

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Reducing the symptom onset to recanalization time is essential to achieve better outcomes for patients with acute ischemic stroke (AIS) and acute myocardial infarction (AMI). Certifying or designating hospitals capable of treating AIS and AMI patients round-the-clock and establishing a direct transfer system to such hospitals may be the best strategies to achieve this goal.12 Several efforts have been made to implement such strategies at a national level.34 In South Korea, regional cardiocerebrovascular centers (RCVCs) were designated by the Korean Government starting in 2008.56 Currently, 12 university hospitals have been designated as RCVCs wherein patients with AMI and AIS can receive high-quality round-the clock acute care administered by, which may improve outcomes.56
However, to construct optimal care systems for AIS and AMI at a national level, there are questions that need addressing. These include whether to direct as many patients as possible to comprehensive centers; if this is the case, the number of comprehensive centers should be determined. At present, many AMI and AIS patients are transferred to higher-level centers for advanced care.789 South Korea is a relatively small country with a well-developed transport system, and most of the large hospitals with specialized care systems for AIS and AMI are located in metropolitan areas.910 Therefore, it may be more reasonable to bypass local hospitals and instead transport patients with AIS and AMI directly to large hospitals capable of advanced care.31112
Although AIS and AMI share several systemic components, including emergency medical services (EMSs), the in-hospital care for both conditions is different,12 and implementing only one system for both conditions may be inappropriate and insufficient for achieving optimal care. Identifying factors associated with direct admission versus transferred-in admission to comprehensive centers and understanding the differences between AIS and AMI can be good starting points to answer the above questions. In the literature, we can find comparisons between direct admission and transferred-in admission to comprehensive centers in patients with AIS and AMI, respectively.781314 For AIS, patients who were directly admitted were more likely to be older and have milder stroke compared with patients who were transferred-in.7 For AMI, patients who were directly admitted were more likely to be older and have previous MI, heart failure, and previous revascularization.8 However, there has been no nationwide study that investigated and compared the determinants of route of admission (direct versus transferred-in admission) between AIS and AMI under identical practice settings, which we aimed to perform in this study. The RCVC registry, which was launched in 2014 by the Korean government, provided us the opportunity to undertake this study.
METHODS
Study population
With the establishment of RCVCs, a nationwide multicenter registry was developed to monitor and improve the pre-hospital, in-hospital, and after-discharge care for AIS and AMI patients at a national level. Thus, we could use the prehospital data from the RCVC registry that were collected from the same hospitals across the country to analyze and compare the determinants of direct versus transferred-in admission between AIS and AMI patients.
The RCVC registry started to collect data in June 2014 for AIS and July 2016 for AMI. This web-based registry has automatic error-checking, user-training, and on-site monitoring to assure the quality of collected data. A training workshop for improving data entry and preventing errors is held at least once a year.615
From the registry database, we identified a consecutive series of patients with AIS or AMI who were admitted to the RCVCs via the emergency room within 7 days from symptom onset between July 2016 and December 2018.
Data collection and definitions
All patients were divided into direct and transferred-in admission groups. The direct group consisted of patients directly presenting to the emergency room of RCVCs using EMS or by themselves, while the transferred-in group consisted of patients transferred-in from other hospitals.
Information on demographics, medical history, household factors, prehospital awareness, use of EMS, education levels, exact date and time of symptom onset, and onset-to-arrival time was obtained directly from the registry database.
We defined EMS use as patients being transported from home or the scene of symptoms onset to the first hospitals (RCVC or other hospitals) via an EMS ambulance. Prehospital awareness was defined as the awareness of the patient or his/her caregiver that the patient is having an AIS or AMI at symptom onset. Symptom onset was defined as the time when symptoms relating to acute stroke or myocardial infarction were first noticed. For patients who were transferred-in, the date and time of presentation to the first hospital were also collected. Work-hour and off-hour presentations were defined as arrival at the emergency room between and beyond 8 AM and 5 PM, respectively.
Statistical analysis
Patient characteristics were summarized as frequency and percentage. Age was categorized into three groups: 18–64, 65–74, and ≥ 75 years. We had missing values in 4 variables, whose missing rates were 2.0% for onset time, 0.6% for presentation day, 3.7% for arrival time to hospitals and 4.3% for education level. The missing values were imputed using randomly selected values based on the distribution of the corresponding variables within age and sex subgroups.
Comparisons of characteristics between groups were made by Pearson’s χ2 test. To explore the determinants of direct versus transferred-in admission and their differential effects in AIS and AMI patients, univariable and multivariable generalized linear mixed models with interaction terms between each of the potential determinants of direct admission and disease type were constructed regarding a center effect as random. Adjusted odds ratios (ORs) and their 95% confidence intervals (CIs) for each determinant were estimated within the strata of disease type and in total subjects with a single common reference group, respectively, according to the previous recommendations.16
To explore patient-level factors that influence hospital selection with and without EMS, stratified analysis according to EMS use was also performed.
All statistical analyses were conducted using the SAS software version 9.4 (SAS Institute Inc., Cary, NC USA), and a two-sided p-value less than 0.05 was considered statistically significant.
Ethics statement
Collection of de-identified information from this registry without informed consent for monitoring and improving the quality of care of AIS and AMI patients was approved by the Institutional Review Boards of the participating hospitals due to study subjects’ anonymity and minimal risk to participants (IRB No. B-1410-271-116 and B-1909-564-105). The retrospective analysis of the registry database for the present study were approved additionally.
RESULTS
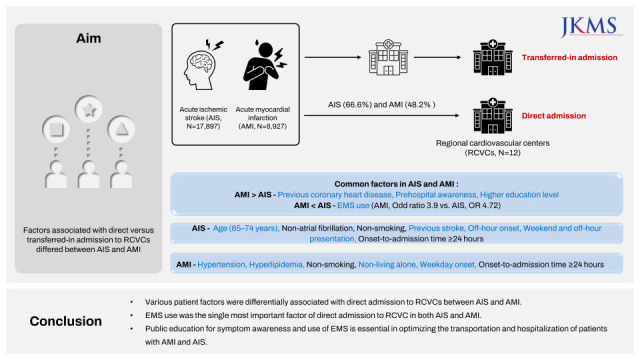
During 30 months, 26,826 patients (17,897 with AIS and 8,929 with AMI; mean age, 68.3 ± 12.9 years; 64% male) hospitalized at RCVCs were registered (Table 1, Supplementary Table 1). Overall, 60.5% (n = 16,230) and 39.5% (n = 10,596) were direct admissions and transfer-ins to RCVCs, respectively. Meanwhile, 40% of patients arrived at the first hospital via EMS.
Table 1
Comparison between AIS and AMI patients
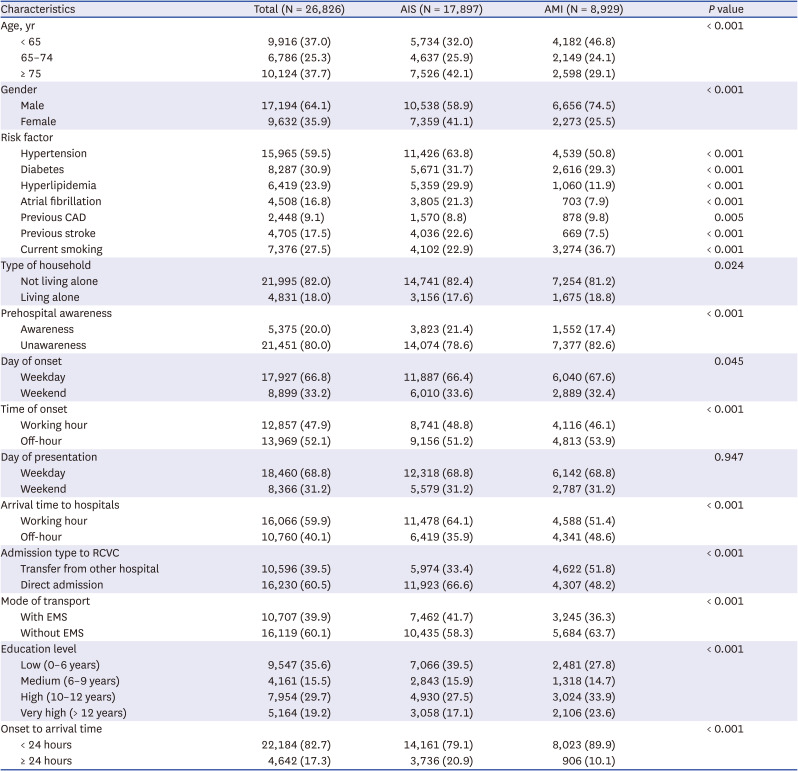
Compared to AMI patients, AIS patients were more likely to be older and to have hypertension, diabetes, hyperlipidemia, and atrial fibrillation. Prehospital awareness, work-hour presentation, and EMS use were more frequent in AIS patients (Table 1).
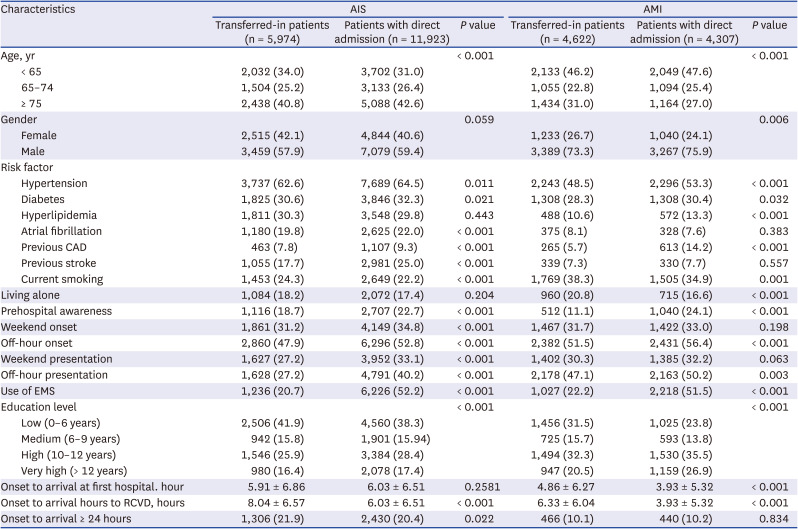
In total, 67% and 48% of AIS and AMI patients, respectively, were directly admitted to RCVCs. Among AIS patients, those who were directly admitted were more likely to be older, to have used EMS, and to have traditional vascular risk factors, higher prehospital awareness, weekend and off-hour onset and presentation, higher education level, and onset-to-arrival time ≤ 24 hours as well as less likely to be current smokers compared with those who were transferred-in. Among AMI patients, those who were directly admitted were more likely to be younger and male, to have used EMS, and have traditional vascular risk factors, previous coronary artery disease (CAD), off-hour onset and presentation, and higher education as well as less likely to be current smokers and living alone compared with those who were transferred-in (Table 2).
Table 2
Comparisons between direct versus transferred-in admissions to RCVCs according to disease type (AIS and AMI)
In the multivariable analysis, onset-to-admission time ≥ 24 hours and current smoking increased and decreased the odds of direct admission, respectively, with no difference between AIS and AMI (Ps for interaction > 0.1) (Table 3). Previous CAD, prehospital awareness, and higher education level increased the odds of direct admission in both AIS and AMI, but these associations were stronger in AMI patients than in AIS patients (Ps for interaction < 0.05). EMS use, which may be the strongest determinant, also increased the odds of direct admission in both AIS and AMI, but its association was stronger in AIS patients than in AMI patients (ORs, 4.72 vs. 3.90). A weekend onset and living alone decreased the odds of direct admission, whereas hypertension and hyperlipidemia increased the odds only in AMI. Meanwhile, age (65–74 years), previous stroke, and weekend and off-hour presentation increased the odds of direct admission only in AIS (Ps for interaction < 0.05).
Table 3
Predictors of direct admission to regional cardiocerebrovascular centers among patients with AIS and AMI: multivariate analysis
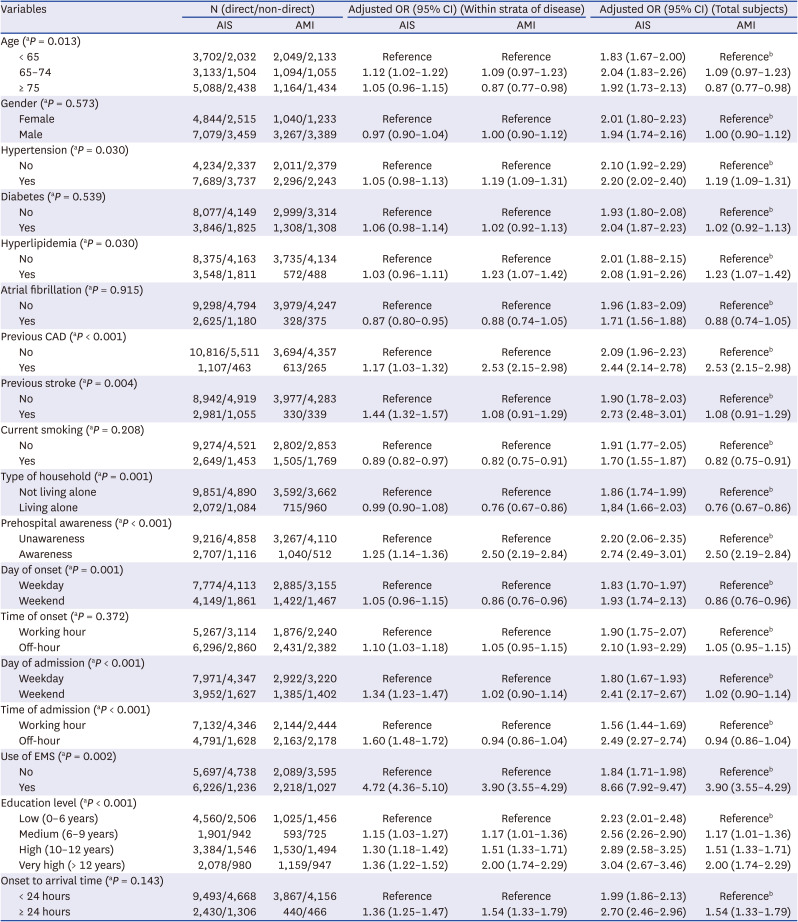
AIS = acute ischemic stroke, AMI = acute myocardial infarction, OR = odds ratio, CI = confidence interval, CAD = coronary artery disease, EMS = emergency medical service.
aP for effect modification by disease (AIS vs. AMI) on multiplicative scale.
bDefined as 4 stratums with direct admission to regional cardiocerebrovascular centers in both diseases
Analysis of subjects with a single common reference group revealed uniformly increased odds of direct admission to RCVCs in AIS patients compared to AMI patients (Table 3).
Stratified analysis according to EMS use was performed (Supplementary Tables 2 and 3). In patients who did not use EMS, the effects of most factors on direct admission were similar to those in the whole study population. However, the difference between AIS and AMI seemed to be greater in patients who did not use EMS. For example, the adjusted ORs of previous CAD on direct admission were 2.53 and 1.17, and 3.45 and 1.19 for AMI and AIS in the whole study population and in patients who did not use EMS, respectively (Supplementary Table 2). In patients who used EMS, the associations with direct admission weakened for most of the factors except prehospital awareness (Supplementary Table 3).
DISCUSSION
Among the 26,000 AIS and AMI patients from the nationwide RCVC registry, 40% were transferred-in from other hospitals. The proportion of patients transferred to RCVCs was higher among AMI patients than among AIS patients (52% vs. 33%). EMS use was the single most important factor associated with direct admission in both AIS and AMI. Age, hypertension, hyperlipidemia, previous stroke/CAD, living alone, prehospital awareness, weekend/off-hour presentation, EMS use, and education level had differential effects between AIS and AMI. Previous studies mostly focused on hospital factors relating to direct versus transferred-in admission or the effects of interhospital transfers on treatment delay and clinical outcomes.711131718 There is lack of knowledge about the difference between AIS and AMI regarding the associations between patient factors and direct admission to higher-level centers at a national level.
Prehospital awareness, EMS use, and a higher education level increased the odds of direct admission to RCVCs in both AIS and AMI, which are the most important determinants to reduce prehospital delays in patients with acute coronary syndrome or stroke.1920212223 Notably, EMS use, which has been recognized as an effective method to rapidly transport patients to hospitals capable of providing acute care for AIS and AMI and reduce interhospital transfer,20242526 increased the odds of direct admission by four-fold. Although 60% of patients with AIS or AMI used EMS in the United States according to national registry data,2026 40% used EMS in this study. Thus, efforts should be undertaken to facilitate EMS use in Korea.
Previous CAD increased the odds of direct admission to RCVCs in both AIS and AMI, and previous stroke increased the odds in AIS, which are in line with those of previous studies.7813 One hypothesis about the positive effect of prior history on direct admission is that, by experiencing AIS or AMI, patients and/or caregivers inherently recognize that early and direct admission to higher-level centers may lead to good outcomes. Hypertension and hyperlipidemia increased the odds in AMI, but diabetes and atrial fibrillation did not in both AIS and AMI. Patients with vascular risk factors may have been educated regarding the importance of rapid treatment, but there is no explanation for its differential effect in AIS and AMI.
Weekend and off-hour onset and presentation increased the odds of direct admission to RCVCs in patients with AIS. These imply that RCVCs in Korea perform their expected roles well as round-the-clock regional comprehensive centers.56 However, a weekend onset decreased the odds of direct admission in AMI patients. Although uncertainty exists over the benefit of organizing regional transfer systems for AIS and AMI,2728 direct admission to hospitals capable of providing acute care is beneficial to most AIS or AMI patients.81225 Further investigations are required to elucidate the differences between AIS and AMI.
Understanding the differential impact of factors associated with direct versus transferred-in admission between AIS and AMI may affect the design of educational interventions to improve public awareness. In this study, it was difficult to explain why prehospital patient factors such as hypertension, hyperlipidemia, living alone, prehospital awareness, and higher education level had a greater impact on direct admission to RCVCs in AMI than AIS, and age (65–74 years) and weekend and off-hour presentation had a greater impact on direct admission in AIS than AMI. Despite their similarities, initial presenting symptoms are significantly different between AIS and AMI.23 In AIS, selection of a visiting hospital is influenced by symptoms because altered consciousness, cognitive impairment, or aphasia render a patient incapable of calling for help. Hence, decisions for choosing a hospital could be made by other individuals. Among calls for stroke that activated the EMS, > 60% were made by family members, and 18% were made by paid caregivers.29 Thus, the impact of prehospital patient factors on direct admission can be weaker in AIS. Prehospital patient factors relating to delays in seeking treatment were more influential in AMI than AIS.23 In contrast, EMS use had a greater effect on direct admission to RCVCs in AIS than in AMI, which may be explained by paramedics likely transporting AIS patients with severe symptoms to RCVCs than those without.
When stratifying the study population according to EMS use, the association of most factors with direct admission and their differences between AIS and AMI were strengthened in EMS non-users and weakened in EMS users. This suggests that EMS paramedics are quite influential in selecting the hospital where a patient will be brought to. Further studies are needed to identify factors determining EMS use in patients with AIS and AMI. To facilitate direct admission to RCVCs, the primary intervention should be educating the public regarding EMS use as well as tailored approaches, including improving disease awareness.
The strengths of this study are its large sample size, nationwide scale, and prospective and extensive data collection, including prehospital factors. However, limitations should also be noted. First, this study enrolled patients admitted to 11 university hospitals designated as regional centers in South Korea. Thus, the generalizability of the results to other countries with different healthcare systems is limited. Second, despite adjustments of all variables, unmeasured confounders might have influenced our findings. The types and severity of presenting symptoms, socioeconomic status, and distance from scene of disease onset to hospitals may affect the selection of first hospitals, although data regarding these were not available in this study. Third, this study did not include patients with AIS or AMI who were admitted to hospitals other than RCVCs and were not transferred to the corresponding RCVCs. Lastly, differences in clinical outcomes between those directly admitted and transferred-in could not be compared.
In conclusion, a significant proportion of patients with AIS and AMI undergo interhospital transfer to RCVCs, and prehospital patient factors between those with AIS and AMI differentially affect route of admission to RCVCs. Importance of influence of EMS use and pre-hospital awareness on direct admissions to RCVCs, as well as the differential impacts of prehospital patient factors on direct admission between AIS and AMI should be noted. Public education regarding the use of EMS is needed to optimize the transportation and hospitalization system after AMI and AIS.
 XML Download
XML Download