

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Most cardiologists have treated dying patients. However, more than half of clinicians answered no to the question, “Have you ever been involved in end-of-life (EOL) care?”1)
Heart failure (HF) is an important chronic condition because it carries a high socioeconomic burden and poor prognosis.2)3) As treatments improve for major cardiovascular diseases, including myocardial infarction, valvular heart disease, and cardiomyopathies, the prevalence of HF is continuously increasing.3)4)5)6) Many patients with HF, especially those with end-stage HF (ESHF), suffer from uncontrolled symptoms despite optimal guideline-directed medical treatment (GDMT) which are mainly focused on improving survival and reducing HF readmissions.7)8) Though the number of patients who might need EOL care has been increasing gradually as the medical and device therapy for HF have improved, the debilitating symptoms of those patients and their need for a holistic approach to EOL have only recently begun to be recognized by clinicians.
Although several studies provide palliative-care guidance for physicians treating ESHF patients,9)10)11) and previous research reported that EOL care improved both clinical outcomes and patient quality of life (QOL),12)13) most patients with ESHF do not receive EOL care.7)14) In this review, we discuss the concept and key components of EOL care and provide clinical guidance for physicians caring for patients with ESHF.
Go to : 
DEFINITION OF END-OF-LIFE AND CONCEPT OF PALLIATIVE CARE
Advanced HF is described as a clinical status with severe and persistent symptoms, severe cardiac dysfunction, and severe impairment of exercise capacity that is characterized by episodes of pulmonary congestion, low cardiac output, or malignant arrhythmia despite optimal guideline-directed treatment.15) The clinical delineation between advanced HF and ESHF is often difficult, but ESHF is generally included in advanced HF and is usually perceived to be a more advanced condition than advanced HF.16) Patients with ESHF generally do not respond or are not eligible for advanced HF treatments such as a ventricular assist device or heart transplantation. EOL is also not clearly defined, but patients who transition to ESHF are usually thought to have less than 6 months to live and are thus considered to be at the EOL.17)18)
The World Health Organization defines palliative care as an “approach that improves the QOL of patients and their families who are facing problems associated with life-threatening illness” and asserts that only 14% of the people who need palliative care currently receive it.14) Recent HF guidelines say that palliative and supportive care should be integrated into the routine care of all patients with HF.10)11) Palliative care is not synonymous with hospice, nor is it synonymous with EOL care. Hospice is a formal system of interdisciplinary care that provides palliative care services to the dying in the last months of life.19) EOL care comprises continuous treatment for underlying HF, palliative care to control symptoms and improve QOL, and a shared decision-making process to delineate an advance care plan (ACP). The key components of EOL care are listed in Table 1.10)11)20)

Go to :
WHEN SHOULD END-OF-LIFE CARE BE CONSIDERED?
In the past, the timing of treatment for curative and palliative care was relatively clearly distinguished. Curative treatment was converted to palliative care to reduce the symptom burden when little or no further therapeutic effect from curative treatment was expected due to disease progression or exacerbation. However, that understanding is changing. Now, palliative care is deemed appropriate early in the disease course, in conjunction with disease-modifying treatments intended to cure or control the disease, to reduce symptoms and improve QOL.10)20) As HF progresses, the proportion of treatment intended or expected to increase the survival gradually decreases, and the importance of palliative treatment and supportive care increases, becoming the predominant treatment as death approaches. It is important to recognize that the transition to the end-stage is a process, not a specific point in time.
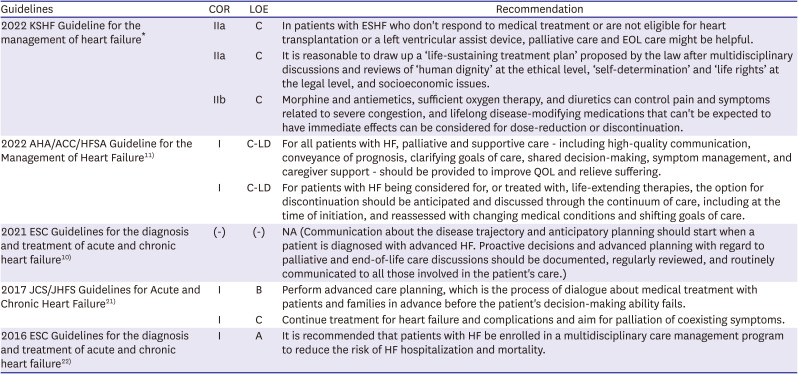
Recent HF guidelines highlight more clinical considerations for palliative care, including at the EOL, than previous editions (Table 2). The 2021 European HF guideline suggests that EOL care should be considered in patients with 1) progressive functional decline (physical and mental) and dependence in most activities of daily living, 2) severe HF symptoms with poor QOL despite optimal pharmacological and non-pharmacological therapies, 3) frequent admissions to a hospital or other serious episodes of decompensation despite optimal treatment, 4) unsuitable conditions for heart transplantation or mechanical circulatory support, 5) cardiac cachexia, 6) clinically judged nearness to the EOL.10) However, in real clinical practice, unlike with cancer, it is very difficult to predict the last days of an HF patient, and thus it is also very difficult to discuss care plans in advance and prepare for EOL care.23)24) Unexpected sudden cardiac death can occur at any time during the course of HF, and acute decompensation and clinical deterioration can occur even in stabilized chronic HF patients under GDMT. Each patient has a very diverse disease course, and there is considerable uncertainty in predicting the prognosis (Figure 1).
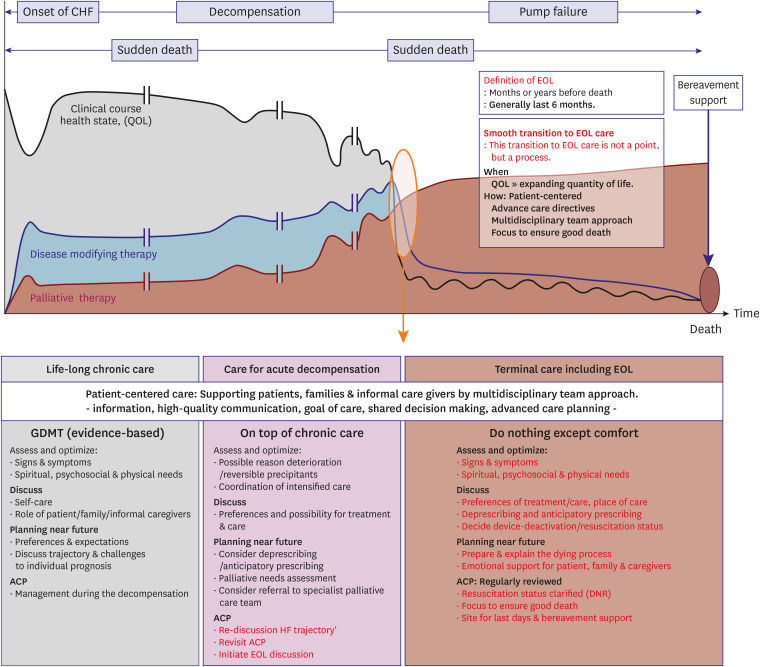 | Figure 1Integrating palliative care and end-of-life care across heart failure disease trajectory.9)11) Integrating palliative care, including EOL care, into heart failure management across the whole disease trajectory is clearly challenging. Ideally, it should include symptom control for QOL, ACP, family and informal caregiver support (including bereavement), and trying to ensure a good death. This figure shows 1) transition timing for EOL care and 2) a method for patient-centered EOL care through a multidisciplinary team approach.ACP = advanced care planning; CHF = congestive heart failure; EOL = end of life; GDMT = guideline-derived medical treatment; QOL = quality of life.
|
Table 2
Recommendations for palliative care, shared decision-making, and end-of-life in heart failure guidelines
| Guidelines | COR | LOE | Recommendation |
|---|---|---|---|
| 2022 KSHF Guideline for the management of heart failure* | IIa | C | In patients with ESHF who don't respond to medical treatment or are not eligible for heart transplantation or a left ventricular assist device, palliative care and EOL care might be helpful. |
| IIa | C | It is reasonable to draw up a ‘life-sustaining treatment plan’ proposed by the law after multidisciplinary discussions and reviews of ‘human dignity’ at the ethical level, ‘self-determination’ and ‘life rights’ at the legal level, and socioeconomic issues. | |
| IIb | C | Morphine and antiemetics, sufficient oxygen therapy, and diuretics can control pain and symptoms related to severe congestion, and lifelong disease-modifying medications that can't be expected to have immediate effects can be considered for dose-reduction or discontinuation. | |
| 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure11) | I | C-LD | For all patients with HF, palliative and supportive care - including high-quality communication, conveyance of prognosis, clarifying goals of care, shared decision-making, symptom management, and caregiver support - should be provided to improve QOL and relieve suffering. |
| I | C-LD | For patients with HF being considered for, or treated with, life-extending therapies, the option for discontinuation should be anticipated and discussed through the continuum of care, including at the time of initiation, and reassessed with changing medical conditions and shifting goals of care. | |
| 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure10) | (-) | (-) | NA (Communication about the disease trajectory and anticipatory planning should start when a patient is diagnosed with advanced HF. Proactive decisions and advanced planning with regard to palliative and end-of-life care discussions should be documented, regularly reviewed, and routinely communicated to all those involved in the patient's care.) |
| 2017 JCS/JHFS Guidelines for Acute and Chronic Heart Failure21) | I | B | Perform advanced care planning, which is the process of dialogue about medical treatment with patients and families in advance before the patient's decision-making ability fails. |
| I | C | Continue treatment for heart failure and complications and aim for palliation of coexisting symptoms. | |
| 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure22) | I | A | It is recommended that patients with HF be enrolled in a multidisciplinary care management program to reduce the risk of HF hospitalization and mortality. |
ACC = American College of Cardiology Foundation; AHA = American Heart Association; COR = class of recommendation; EOL = end of life; ESC = European Society of Cardiology; HFSA = Heart Failure Society of America; JCS = Japanese Circulation Society; JHFS = Japanese Heart Failure Society; KSHF = Korean Society of Heart Failure; LOE = level of evidence; NA = Not available; QOL = quality of life.
*The 2022 KSHF guideline for the management of heart failure was published in July 2022 in Korean.
![]()
Though several scoring systems for predicting HF prognoses have been proposed, including the Meta-analysis Global Group in Chronic Heart Failure score,25) Seattle Heart Failure Model,26) and Gruppo Italiano per lo Studio della Streptochinasi nell'Infarto Miocardico-Heart Failure score,27) those models generally predict survival times and help to identify patients who could benefit from invasive or complex procedures such as mechanical circulatory support or heart transplantation. Validated prognostic tools28)29) to identify patients who could benefit from palliative care have been suggested, but they are designed for cancer patients, not HF patients, and they are not routinely used in clinical practice because of their perceived complexity or inconvenience. Recently, the Surprise Question (SQ; “Would you be surprised if this patient died within the next 6–12 months?”) was suggested as a reasonable alternative to a standard prognostic predictor.30)31)
Given the unpredictable disease trajectory and challenging prognostication of HF, communication about disease course and ACPs should be started when ESHF is diagnosed (Figure 1). Early discussions about palliative care can reduce unwanted hospital admissions and unnecessary use of health services.
Go to :
THE ADVANCE CARE PLAN AND SHARED DECISION-MAKING PROCESS
The ACP is the mainstay of EOL care. All decisions needed at the EOL will be made in accordance with the ACP, a treatment plan used when the patient is unable to make their own decisions at the EOL. All care decisions should be based on the ACP.
Until recently, healthcare providers thought that the main issues to be addressed in an ACP were whether or not the patient consented to invasive procedures and whether they wanted to be resuscitated. The paradigm of EOL care in HF is now shifting to a value-based model that requires a comprehensive discussion of all aspects of the patient.17) Factors that should be included in the ACP are listed in Table 3.
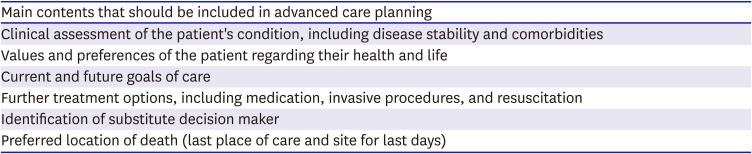
Table 3
Main content for advanced care planning
![]()
The discussions in which the ACP is written should be patient-centered and involve the physician, patient, and family members (caregivers). Clinicians should inform the family about the patient’s current condition and treatment, expected prognosis, further treatment options (including invasive procedures) and their probable outcomes, and problems likely to be faced in the near future. The patient and their family members are responsible for sharing their understanding of the disease, the burden of symptoms, QOL, and functional status. The patient’s values about health, desired goals, and wishes should be expressed during the discussion. Writing an ACP is a shared decision-making process in which patients, families, and medical providers discuss together what choices the patient wants to make now or in the foreseeable future within a medically reasonable part, and the decisions made through this process are formalized in various documents (Table 4).32) The healthcare proxy form should have been completed long before the EOL, but it should be confirmed during the ACP discussion. The ACP documents that result from that discussion should be regularly reviewed, revised, and updated continually during routine conversations about treatment goals, values, and patient preferences. This process clarifies the patient's health goals and treatment preferences and allows medical staff to follow the patient's wishes when the patient is unable to participate in decision-making. Furthermore, it can reduce the burden and pain of family members who are also experiencing the last period of the patient’s life.

Table 4
Advance care planning documentation32)
MOLST = the Medical Orders for Life-Sustaining Treatment; POLST = the Physician Orders for Life-Sustaining Treatment.
![]()
Identifying a substitute decision maker (SDM) to reflect the patient’s values and wishes is an indispensable step. The SDM is encouraged to participate early in the process of developing the ACP to share the patient’s values about life, goals of care, wishes, beliefs, and preferences. SDM must be prepared for future decision making by discussing these factors.
An important part of the ACP is determining where the patient and their family members will spend the last few days of the patient’s life. More than expected patients with a terminal illness prefer home as their site of death, but the congruence between the preferred place and the actual place of death is unsatisfactory.33)34)35)36)37) Dying at home requires constant family support, which is not always available. In Korea, satisfying the preferred place of death is complicated by the lack of a home-based nursing program and limited accessibility to medical care. Many patients with chronic illness fear that their medical contact out of hospital could be restricted, and patients receiving high-intensity therapies are generally not eligible for home hospice. Hemodialysis and intravenous inotrope infusion, for example, can be a considerable obstacle to EOL care at home. In such a circumstance, the existing high level of support should generally be discontinued before discharge, and it should be fully recognized that death might occur in the hospital. The establishment of an integrated system to provide EOL care, coordinated by an HF specialist, palliative care specialist, and home nursing specialist, is needed to address the range of needs of patients and their caregivers.
Go to :
REVIEW AND ADJUSTMENT OF CURRENT HEART FAILURE MANAGEMENT
Unlike cancer patients who stop aggressive disease-modifying treatments such as chemotherapy or radiotherapy, most HF patients need to continue their baseline HF treatment, such as diuretics, renin-angiotensin-aldosterone system blockers, beta blockers, or mineralocorticoid antagonists. At this point, it is mostly appropriate to maintain the treatment already in use to stabilize the patient, but in some cases, certain treatments can be added or discontinued to relieve the patient’s symptoms and improve QOL. Medication deprescribing is a proactive, patient-centered approach founded on good prescribing principles that takes into consideration the context of a patient’s changing goals of care, values, preferences, and perceived life expectancy.38) There are a variety of reasons to deprescribe in the setting of inexorable HF progression: a treatment burden that outweighs the benefit, a risk of adverse drug reactions from polypharmacy, declining pharmacologic and metabolic efficacy, and poor patient adherence. Optimizing diuretic therapy and down-titrating beta-blockers can be considered in worsening congestion. Similarly, symptomatic hypotension might require down-titration of beta-blockers or renin-angiotensin-aldosterone system inhibitors. Aborting some medications might worsen the long-term prognosis of stable chronic HF patients, but it might not cause acute deterioration of cardiac function in the last few days of life. Patients and their family members should understand that stopping a previous medication could shorten the patient’s life expectancy (Table 5).
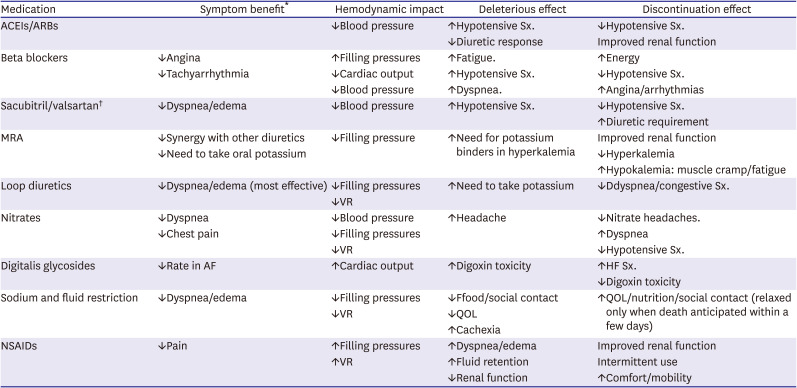
Table 5
Symptom benefit and discontinuation effect of cardiovascular medications at the end of life32)
ACEIs = angiotensin-converting enzyme inhibitors; AF = atrial fibrillation; ARBs = angiotensin receptor blockers; HF = heart failure; MRA = mineralocorticosteroid antagonist; NSAIDs = nonsteroidal anti-inflammatory drugs; QOL = quality of life; VR = valvular regurgitation; Sx = symptoms; ↓ = decreased; ↑ = increased.
*Short-term symptom benefit in continuing medication at end of life; †Insufficient experience to anticipate effects of withdrawal near end of life.
![]()
Maintaining a euvolemic state is essential in HF treatment. HF patients at the EOL commonly show poor volume control and frequently experience diuretic resistance. However, because several recommendations already cover diuretic use in patients with HF and diuretic resistance,39)40) we do not discuss diuretic therapy in this review.
Continuous infusion of intravenous inotropes can be helpful in HF patients at the EOL who have uncontrolled symptoms refractory to GDMT. Inotropic support is recommended only to palliate symptoms in selected EOL patients who are ineligible for mechanical support or transplantation because inotropes have not shown improved survival in previous studies.11)41)42)43)44) However, based on limited evidence, inotropic therapy in HF patients at the EOL does seem to improve dyspnea without hastening death.20) Even in cases in which intravenous inotropes are used temporarily, initiation should be made after careful consideration of the potential risk of adverse effects and benefits of symptom palliation. Recently, advanced HF patients on home-based intravenous inotrope infusion for palliation showed a median survival of 9.0 months, an actual 1-year survival of 47.6%, and 2-year survival of 38.4%, all of which were modestly better than previously reported.45) However, intravenous inotropes are often complicated by intravenous access routes, infusion costs, and limited outpatient availability. In Korea, most patients receiving intravenous inotropes infusion have to remain in the hospital. Increased healthcare costs and reduced accessibility to hospice care must thus also be taken into consideration.
The discontinuation of potentially life-sustaining treatment, including the deactivation of cardiac devices, discontinuation of renal replacement therapy, and the deactivation of mechanical circulatory devices, should also be discussed. Though proactive communication about device deactivation is needed at the time of treatment initiation, physician discomfort, lack of counseling, and patient misconceptions can make that difficult.46) Planning for device deactivation is an essential part of EOL care for the recipients.
Go to :
SYMPTOM ASSESSMENT AND MANAGEMENT
Patients with ESHF have a high burden of symptoms despite traditional medical therapy, which results in HF progression and other comorbid conditions.7)8)47) The burden of symptoms in ESHF patients is as high as that seen in patients with advanced cancer or acquired immune deficiency syndrome.7) These symptoms appear more frequently as death approaches.7)48) The main symptoms presented in HF patients at the EOL are dyspnea, pain, anxiety/depression and fatigue.8)19) Because the non-typical symptoms, such as pain, anxiety, and depression, are easily neglected in HF clinics, care should be taken to identify them. Moreover, given the considerable mismatch between symptoms identified by physicians and those of which patients complain, physicians, patients, and caregivers have to share the responsibility for symptom recognition.7)
Regular symptom assessments using validated scales are essential for managing debilitating symptoms. The use of standardized instruments to measure symptoms can help in their early recognition and management. Clinically, numeric rating scales and visual analog scales are simple to use in assessing and following up with most symptoms.7)10) The Edmonton Symptom Assessment System can be used for a more comprehensive evaluation. Patients rate their level of distress from 0 (best) to 10 (worst) in ten domains (pain, fatigue, nausea, depression, anxiety, sleepiness, appetite, dyspnea, other symptoms, and overall well-being). The summed score provides an overall distress score for non-classical HF symptoms and correlates well with the New York Heart Association functional class and the Kansas City Cardiomyopathy Questionnaire, which are frequently used in HF clinics.7)17) The HF-specific tools, such as the Minnesota Living with Heart Failure Questionnaire and Kansas City Cardiomyopathy Questionnaire, can also be used to measure the symptom burden and QOL, but they carry an additional cost for the licenses required to use them.
Dyspnea
Dyspnea is a hallmark symptom of worsening HF reported by 60–90% of advanced HF patients.19)20)48)49)50) Sustained dyspnea is closely related to poor outcomes, frequent medical contacts, and poor patient QOL.51)52)53) Many explanations have been proposed for dyspnea in ESHF (Figure 2). Volume overload and increased left ventricular filling pressure are its main causes. These can be optimized with medical treatment, including diuretics and vasodilators, but despite GDMT, it is often impossible to completely alleviate dyspnea. Multiple comorbid diseases, such as obstructive pulmonary disease, skeletal muscle weakness, physical deconditioning, and malnutrition, can also contribute to sustained dyspnea in HF patients.55) Oversensitivity of the arterial chemoreceptor and overactivation of the muscular ergoreceptor, which detects metabolic changes in muscular work, are also suggested as important factors that contribute to poorly controlled dyspnea.56)57)
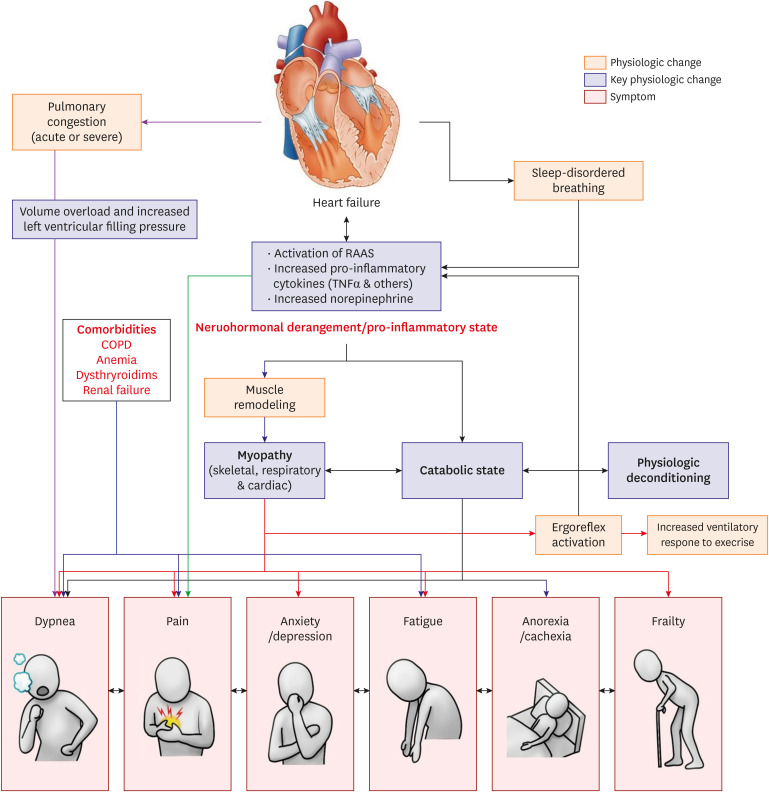 | Figure 2Main symptoms presented in heart-failure patients at the end of life and suggested mechanisms.54) Regardless of etiology, heart failure is characterized by neurohormonal derangement and a pro-inflammatory state, resulting in muscle remodeling/myopathy and a catabolic state. These neurohormonal and cytokine alterations result in respiratory and skeletal muscle atrophy and weakness, which contribute to symptoms of dyspnea, (anticipatory) anxiety, fatigue, and frailty. The activation of the ergoreflex in muscle affects the increased ventilator response to exercise. A catabolic state and related physical deconditioning result in dyspnea, fatigue, anorexia, and cachexia. Overt pulmonary congestion, volume overload, and increased left ventricular filling pressure are associated with dyspnea. Sleep-disordered breathing contributes to daytime fatigue. Comorbidities can also contribute to the symptom spectrum in heart failure.COPD = chronic obstructive pulmonary disease; RAAS = renin-angiotensin-aldosterone system; TNF = tumor necrosis factor.
|
Although the few relevant studies have shown inconsistent results,58)59)60)61) supplemental oxygen can be given for symptom relief and functional improvement with minimal adverse effects.10) Some evidence indicates that exercise rehabilitation, including physical exercise and inspiratory muscle training, can alleviate dyspnea,62)63)64) but many of ESHF patients are unable to continue exercise therapy due to their weakness and fatigue. Although the evidence is scant, electrical stimulation appears to be an effective muscle training method for ESHF patients who are too frail to perform a full exercise program.65)66)67)
Low-dose opioids are a safe and effective option for relieving intractable dyspnea. Morphine and codeine improved dyspnea and exercise capacity in small randomized trials.68)69)70) That effect might be associated with the decreased chemosensitivity associated with opioid use. The potential adverse effects of opioids, such as constipation, nausea, and dizziness, should be explained to patients. Respiratory depression, a rare but dangerous side effect, should be carefully monitored in all patients, especially elderly patients and those with impaired renal function.10) Benzodiazepines can be considered when other measures have failed to relieve dyspnea, especially in patients with strong anxiety.10)20)
Pain
Pain among ESHF patients is common, reported by up to 89% of New York Heart Association functional class IV patients, and it is often undertreated.7)48)71) Pain originates from several factors that can be caused by the advanced HF itself or related to other comorbid diseases or mental stress (Figure 2); in many cases, no clear cause can be found.20) Uncontrolled pain can decrease medication adherence, diminish self-care ability, worsen QOL, and increase hospitalizations.7)
Non-pharmacologic management, such as massage and physical therapy, can be helpful.7)10)46) Even though acetaminophen is preferentially recommended as a non-opioid analgesic, there is no evidence of its effectiveness for neuropathic pain, and in many cases, it does not sufficiently control pain.20) Nonsteroidal anti-inflammatory drugs are generally not recommended for HF patients because of concerns about fluid retention and kidney injury.7)46) Neuropathic pain can be also treated with non-opioid medications such as anticonvulsants and antidepressants.
Opioids can be a useful alternative therapy for ESHF patients who do not respond to non-opioid analgesics. Tramadol, oxycodone, hydromorphine, and fentanyl are recommended as safe and effective options for those patients.7)10)20)46) Caution is needed when considering chronic use of morphine and codeine, especially in patients with renal impairment, because of their renal excreted neurotoxic metabolites. Concerns about overdoses and opioid addiction are major barriers to effective pain management in ESHF patients. However, true addiction in terminally ill patients is rare, and the benefits of using opioids for effective pain control surpass the risk of side effects.
Anxiety and depression
Anxiety and depression are commonly encountered problems in patients living with HF and tend to increase as HF symptoms worsen and functional status deteriorates.72)73)74) Depression per se also aggravates HF symptoms and worsens medication adherence.7) When anxiety or depression is identified, treatment for the underlying cause, such as dyspnea or pain, is the first step. Non-pharmacological therapy such as exercise and cardiac rehabilitation can improve depressive symptoms.75)76)77)
Selective serotonin reuptake inhibitors, such as paroxetine and sertraline, are effective first-line therapies for depression in HF patients and have a favorable side-effect profile.78)79)80) These drugs should be started at a low dose, and monitoring for hyponatremia and fluid retention is needed, particularly in patients with renal dysfunction. Tricyclic antidepressants should be prescribed with caution due to the risk of QT prolongation and a negative inotropic effect.7)20)
Fatigue
Generalized fatigue can result from low cardiac output, depression, generalized myopathy associated with neurohormonal derangement, and comorbidities (Figure 2). Neurohormonal and cytokine alterations can produce respiratory and skeletal muscle atrophy and weakness, which contribute to symptoms of fatigue and limited exercise capacity. Therefore, before managing fatigue, it is essential for clinicians to identify its underlying causes, including low cardiac output, depression, anemia, thyroid dysfunction, uremia, renal failure, excessive use of diuretics, electrolyte imbalance, and sleep apnea.20) Fatigue caused by ESHF is often unresponsive to drug therapy; thus, non-pharmacological treatment, such as aerobic exercise and energy-sparing therapy, might be effective.64)81)
Nausea and vomiting
Nausea and vomiting near the EOL commonly result from side effects of medications (including opioids), uremia, and gastrointestinal edema.82) Although some cases of nausea and vomiting can be treated according to their cause, most episodes come from multifactorial or uncertain causes. The evidence supporting the efficacy of antiemetics in patients at the EOL is scant. Serotonin antagonists (e.g., ondansetron), dopamine-receptor antagonists (e.g., metoclopramide and haloperidol), and first- or second-generation antipsychotics (e.g., prochlorperazine and olanzapine) can be used.82)83)
Frailty, cachexia, and sarcopenia
Frailty, cachexia, and sarcopenia are associated with physical deconditioning in advanced HF. These conditions can overlap with comorbidities, particularly in elderly HF patients. Frailty, exhibited as poor physiological reserve and increased vulnerability, is found in about 45% of HF patients, though the exact proportion of affected patients is uncertain because no assessment tool has been specifically validated for HF patients. Cachexia and sarcopenia could be evident in 5–15% of HF patients.84) This recognition rate varies in clinical practice, and the first indicator is an involuntary weight loss of more than 5% over 3–12 months. If diagnosed early, frailty, cachexia, and sarcopenia can be attenuated through exercise interventions provided alongside GDMT.85)86)87) Muscle abnormalities in HF are similar to sarcopenia caused by aging, which also likely relates to abnormalities of the renin-angiotensin-aldosterone system and proinflammatory abnormalities common in elderly people.88)89)
Palliative sedation to unconsciousness at the end-of-life
Palliative sedation to the point of unconsciousness might be the last-resort option when distressing symptoms cannot be controlled despite expert consultation and treatment.90) Although this is widely recognized as an ethically appropriate approach in EOL care,91) it is still difficult to apply in clinical practice in Korea. The goal, of course, is to relieve refractory suffering, not to hasten death. Therefore, it should not be confused with physician-assisted dying or voluntary euthanasia. The patient or a legal surrogate must agree that such an approach is justified. Consultation with specialists in palliative care, ethics, psychiatry, and other areas should be considered before a decision to initiate palliative sedation is made.82)
Many palliative care needs can be addressed by the patient’s interdisciplinary care team (primary palliative care). However, specialty palliative care clinicians (secondary palliative care) can be consulted to collaboratively care for patients and families with particularly challenging needs. Formal palliative care consultation can be especially helpful for patients with 1) refractory symptoms; 2) major medical decisions to make; or 3) multiple comorbidities, frailty, or cognitive impairment.11) In one study, multidisciplinary palliative care intervention in advanced HF patients showed greater benefits in QOL, anxiety, depression, and spiritual well-being compared with usual care alone.92)
Go to :
PSYCHOLOGICAL SUPPORT AND SPIRITUAL CARE
Loss of physical and social functioning has enormous consequences for ESHF patients and their family members. In fact, patients with progressive disease can experience the fear of death, anxiety about burdening their families, uncertainty and despair over the course of their disease, and social isolation. Therefore, clinicians should be well aware of the causes of loss and despair that patients feel, screen for spiritual interest, and make appropriate connections to priests or other religious communities. Careful attention and access, including grief counseling for families left behind after bereavement, are important parts of EOL support.
Spirituality is defined as “the aspect of humanity that refers to the way individuals seek and express meaning and purpose and the way they experience their connectedness to the moment, to self, to others, to nature, and to the significant or sacred.”93) Spirituality thus plays an important role in coping with disease and improving QOL.94) Even though spiritual concerns and needs are common in patients at the EOL, only a minority of clinicians address the spirituality of their patients.19)94) Clinicians can identify spiritual beliefs and sources of support by asking the FICA questions (Table 6).95) Clinicians should recognize that spiritual well-being is an important part of EOL care, and they should endeavor to provide the necessary elements by properly understanding the patient's interests and need for spiritual support.

Table 6
FICA questions for addressing spirituality95)
![]()
Go to :
CAREGIVER BURDEN AND BEREAVEMENT
Although most family and informal caregivers embrace the opportunity to help, they might still struggle with the inevitable physical, emotional, and economic burdens of caregiving. As patients approach the EOL, those burdens grow.96) A challenging situation, such as deactivation of an implantable cardioverter defibrillator (ICD) or left ventricular assist device (LVAD), can impair the emotional well-being of caregivers.97) Therefore, careful attention to family and other caregivers, including the provision of grief counseling and bereavement services, is an important part of the EOL process.98)
Bereavement is a universal experience, defined as the situation of having recently lost a significant person through death. Bereaved individuals can experience a range of debilitating physical and psychological responses,98) and these should be addressed by an assigned member of the multidisciplinary team. For some who experience the significant suffering of a relative or friend, death can be viewed as a release. For others, bereavement is deep and protracted, which is characterized as complicated grief.99) The involvement of specialist palliative care can significantly support affected individuals.9)
Go to :
SPECIAL ISSUES WITH EOL CARE
Device treatment and deactivation: implantable cardioverter defibrillator and left ventricular assist device
The common use of device treatment has significantly reduced the mortality associated with HF. Nevertheless, these devices pose significant problems for ESHF patient who want to minimize the intensity of treatment. ICD can cause serious distress in patients with ESHF due to frequent, undesired, painful shocks,100)101) and it prolongs pain and death. Therefore, ICD deactivation is a recommended option during EOL care in ESHF. Although most clinicians understand the need to consider ICD deactivation, many are reluctant to discuss this issue with patients and their families; in one study, only 25% of patients’ families discussed switching off the ICD with the physician before the patient died.102) Even among patients who had previously expressed a wish to restrict life-sustaining therapy, ICD deactivation was discussed only near the EOL. Recent guidelines for device management have outlined a process for ICD deactivation that applies equally to cardiac resynchronized therapy.
Patients with advanced HF who are not eligible for heart transplantation might be suitable for LVAD as destination therapy (DT-LVAD). The 48-month survival rate of patients with LVAD is up to 89%.103)104) Although LVAD can alleviate HF symptoms such as dyspnea and improve exercise capacity, patients can continue to experience other symptoms, such as physical pain, depression, and anxiety.105) For DT-LVAD patients, the most common modes of death are multi-organ failure, stroke, and progressive HF,106) and the terminal phase often occurs in a hospital intensive care unit. In the face of major complications, planned deactivation of the LVAD might be indicated, with death usually occurring within an hour of withdrawal. Therefore, LVAD implantation should be performed only after extensive discussion among medical professionals, patients, and their caregivers. The LVAD care team should include palliative specialists to assist with symptom management and support the transition to EOL care, if necessary.20) Careful evaluation of the potential benefit versus burden of each device treatment and the withdrawal of those without substantial benefit is the best way to prevent harm and provide benefit for HF patients at the EOL. This careful evaluation is best approached collaboratively among disciplines.107)
Cardiopulmonary resuscitation
All HF patients are at risk of sudden cardiac arrest at any time during the entire disease trajectory. Therefore, it is very challenging to determine in advance whether to perform cardiopulmonary resuscitation (CPR) during cardiac arrest. Especially in EOL care, the benefits and prognosis of CPR cannot be evaluated. This prognostic uncertainty makes it difficult to plan for the patient’s EOL wishes. Physician Orders for Life-Sustaining Treatment is a concept advocated in the United States based on practical experience with advance directives, and it includes the do-not-resuscitation (DNR) directive, which precludes CPR in the event of cardiac arrest.108)109) Some observers have suggested that ‘DNR’ be changed to ‘do-not-attempt resuscitation (DNAR)’ because CPR can only ever be an attempt, and the chance of success is sometimes vanishingly small. For some patients and their families, the symbolic meaning of this attempt can be critical for a variety of cultural, religious, and personal reasons. The decision about whether to attempt resuscitation is one of many salient decisions that physicians are encouraged to discuss with patients and their surrogates with regard to desired EOL care.110) EOL care, including the CPR directive, should aim to meet the patient's needs regardless of their prognosis.
End-of-life care for elderly people
As society continues to age rapidly, it is necessary to pay attention to EOL care in elderly patients. The EOL process in elderly patients is known to be more complicated than in younger adults.111)112) Elderly patients might have difficulty conveying their symptoms accurately, and it might be hard for physicians to properly evaluate symptoms at an appropriate time. They are more likely than younger people to have symptoms associated with various comorbidities, including cognitive dysfunction and frailty, and to take multiple medications. In addition, the views of life and death among elderly people are known to vary. Each patient's individual circumstances and view of life and death will influence their choice of treatment strategy.107) In one study, most elderly patients chose life expectancy above QOL, and half wanted to be resuscitated as necessary.113) However, elderly patients feel close to death for the remainder of their lives and therefore tend to explore the meaning of life. Most elderly patients with HF are prepared to confront their terminal condition, and although their wishes in terms of EOL care can change according various factors, such as their degree of cognitive function and surrounding environment, the desire for a tranquil death remains constant.107)
Go to :
KOREAN PERSPECTIVES AND SUGGESTIONS FOR END-OF-LIFE CARE
With the implementation of the Life-sustaining Treatment Decision Act in February 2018, interest in EOL care for patients with advanced disease, including HF, has been increasing in Korea. However, the reality is that many obstacles remain to effectively applying EOL care in actual clinical practice. A lack of physician knowledge resulting from a lack of systematic educational programs about EOL care can lead to insufficient provision of EOL care. Medical training for a palliative approach and EOL care would improve the knowledge and experience of cardiologists, which would improve the quality of EOL care. With an educational program, cardiologists could recognize the importance of EOL care and learn to provide both optimal management of the underlying HF and appropriate palliative care as a primary care provider. In a meta-analysis, clinician-targeted interventions that included a reminder system and educational meetings effectively facilitated the development of ACPs.114)
The participation of HF specialists in palliative care consultations is an effective way to integrate EOL care into an HF program.17)115) HF doctors are responsible for managing HF and establishing an ACP. A palliative care team can help the HF doctors by controlling symptoms that do not respond to conventional therapy and supporting the psychological and spiritual aspects of the patient.
Appropriate coverage of EOL care costs from the medical insurance system could also promote the proper establishment of EOL care in HF management programs. We need to continue to develop a treatment model that is responsible for prioritizing patient and family goals throughout the whole course of HF, including the EOL, as well as being responsible for the allocation of limited medical resources as a health provider.
Fortunately, a lot of data from the Korean acute and chronic HF registration project has been published on the cause, diagnosis, prognosis, and treatment of HF, and public education about HF is also being actively conducted. As Korean society ages rapidly, the number of HF patients, especially elderly patients, and HF mortality are increasing.116) Based on domestic data and reality, Korean guidelines for integrated palliative care, including at the EOL, and appropriate management are needed. In addition, it is essential to develop and evaluate palliative care, including at the EOL, and develop a delivery model that can proceed efficiently within the Korean healthcare system.
Go to :
CONCLUSION
The treatment of HF patients should incorporate discussions about the overall goals of care and assessments of individual patient preferences for management at the EOL or sudden change in health status. Optimally, these discussions should begin early in the course of HF and be repeated as the patient’s condition changes. Especially when QOL concerns outweigh the desire to expand the quantity of life, EOL care based on the concept of `do nothing except for comfort’ should be considered. Furthermore, EOL care should support not only the patient but also the family and informal caregivers through a multidisciplinary team approach.
Go to :
 XML Download
XML Download