

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Aortic stenosis (AS) is one of the most common valvular heart diseases and aortic valve replacement (AVR) is only treatment. Severe AS is generally defined as significant left ventricular (LV) outflow tract obstruction to cause symptoms (dyspnea, heart failure, chest pain, or syncope) and the criteria for severe AS has evolved over several decades.1)2)3)4)5)6) Although the severity of AS was initially assessed by hemodynamic cardiac catheterization, currently depends on 2-dimensional (2D) and Doppler echocardiography assessment in most cases. AS is considered severe when peak AV velocity is ≥4.0 m/s, mean pressure gradient (MG) ≥40 mmHg, or aortic valve area (AVA) ≤1.0 cm2. However, these parameters are frequently inconsistent with each other since they depend on individual’s body habitus, stroke volume (SV), and other coexisting conditions.7) A spectrum of the disease in patients with AS has been well recognized and LV response toward high afterload differs based on underlying myocardial condition.8) Wall thickness usually increases to offsets the pressure overload to keep the wall stress normal, however, less hypertrophy develops in some patients.9) Even in those with moderate severity of AS, some patients already have high wall stress and/or decreased contractility indicating decompensated LV.10) Pressure loss (energy loss) is an important part of significant AS and it becomes exponentially large as AVA is reduced to 30% which corresponds to an AVA of 1.2 cm2 if its normal size is 4.0 cm2.11)
Significant LV functional and hemodynamical changes can arise when AVA is moderately reduced, hence, there is an important need to revisit the definition of severe AS on the basis of the pathophysiologic event or clinical outcomes. Artificial intelligence (AI) may be able to play an important role in identification of AS in asymptomatic patients as well as in risk stratification. In this review, we will discuss a paradigm shift from “standardization” to “individualization” in defining the severity of AS and management strategy that would dramatically improve clinical outcomes and quality of life in patients with AS.
Go to : 
DEFINITION OF SEVERE AORTIC STENOSIS
Severe AS was initially defined as AVA of ≤0.75 cm2 with MG ≥50 mmHg until AVA of ≤1.0 cm2 was introduced as severe in the American College of Cardiology/American Heart Association valvular guidelines in 1998.1) In the subsequent 2006, 2014, 2017, and 2022 American and European guidelines,2)3)4)5)6) peak velocity ≥4 m/s or MG ≥40 mmHg became the main parameter to define severe AS irrespective of AVA as long as flow status is normal. When peak velocity or MG is lower than above values, AVA ≤1.0 cm2 is defined as severe AS. The higher aortic valve (AV) gradient is associated with a higher clinical event rate,12)13) therefore, the current diagnostic approach has a high specificity for identifying patients with severe AS but is less sensitive. Since all AS parameters assessed by Doppler echocardiography are flow-dependent, flow status is a key when assessing AS severity. However, how to manage the differences in flow status has been difficult, especially between men and women as well as among different body habitus. There are hemodynamic and anatomical differences between sexes; women normally have lower SV than men and thus the AV gradient is lower in women for a given AVA (Figure 1).14) Obese patients have higher SV than those with normal weight due to excess adipose tissue.15) To correct these differences, the current guidelines employ body surface area (BSA); indexed SV (SVI) ≤35 mL/m2 is for defining low-flow AS, and indexed AVA (AVAi) ≤0.6 cm2/m2 is for severe AS.4)6) However, AV gradient has a better correlation with SV compared to SVI14) and a poor correlation between cardiac output and BSA has been demonstrated.16) Therefore, it is not clear whether such an adjustment by BSA is relevant in defining the severity of AS. Instead of SV or SVI, the prognostic utility of flow rate (ratio of SV to LV ejection time) has been introduced in patients with AS,17) but further investigation is still required. AVAi of 0.6 cm2/m2 was proposed as a cut-off value for severe AS in 1967 as it corresponded with significant LV stroke work loss.18) In their study, infants were involved in the analysis, leading to a wide range of BSA. AVAi identifies patients with a milder degree of the disease without improving the predictive accuracy for AV related events.19) In regard to the body habitus, the prevalence of obesity has increased not only in the US but also in other countries. For example, the overall obesity rate in Korea rose to 38.3% in 2020 when obesity was defined as having a body mass index (BMI) ≥25 kg/m2.20) Although “obesity paradox” (obesity is unexpectedly associated with better or equal survival to normal weight patients) has been reported in patients with AS similar to those with heart failure, higher flow status with higher AV gradient is common in obese patients thus such a comparison is tricky when the same criteria for AS severity is applied.21) This is also the case for patients with a prosthesis-patient mismatch (PPM); PPM does not impact on survival outcomes in obese patients, thus the indexed effective orifice area (EOAi) cut-off for PPM differs based on BMI.22) BMI is commonly used to classify overweight and obesity, but, it has an only evidence category C for assessing body habitus as described in the US National Institutes of Health guidelines.23) The application of BSA and BMI in patients with AS requires further investigations.
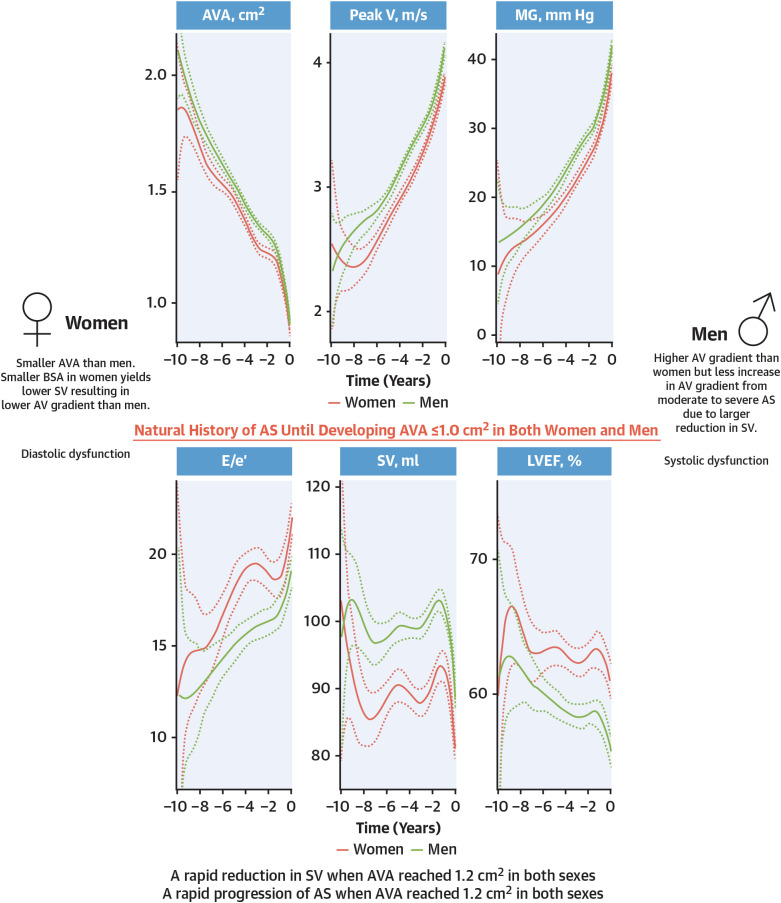 | Figure 1Longitudinal change of AS and LV hemodynamics between sexes. Longitudinal analysis using splines within mixed linear models is shown with mean and 95% confidence interval for AS and LV hemodynamics until developing AVA ≤1.0 cm2 in a total of 927 patients.AS = aortic stenosis; AVA= aortic valve area; LV = left ventricular; LVEF = left ventricular ejection fraction; MG = mean pressure gradient; peak V = peak velocity; SV = stroke volume.
With permission from Ito S, Miranda WR, Nkomo VT, Lewis BR, Oh JK. Sex differences in LV remodeling and hemodynamics in aortic stenosis: sex-specific criteria for severe stenosis? JACC Cardiovasc Imaging 2022;15:1175-89.14)
|
It is important to acknowledge that there is a significant reduction in the SV when AS transitions from moderate to severe AS when assessed by either cardiac catheter or Doppler echocardiography.14)24)25) A precipitous reduction in SV is observed when AVA becomes approximately 1.2 cm2 in progressive AS (Figure 1).14)26) A large data from Australia also shows that patients with severe AS have lower SVI compared to those with moderate AS (moderate AS: 49.8±14.6, severe AS-high gradient: 41.9±13.9, severe AS-low gradient: 29.0±10.0 mL/m2).27) Patients with low-flow low-gradient severe AS are known to have experienced a significant SV reduction.28) Reduction in SV is associated with less increase in AV gradient as AS progresses. In this context, AVA may have a better association with the pathophysiology of AS compared to AV gradient since SV is incorporated into the continuity equation. In fact, the risk profile for mortality differs between AV gradient and AVA.29) The importance of AVA could be more emphasized when assessing AS severity.
Go to :
RISK ASSESSMENT
When defining severe AS, it is important to evaluate overall risk which results from combination of underlying myocardial dysfunction and AV hemodynamics. Currently, the risk assessment is primarily dependent on evaluating symptomatic status. Patients with symptomatic severe AS is class I indication for AVR as in the guidelines.4)6) Symptomatic patients are at high risk and averaged survival according to symptoms originally reported by Ross and Braunwald30) in 1968 is as follows: chest pain 5 years, syncope 3 years, and dyspnea 2 years. These findings have been a huge impact on our patients’ management strategy, however, it should be acknowledged that their data is a retrospective observation from 10 relatively younger patients than contemporary AS patients with symptoms.30) Furthermore, the majority of contemporary patients with AS are elderly with limited activity, and symptom assessment is often difficult. Objective parameters are required for the risk assessment. Park et al.31) demonstrated that each symptomatic status in AS is associated with Doppler echocardiography findings. They showed that a smaller LV cavity and reduced SV are associated with syncope and advanced diastolic dysfunction (e.g., higher E/e’) for dyspnea. E/e’ has been shown to be well correlated with pulmonary arterial wedge pressure and may play an important role in the risk assessment.32)33)34) In patients with severe AS, decreased left ventricular ejection fraction (LVEF; <50% or 50–60%) is associated with intrinsic cardiomyopathy and has a poor prognosis compared to LVEF ≥60%.26)35)36)37) LV global longitudinal strain (GLS) assessed using 2D speckle-tracking imaging is also reported to have prognostic value in patients with severe AS.38)39)40)41) Even in patients with moderate AS, impaired LVEF, E/e’, and GLS have been associated with adverse survival outcomes.42)43) Cardiac magnet resonance (CMR) plays an important role in risk stratification; diffuse interstitial fibrosis which is potentially reversible can be quantified with CMR T1 mapping44)45) and irreversible fibrosis is identified using late gadolinium enhancement CMR.46)47) However, because CMR is not always clinically indicated in patients with AS, histological change in the LV especially at the subclinical level amongst patients with AS is sometimes difficult to evaluate. AI incorporating multiple clinical, imaging, and blood test result may be helpful for identifying these patients in the future as discussed below. In patients with AS, LV response differs based on underlying cardiac conditions.8) Together with multiple comorbid conditions in the elderly, there is a necessity of shifting from “standardization” to “individualization” in diagnosis and prognostication of severe AS to provide the better management.
Go to :
AORTIC VALVE REPLACEMENT
The first valve replacement in a human was performed in 1962. Since then, various types of prosthetic valves have been developed.48) In the last 15 years, the efficacy and safety of transcatheter aortic valve replacement (TAVR) have been studied and established in the extreme-, high-, intermediate-, and low-risk patients with severe AS.49)50)51)52)53)54)55) In the current guidelines, a benefit of TAVR and surgical AVR (SAVR) is described in patients with 65–80 years for whom bioprosthetic valve is preferred, and a preference of TAVR in elderly patients (>80 years) is supported if patients have high or prohibitive surgical risk with adequate quality of life and life expectancy.4) In the US, TAVR volume has been increasing every year exceeding SAVR in 2019.56) The most widely used TAVR bioprostheses are intra-annular balloon-expandable valves (SAPIENTM family; Edwards Lifesciences LLC, Irvine, CA, USA) and supra-annular self-expandable valves (CoreValve®/EvolutTM family; Medtronic Inc, MN, USA). Their hemodynamical and anatomical differences assessed by Doppler echocardiography are summarized by Hahn et al.57) They reported that larger EOA and lower MG in self-expandable valves compared to balloon-expandable valves when comparing the same size valves. These findings are also observed in patients with small aortic annuls in a retrospective study,58) and the differences are currently being investigated prospectively (SMART trial; NCT04722250). On the other hand, as summarized in Table 165) the risk of conduction disturbance such as a new onset of left bundle branch block and a necessity of pacemaker implantation after TAVR are more frequent in the self-expandable valve.65)66)67)68)69) Impact of pacemaker implantation on survival outcomes following TAVR is yet controversial, however, reduction in LV function induced by a right ventricle-paced rhythm has been well documented.68) The pacemaker implantation rate may decrease with the improvement of implantation technique (e.g., cusp overlap technique),66)67) but coronary protection is also important when positioning a TAVR valve. Significant paravalvular regurgitation (≥moderate) has been shown to be associated with poor clinical outcomes70)71)72)73) and even a mild degree of paravalvular regurgitation has been demonstrated to be the case.59) However, these findings came from early studies and the most recent TAVR valves have very low incidents of paravalvular regurgitation (0–2.0%, Table 1). An adverse impact of paravalvular regurgitation on clinical outcomes is likely to reduce.
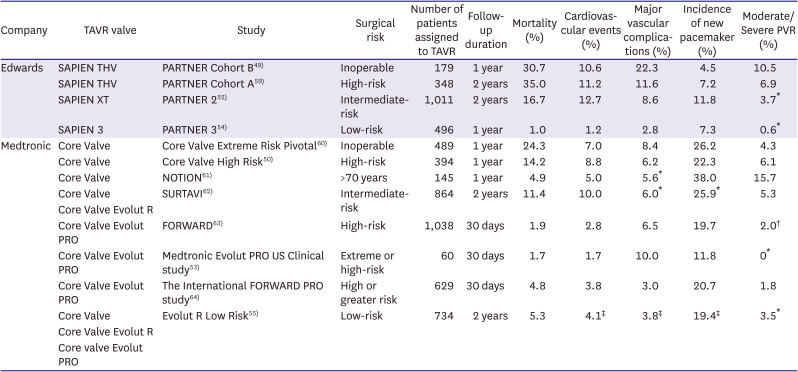
Table 1
The summary for TAVR trials
| Company | TAVR valve | Study | Surgical risk | Number of patients assigned to TAVR | Follow-up duration | Mortality (%) | Cardiovascular events (%) | Major vascular complications (%) | Incidence of new pacemaker (%) | Moderate/Severe PVR (%) |
|---|---|---|---|---|---|---|---|---|---|---|
| Edwards | SAPIEN THV | PARTNER Cohort B49) | Inoperable | 179 | 1 year | 30.7 | 10.6 | 22.3 | 4.5 | 10.5 |
| SAPIEN THV | PARTNER Cohort A59) | High-risk | 348 | 2 years | 35.0 | 11.2 | 11.6 | 7.2 | 6.9 | |
| SAPIEN XT | PARTNER 252) | Intermediate-risk | 1,011 | 2 years | 16.7 | 12.7 | 8.6 | 11.8 | 3.7* | |
| SAPIEN 3 | PARTNER 354) | Low-risk | 496 | 1 year | 1.0 | 1.2 | 2.8 | 7.3 | 0.6* | |
| Medtronic | Core Valve | Core Valve Extreme Risk Pivotal60) | Inoperable | 489 | 1 year | 24.3 | 7.0 | 8.4 | 26.2 | 4.3 |
| Core Valve | Core Valve High Risk50) | High-risk | 394 | 1 year | 14.2 | 8.8 | 6.2 | 22.3 | 6.1 | |
| Core Valve | NOTION61) | >70 years | 145 | 1 year | 4.9 | 5.0 | 5.6* | 38.0 | 15.7 | |
| Core Valve | SURTAVI62) | Intermediate-risk | 864 | 2 years | 11.4 | 10.0 | 6.0* | 25.9* | 5.3 | |
| Core Valve Evolut R | ||||||||||
| Core Valve Evolut PRO | FORWARD63) | High-risk | 1,038 | 30 days | 1.9 | 2.8 | 6.5 | 19.7 | 2.0† | |
| Core Valve Evolut PRO | Medtronic Evolut PRO US Clinical study53) | Extreme or high-risk | 60 | 30 days | 1.7 | 1.7 | 10.0 | 11.8 | 0* | |
| Core Valve Evolut PRO | The International FORWARD PRO study64) | High or greater risk | 629 | 30 days | 4.8 | 3.8 | 3.0 | 20.7 | 1.8 | |
| Core Valve | Evolut R Low Risk55) | Low-risk | 734 | 2 years | 5.3 | 4.1‡ | 3.8‡ | 19.4‡ | 3.5* | |
| Core Valve Evolut R | ||||||||||
| Core valve Evolut PRO |
TAVR = transcatheter aortic valve replacement.
The incidence is reported based on the follow-up duration of each study, but the following are the exceptions; *Results at 30 days; †Results at discharge; ‡Results at one year.
With permission from Bourantas CV, Modolo R, Baumbach A, et al. The evolution of device technology in transcatheter aortic valve implantation. EuroIntervention 2019;14:e1826-33.65)
![]()
Given the reports of high mortality rates in patients with moderate AS,27)42) together with the establishment of the TAVR procedure, there has been a growing interest in applying TAVR to patients with moderate AS. Several clinical trials are currently ongoing to investigate the efficacy of TAVR (TAVR UNLOAD: NCT02661451, PROGRESS; NCT04889872, EXPAND II; NCT05149755). In these trials, symptomatic patients with moderate AS with age ≥65 years (TAVR UNLOAD; ≥18 years) and cardiac dysfunction or a history of congestive heart failure are eligible. Impaired E/e’ and GLS, and elevated NT-proBNP are also used for identifying candidates.26)42)43)74) At the completion of these trials, we should be able to assess whether an earlier TAVR can benefit patients with the underlying myocardial disease. In the retrospective studies, AVR is reported to reduce the risk of mortality in patients with moderate AS and reduced LVEF.75)76)77) Of note, LV hemodynamic deterioration has started when AS is becoming moderate to severe as currently defined in a considerable proportion of patients as we discussed above (Figure 1). Patients with moderate AS plus moderate aortic regurgitation are also known to be at high risk, they have comparable clinical outcomes to those with severe AS.78) Besides these trials, identifying those who are potentially decent candidates for earlier AVR requires further investigations. In the process of applying TAVR to less severe, younger, and lower-risk populations with longer life expectancy, it is also important to better appraise the long-term durability characteristics of TAVR prostheses so-called structural valvular dysfunction (SVD) or hemodynamic valve dysfunction (HVD). In surgical bioprosthesis, SVD starts to occur especially >5 years after implantation, and its incidence increases substantially at 10 years, and even more at 15 years.79) Furthermore, SVD in surgical bioprosthesis usually occurs earlier in younger patients.75) Similar changes may happen in the TAVR valves. Meta-analysis comparing valve durability with a follow-up range from 1 to 6 years is available although the definition of SVD differs between referenced studies.81) A total of ten randomized control trials were involved in the analysis (PARTNER 1A, PARTNER 2A, PARTNER 3, US CoreValve, SURTAVI, NOTION, Evolut, CHOICE, SOLVE-TAVI, and SVOPE I) for comparing balloon-expandable TAVR (n=2,562), self-expandable TAVR (n=2,863), and SAVR bioprosthesis (n=3,963). At 1-year follow-up, a change in MG is similar between balloon-expandable TAVR (baseline 45.75 to 1-year 10.52 mmHg), self-expandable TAVR (44.47 to 8.63 mmHg), and SAVR bioprosthesis (46.38 to 11.29 mmHg).81) At 5-year, a significant increase in MG was observed in balloon-expandable valve (at 5 year: 11.61 mmHg) compared to self-expandable TAVR (7.42 mmHg) and SAVR (11.33 mmHg) but the change was minimal in all arms. SVD was less frequent in self-expandable TAVR compared to balloon-expandable TAVR and SAVR (hazard ratio [HR], 0.14, 95% confidence interval [CI], 0.07–0.27; HR, 0.34, 95% CI, 0.24–0.47, respectively). Incidence of moderate-severe AR and reintervention following AVR was more frequent in both balloon-expandable TAVR (HR, 4.21, 95% CI, 2.40–7.39; HR, 2.22, 95% CI, 1.16–4.26, respectively) and self-expandable TAVR (HR, 7.51, 95% CI, 3.89–14.5; HR, 2.86, 95% CI, 1.59–5.13, respectively) compared to SAVR, although the reasons for the necessity of re-intervention in TAVR have not been clarified in the manuscript. Pibarot et al.82) have reported 5-year rate of SVD in balloon-expandable TAVR based on data from the PARTNER-2 trial (SAPIEN XT) and the SAPIEN 3 registry (SAPIEN 3). The second-generation SAPIEN XT balloon-expandable valve has a higher 5-year rate of SVD (9.5%) compared with SAVR (3.5%), whereas the third-generation SAPIEN 3 has a rate of SVD (3.9%) that was not different from SAVR.82) These reports are clinically important, however, without applying the same criteria for SVD to all studies, it cannot be conclusive. SVD has been described and defined in several approaches; its definition has been historically based on the requirement of valve reintervention or prosthetic valve-related death thus resulting in underestimation of the actual incidence. Recently, specific criteria for SVD/HVD has been proposed by the European society and the VARC 3 (valve academic research consortium 3).83)84) However, it remains still difficult to define it since it is necessary to differentiate 1) whether the prosthetic valve dysfunction is a permanent structural deterioration, 2) transient dysfunction (e.g., thrombosis), or 3) non-structural dysfunction (e.g., PPM). Despite of the difficulty in SVD/HVD definition, these results indicate that the durability of TAVR valves is at least as good as that of SAVR up to 5 years.
The importance of lifetime management of patients with AS has been becoming ever more emphasized in the process of applying earlier AVR in younger patients. The decision-making process for lifetime management may include the patients’ biological background (e.g., age, comorbid conditions), available valve size, risk of future cardiac surgery, and the ability to perform valve in valve procedure.
Go to :
MEDICAL THERAPY: PREVENT THE AS PROGRESSION
Calcific AS is a progressive active disease and the only effective treatment is replacing the AV, thus, we usually watchful-wait until AS becomes symptomatically severe. There has been hope and huge enthusiasm to find effective medical therapy to prevent the progression of the disease, but there is no such drug available currently. Identifying a therapeutic target in the pathophysiology of AS is crucial and has been investigated.85)86) Following endothelial damage which initiates the AV injury, the lipids such as lipoprotein (a) and oxidized low-density lipoprotein cholesterol infiltrate the valve (Figure 2).85) Progression of this process establishes an inflammatory response within the valve that is characterized predominantly by infiltration of macrophages but also involves T lymphocytes and mast cells.85)87) These processes trigger the very early stage of valve calcification. Valvular interstitial cells (VICs), residing in the interstitial layer of the AV, are subsequently induced to undergo osteogenic differentiation via several different mechanisms, including the binding of receptor activator of nuclear κB ligand (RANKL) to RANK.85)88) RANKL binding stimulates osteogenic differentiation of VICs into osteoblasts, leading to the formation of calcific nodules and expression of alkaline phosphatase and osteocalcin.85)89) Similar to skeletal bone formation, the initial deposition of collagen matrix provides a scaffold upon which progressive calcification, and further calcification develops as described in Figure 2.85)
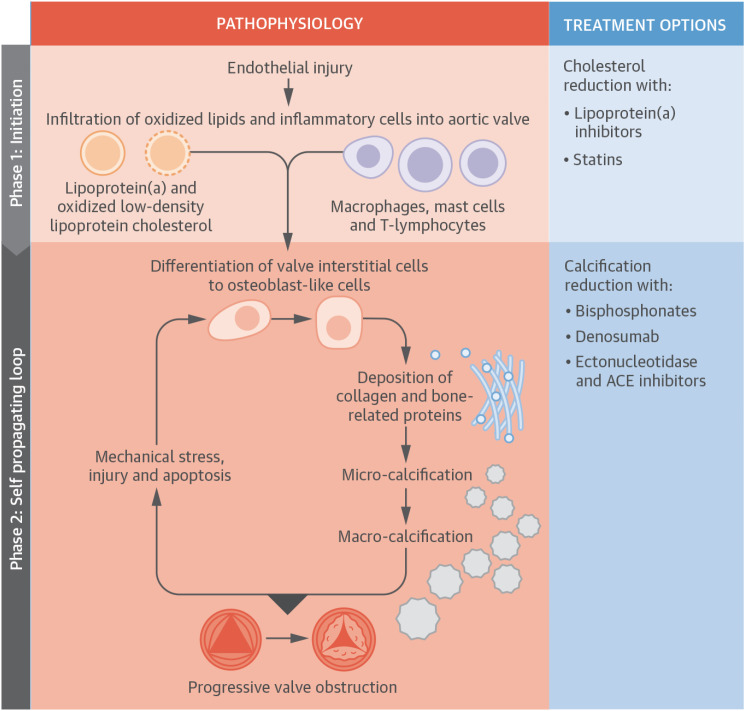 | Figure 2The pathophysiology of AS. The pathophysiology of AS is summarized. Initiation phase: endothelial injury facilitates the infiltration of oxidized lipids and inflammatory cells into the valve and the release of proinflammatory mediators. These trigger the very early stages of valve calcification. The propagation phase: these proinflammatory processes subsequently induce VICs to undergo osteogenic differentiation via several different mechanisms, including the binding of receptor activator of nuclear kappa B ligand to receptor activator of nuclear kappa B. Differentiated cells within the aortic valve first lay down a collagen matrix and other bone-related proteins causing valvular thickening and stiffening before producing calcium. Additionally, apoptotic remnants of some VICs and inflammatory cells create a nidus for apoptosis-mediated calcification. Calcification of the valve induces compliance mismatch, resulting in increased mechanical stress and injury. This results in further calcification via osteogenic differentiation and apoptosis. Hence, a self-perpetuating cycle of calcification, valve injury, apoptosis, and osteogenic activation is established that drives the propagation phase of the disease.ACE = angiotensin-converting enzyme; AS = aortic stenosis; VIC = valvular interstitial cell.
With permission from Pawade TA, Newby DE, Dweck MR. Calcification in aortic stenosis: the skeleton key. J Am Coll Cardiol 2015;66:561-77.85)
|
Based on the mechanism of the AV calcification, the pharmacological targets have been tested in several clinical trials. The efficacy of statin therapy was tested in 3 randomized control trials using atorvastatin, rosuvastatin, and simvastatin plus ezetimibe, but all of them failed to halt the progression of calcific AS or induce its regression.90)91)92) Because angiotensin-converting enzyme (ACE) is upregulated in calcific AV disease, the efficacy of ACE inhibitor (ramipril) has been tested and shown the slower progression of the AV stenosis compared to the placebo group although it was not statistically significant.93) Neither RANKL inhibitor nor bisphosphonate affect the progression of AV calcification.89) The post hoc analysis from the FOURIER trial, evolocumab (proprotein convertase subtilisin/kexin type 9) inhibitor is shown to potentially reduce AS events94) and prospective trial is currently ongoing (EPISODE trial: NCT04968509). A pilot trial investigating the effectiveness of Lipoprotein (a) lowering therapy using niacin on the development of AS is also currently active (EAVaLL trial, NCT02109614). Recently, Dr. Song’s group from South Korea reported that endothelial dysfunction in the AV leads to increased expression of dipeptidyl peptidase-4 (DPP-4), which induces the degradation of insulin-like growth factor-1 and subsequent osteogenic differentiation of VICs in vitro.95)96) Their result suggest that DPP-4 could serve as a potential therapeutic target to inhibit calcific AS progression. They subsequently reported that specific favorable DPP-4-inhibitorsmay delay the AS progression rate using retrospective human data.96) Based on these positive findings, clinical studies investigating the efficacy of a DPP-4 inhibitor (Evogliptin) are currently active in South Korea (DIP-CAVD: NCT04055883) and in the US (EVOID-AS trial: NCT05143177).
Because the therapeutic target of these potential medications is the mild or moderate AS population, identification of patients with an earlier stage of the disease is critical. The importance of earlier detection of patients with AS using AI models will be discussed in the next section.
Go to :
THE ROLE OF ARTIFICIAL INTELLIGENCE
As described above, earlier treatment by TAVR or medical therapy might be available for patients with AS in the coming future, therefore, earlier detection of patients with AS will be a key. As a screening tool for identifying patients with AS regardless of symptomatic status, Kwon et al.97) have developed an AI-enabled electrocardiography (AI-ECG) model from the Korean population to identify patients with moderate or severe AS. The model is well designed and has excellent performance with a high area under the curve (AUC) of 0.88. Our group also developed the AI-ECG model to identify patients with moderate or severe AS from the US population with high performance at an AUC of 0.85.98) The AI model using chest radiographs has been also built for detecting patients with AS from the Japanese population with an AUC of 0.83.99) The performance of these models is excellent, however, its most effective application to clinical practice has not been well ironed out. Although the number of patients with AS has been increasing, a report from the US population in 2006 showed that the prevalence of patients with moderate and severe AS was low at 0.4% (age ≥18 years) and 2.8% even in those with age ≥75 years.100) Based on data from 7 studies, a pooled prevalence of severe AS was shown to be 3.4% in the elderly (age >75 years).101) Because of the low prevalence of the disease in the population, low positive predictive value and high negative predictive value are expected for these models. Consistently, the model from South Korea shows a positive predictive value low at 12.1% and a high negative predictive value of 99.4%, respectively.97) Similarly, our AI-ECG model from the US has positive and negative predictive values of 10.5% and 98.9%, respectively.98) For the radiograph-AI model from the Japanese population, positive and negative predictive values were 18.0% and 97.0%, respectively.99) These models thus have an excellent ability for excluding patients with AS, however, there may be a concern for low positive predictive value because we may need to perform unnecessary echocardiography exams in individuals with positive results. Since the early detection of patients with AS is becoming a key for applying earlier intervention, it should be our mission to clarify how to apply these models effectively to the community as well as clinical practice.
Another expected role for AI is disease phenotyping including risk stratification for providing patient-tailored care. Because AS is a wide spectrum of disease, it is necessary to provide the appropriate treatment to the right patient at the right time. It has been reported that survival outcomes get worse as cardiac damage extended from LV to LA and further involved pulmonary vasculature and right ventricle amongst patients with severe AS identified from the PARTNER 2 cohort.102) They classified the groups based on the cardiac function using echocardiography data without employing AI. Kwak et al.103) investigated whether cluster analysis identifies subgroups with different prognostic significances in AS. In their study, they successfully identified 3 distinct groups with different causes of death regardless of the disease severity using objective parameters characterizing the heterogeneity of patients with AS. Dr. Sengupta’s group actively works on topological data analysis which employs a machine-learning framework to cluster the patient similarity network for phenotypic recognition of the pattern of LV responses in patients with AS.104) The Artificial Intelligence for Aortic Stenosis at Risk International Consortium developed machine-learning models for augmenting the echocardiographic grading of AS severity.105) After generating low- and high-severity disease groups based on echocardiographic data using topological data analysis, a machine-learning-based ensemble classifier was trained to identify these groups of patients. The accuracy of the classifier was high, and it successfully classified the AS severity and stratified the risk for AVR/death even in patients with discordant echocardiography AS parameters as well as those with non-severe AS evaluated by echocardiography.
There is a brilliant potential benefit in applying AI in medicine to improve our patient management, but any models are complex and not interpretable to humans (so-called “black box”). We cannot simply apply an AI model to the clinic without investigating its decision-making process especially when we want to apply it to define AVR timing. Our AI group at Mayo Clinic recently developed a setup to understand which features of the ECG were used by human intelligence (medical expert) and by an AI model.106) The “black-box” problem may be potentially overcome.
Go to :
THE FUTURE DIRECTION
The most recent development in our diagnostic and treatment options for patients with AS are discussed in this review. Identification of the patients with AS at increased risk will require not only valvular hemodynamics but also assessment of underlying myocardial function using multi-modality imaging. Several clinical trials are underway to determine optimal timing of AVR, to find a medical therapy to reduce the progression of AS, and to enable AI to identify asymptomatic patients with AS. Time will come when we are able to identify asymptomatic patients at an early stage of AS, to reduce its progression by a medical therapy, and to determine the optimal timing for AVR if necessary in a much smaller number of patients compared to the current practice.
Go to :
 XML Download
XML Download