IIb/IIIa inhibitors, bivalirudin, or unfractionated heparin. Clopidogrel was administered at a dose of 300 mg or a dose of 600 mg. This study indicated that in patients given clopidogrel (600 mg), the mortality rate was lower compared to the 300 mg dose group (1.9% vs. 3.1%, p=0.03), repeated myocardial infarction was (1.3% vs. 2.3%, p=0.02), and stent thrombosis was (1.7% vs. 2.8%, p=0.04) within 30 days after hospitalization. The drug did not increase the rate of bleeding. A Platelet Inhibition and Patient Outcomes (PLATO) Investigators was a randomized, double-blind, multicenter trial that included 18,624 patients with ACS and with STEMI and non-STEMI (NSTEMI).63) They received ticagrelor (loading dose of 180 mg, then 90 mg twice a day) or clopidogrel (loading dose of 300 mg or 600 mg, then 75 mg daily). After 12 months, adverse events (death from vascular causes, myocardial infarction, stroke) occurred in 9.8% of patients in the ticagrelor group, and in 11.7% of patients in the clopidogrel group (p<0.001). In a multicenter study (STEMI 2003 Registry Collaborators) it was included 7,193 patients with STEMI and PCI.64) All patients received pretreatment with 300 mg of aspirin. Clopidogrel reduced the 1-year all-cause mortality rate by 41% in comparison to aspirin alone.64) In a study it was included 198 patients with STEMI and PCI.65) Magnetic resonance imaging was performed for infarct size assessment after 7 days after PCI.65) Clopidogrel was administered at a dose of 300 mg and 600 mg. Infarct size was 21% less (p=0.03) in patients receiving the larger dose of clopidogrel. The myocardial salvage index was 49% higher when using 600 mg of clopidogrel. Therefore, clopidogrel has an infarct-reducing effect in patients with AMI and PCI. In the randomized Cangrelor versus Standard Therapy for Achieve Optimal Management of Platelet Inhibition (CHAMPION) trial, 6,327 patients with ACS with STEMI or NSTEMI were included.66) Patients (n=2,015) received clopidogrel. This study indicated that clopidogrel contributed to a decrease in infarct size, which was evaluated by the CK-MB level. The peak CK-MB level decreased by 47%.66)
Table 3
The cardioprotective effects of P2Y12 agonists in clinical studies
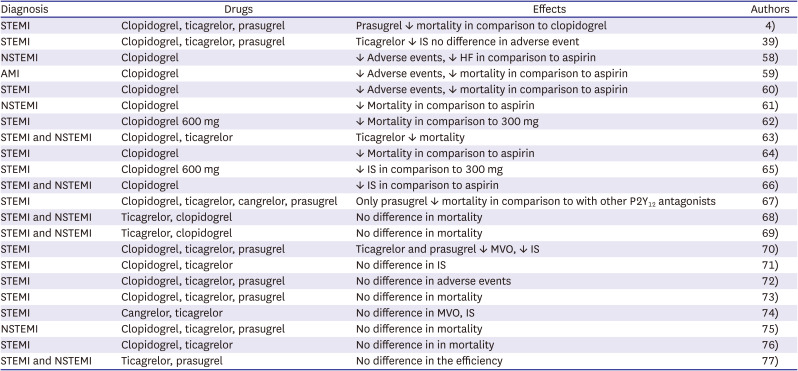
| Diagnosis | Drugs | Effects | Authors |
|---|---|---|---|
| STEMI | Clopidogrel, ticagrelor, prasugrel | Prasugrel ↓ mortality in comparison to clopidogrel | 4) |
| STEMI | Clopidogrel, ticagrelor, prasugrel | Ticagrelor ↓ IS no difference in adverse event | 39) |
| NSTEMI | Clopidogrel | ↓ Adverse events, ↓ HF in comparison to aspirin | 58) |
| AMI | Clopidogrel | ↓ Adverse events, ↓ mortality in comparison to aspirin | 59) |
| STEMI | Clopidogrel | ↓ Adverse events, ↓ mortality in comparison to aspirin | 60) |
| NSTEMI | Clopidogrel | ↓ Mortality in comparison to aspirin | 61) |
| STEMI | Clopidogrel 600 mg | ↓ Mortality in comparison to 300 mg | 62) |
| STEMI and NSTEMI | Clopidogrel, ticagrelor | Ticagrelor ↓ mortality | 63) |
| STEMI | Clopidogrel | ↓ Mortality in comparison to aspirin | 64) |
| STEMI | Clopidogrel 600 mg | ↓ IS in comparison to 300 mg | 65) |
| STEMI and NSTEMI | Clopidogrel | ↓ IS in comparison to aspirin | 66) |
| STEMI | Clopidogrel, ticagrelor, cangrelor, prasugrel | Only prasugrel ↓ mortality in comparison to with other P2Y12 antagonists | 67) |
| STEMI and NSTEMI | Ticagrelor, clopidogrel | No difference in mortality | 68) |
| STEMI and NSTEMI | Ticagrelor, clopidogrel | No difference in mortality | 69) |
| STEMI | Clopidogrel, ticagrelor, prasugrel | Ticagrelor and prasugrel ↓ MVO, ↓ IS | 70) |
| STEMI | Clopidogrel, ticagrelor | No difference in IS | 71) |
| STEMI | Clopidogrel, ticagrelor, prasugrel | No difference in adverse events | 72) |
| STEMI | Clopidogrel, ticagrelor, prasugrel | No difference in mortality | 73) |
| STEMI | Cangrelor, ticagrelor | No difference in MVO, IS | 74) |
| NSTEMI | Clopidogrel, ticagrelor, prasugrel | No difference in mortality | 75) |
| STEMI | Clopidogrel, ticagrelor | No difference in in mortality | 76) |
| STEMI and NSTEMI | Ticagrelor, prasugrel | No difference in the efficiency | 77) |
A retrospective study was performed by Serebruany et al.,67) which included 26,658 patients with STEMI who received clopidogrel, ticagrelor, cangrelor, and prasugrel. The 30-day mortality rate in the clopidogrel group was 2.76%, in the ticagrelor group was 2.6%, in the cangrelor group was 1.7% (p=0.19), in the prasugrel group was 1.75% (p=0.03). Thus, only prasugrel was comparable to cangrelor in reducing the mortality rate of patients with AMI. In a PLATO (n=18,621) study it was demonstrated the effectiveness of ticagrelor and cangrelor in patients with ACS do not differ in the rate of adverse events (death from vascular causes, myocardial infarction, stroke).68) Similar findings were reported by other investigators in a multicenter, double-blind, randomized study PHILO (n=801), which was performed in patients with ACS treated with ticagrelor or clopidogrel.69) A multicenter blind prospective Complete Versus Lesion-Only PRImary PCI Trial-CMR (CvLPRIT-CMR) study included patients with STEMI (n=203) who received clopidogrel (n=70), prasugrel or ticagrelor (n=133).70) Investigators found that infarct size was larger (p=0.013), and microvascular obstruction (p=0.022) is more common in patients who received clopidogrel. However, it should be noted that patients treated with clopidogrel were older and had a longer time interval between the onset of symptoms and revascularization. A study published by Yun et al.71) included patients with STEMI and PCI (n=188), who received ticagrelor or clopidogrel. Infarct size was determined by single-photon emission computed tomography (SPECT) with 99mTc-tetrofosmin and by the CK-MB and troponin T levels. Based on the SPECT findings, infarct size was the same in the clopidogrel and ticagrelor groups. The peak troponin T and CK-MB levels were lower in patients receiving clopidogrel. Differences in the troponin T level (p=0.029) were especially noticeable. The authors concluded that ticagrelor does not exceed clopidogrel in the infarct-limiting effect.
A European Ambulance Acute Coronary Syndrome Angiography (EUROMAX) study included patients with STEMI and PCI (n=1,919). It was compared the rate of adverse cardiovascular events after taking clopidogrel (n=784) or third-generation P2Y12 receptor inhibitors ticagrelor (n=516) and prasugrel (n=619).72) These groups did not differ in the rate of stent thrombosis or adverse events, but there was less frequent bleeding in the clopidogrel group (p=0.002). A retrospective study performed by Olier et al.,4) included more than 89,000 patients with STEMI, and who received P2Y12 receptor inhibitors (clopidogrel, prasugrel, or ticagrelor). Prasugrel was associated with lower mortality within 30 days (p=0.014) and 1 year (p=0.011) compared with clopidogrel. Differences in mortality of patients receiving ticagrelor or clopidogrel could not be detected. Comparative analysis of the use of clopidogrel, prasugrel, ticagrelor in patients with STEMI and PCI revealed differences between groups in fatal outcomes and the rate of adverse events during one year, as demonstrated by a Korea Acute Myocardial Infarction-National Institute of Health (KAMIR-NIH) study (n=9,355).73) In patients who received aspirin + clopidogrel, the rate of adverse events was 4.6% and was significantly higher (p<0.001) than in the aspirin + prasugrel group (2.6%) or the aspirin + ticagrelor group (2.3%). The increase was due to an increase in cardiac mortality (p<0.001). In patients who are receiving clopidogrel, the rate of bleeding (4.1%) was significantly lower (p<0.001) than in the prasugrel group (7.7%) and the ticagrelor group (9.0%). This indicated that after the use of clopidogrel, death is more likely to occur due to cardiac reasons, but bleeding is less likely to occur. In a study performed in China, it was included patients (n=2,001) with ACS.74) It was reported that fatal/life-threatening bleeding was observed in 0.8% of patients. In a randomized study, it was included patients (n=100) with STEMI and PCI.75) Patients received cangrelor or ticagrelor before PCI. The authors could not detect a difference between groups in microvascular resistance, coronary flow reserve, or infarct size detected by the peak troponin T level.75) Investigators tried to enhance the positive effect of P2Y12 receptor inhibitors using prehospital administration of these compounds. However, the prehospital use of P2Y12 receptor inhibitors promoted an increased risk of bleeding without the effect on mortality or major adverse cardiovascular events (MACE) in patients with STEMI, NSTEMI and PCI.76)77) In 2021, it was reported results of a retrospective study of STEMI patients from the CONDI-2/ERIC-PPCI (the combined CONDI-2 and ERIC-PPCI trial) trial.39) It was found that troponin release was decreased in STEMI patients with ticagrelor treatment compared to clopidogrel. MACE did not differ between clopidogrel, ticagrelor, or prasugrel.39) Treatment with ticagrelor reduced the incidence of heart failure within 12 months after STEMI.39) In the multicenter Registry of New Antiplatelets in patients with Myocardial Infarction (RENAMI) trial enrolled 4,424 ACS patients with PCI it was demonstrated that efficacy or safety of ticagrelor and prasugrel is identical.78)
The High Platelet Inhibition With Ticagrelor to Improve Left Ventricular Remodeling in Patients With ST Segment Elevation Myocardial Infarction (HEALING-AMI) study included patients with STEMI and PCI.79) Left ventricular remodeling index (LVRI) and the N-terminal pro-B-type natriuretic peptide level were assed 6 months after myocardial infarction. Ticagrelor reduced the 6-month level the N-terminal pro-B-type natriuretic peptide (p=0.028) level in comparison to clopidogrel. However, ticagrelor did not reduce LVRI compare to clopidogrel. Ticagrelor decreased left ventricular end-systolic volume index (p<0.001), clopidogrel had no effect. Thus, ticagrelor is more effective in preventing adverse post-infarction remodeling than clopidogrel.
Thus, clopidogrel reduces the rate of MACE in patients with acute coronary syndrome and STEMI. The best loading dose of clopidogrel is 600 mg. At this dose, clopidogrel reduces infarct size. Most studies suggest that ticagrelor does not exceed clopidogrel in the rate of adverse events or in limiting infarct size in patients with STEMI. Prasugrel compared with clopidogrel more effectively reduces mortality and the rate of adverse events in patients with AMI. The main side effect utilizing of P2Y12 inhibitors is bleeding.
CONCLUSIONS
It has been demonstrated that P2Y12 receptor antagonists cangrelor and ticagrelor have an infarct-reducing effect in vivo in animals, which is not associated with inhibition of platelet aggregation. Chronic administration of ticagrelor prevented adverse remodeling of the heart in animals. We hypothesize that S1P release plays an important role in the infarct-reducing effect of P2Y12 receptor antagonists. We cannot rule out the possibility of other cardioprotective molecules released from platelets under the impact of P2Y12 receptor antagonists. There are data that ticagrelor can activate the adenosine A3 receptor. However, there is no evince that endogenous adenosine or adenosine receptors are involved in the infarct-reducing effect of ticagrelor in vivo. It is unclear why ticagrelor and cangrelor can reduce infarct size in animals, but other P2Y12 receptor antagonists did not exhibit an infarct-reducing effect. However, clopidogrel reduced infarct size in clinical trial and had no effect in animals. These findings indicate that clinical data could be different from animal studies. P2Y12 receptor inhibitors reduce the rate of adverse events (death due to cardiovascular causes, myocardial infarction, stroke) in patients with acute coronary syndrome and patients with STEMI. P2Y12 receptor antagonists contribute to a decrease in infarct size in patients with AMI. Prasugrel was more effective in reducing mortality and the rate of adverse events in patients with AMI compared to clopidogrel. Ticagrelor can prevent adverse post-infarction myocardial remodeling. P2Y12 receptor antagonists can prevent heart failure in patients with AMI and PCI within 12 months after AMI, thereby it could be suggested that these drugs could prevent adverse post-infarction remodeling of the heart. A multicenter, placebo-controlled, long-term study is needed to confirm this hypothesis.
 XML Download
XML Download