

 PDF
PDF Citation
Citation Print
Print




INTRODUCTION
Since the World Health Organization declared the coronavirus disease 2019 (COVID-19) a global pandemic in March 2020, the COVID-19 pandemic has caused over 550 million confirmed cases, including 6 million deaths globally.1 Currently, COVID-19 continues to be a threat to public health. Vaccines are considered the most promising approach to preventing severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. However, almost one billion people in lower-income countries remain unvaccinated. In addition, the emergence of variants and waning immunity require booster or additional doses of vaccines.2
Multisystem inflammatory syndrome in children (MIS-C) associated with COVID-19 was first described in April 2020, and a similar clinical syndrome was reported in adults (MIS-A) in June 2020.34 To date, there are a limited number of case reports of MIC-A after COVID-19 vaccination without evidence of prior or recent infection with SARS-CoV-2. Therefore, an appropriate treatment strategy for MIS-A after vaccination has not yet been established. Recently, we experienced a definitive case of MIS-A after COVID-19 vaccination and successfully treated the patient with medium-dose steroids and colchicine.
CASE DESCRIPTION
A 52-year-old man visited our emergency room with a four-day history of fever, headache, dizziness, and vomiting. The patient also complained of anterior chest pain. He had received two doses of the BNT162b2 mRNA COVID-19 vaccine on his left upper arm, 62 days and 20 days before the onset of symptoms. After the first dose of COVID-19 vaccine, no local or systemic adverse events occurred. He had no prior history of confirmed or suspected COVID-19 and no close contact with known COVID-19 case within 12 weeks. denied any other past medical history or allergies. Physical examination revealed bilateral nonexudative conjunctivitis. There was no rash or erythema on the whole body. His blood pressure was 66/47 mmHg with a pulse rate of 110 beats/min, respiratory rate of 22/min, and body temperature of 38.2°C. Laboratory findings showed leukocytosis with left shift and lymphopenia, an increase in inflammatory markers, hepatic enzymes, N-terminal pro-B-type natriuretic peptide (NT-proBNP), and D-dimer (Fig. 1). He had a negative SARS-CoV-2 real-time polymerase chain reaction (PCR) test following a nasopharyngeal and throat swab. The respiratory virus panel, including influenza, was also negative. A computed tomography (CT) imaging of the chest and abdomen revealed enlarged lymph nodes with soft tissue infiltrations in the left axilla and mesentery (Fig. 2). Hypotension persisted despite adequate fluid resuscitation and norepinephrine infusion was required. He was admitted to the intensive care unit and treated with empirical antibiotics (ceftriaxone 2 g once daily) and high-flow O2 therapy.
Fig. 1
Clinical course, laboratory findings, and treatment of the patient.
ALT = alanine aminotransferase, AST = aspartate aminotransferase, COVID-19 = coronavirus disease 2019, CRP = C-reactive protein, ESR = erythrocyte sedimentation rate, NT-proBNP = N-terminal pro-B-type natriuretic peptide, PaO2 = arterial oxygen tension, PCR = polymerase chain reaction, SaO2 = arterial oxygen saturation, SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2, WBC = white blood cell, HFNC = high flow nasal cannula.
aOxygen therapy via nasal prong (5 L/min).
bOxygen therapy by HFNC (forced inspiratory oxygen, 50–60%; flow rate, 40–45 L/min).
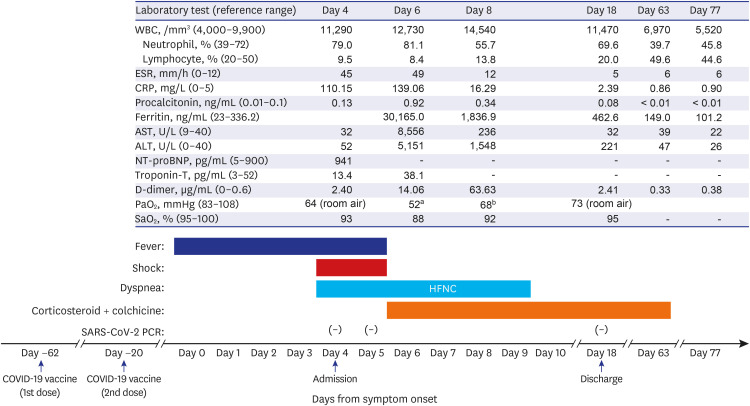
Fig. 2
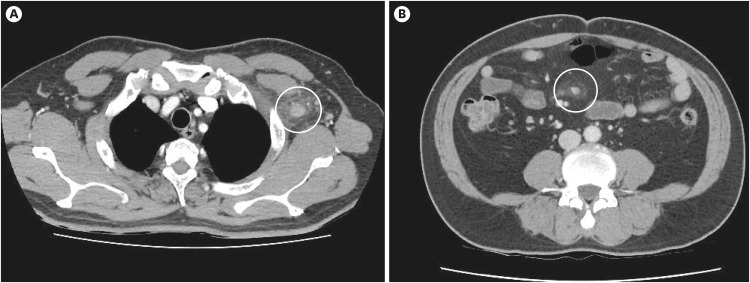
CT scans at admission. Chest CT (A) and abdomen CT (B) show enlarged lymph nodes with soft tissue infiltrations (circles) in the left axilla and mesentery.
CT = computed tomography.
Despite empirical antibiotics and supportive therapy, on hospital day 3, hypoxia and his laboratory tests deteriorated (Fig. 1). His urine output decreased to less than 0.5 mL/kg/h. Transthoracic echocardiography showed normal cardiac chamber dimension, preserved left ventricular contractility without regional wall motion abnormalities (global left ventricular ejection fraction, 53%), and no evidence of vegetations; however, a moderate amount of pericardial effusion was found (Fig. 3). A CT of lower extremity angiography and lung perfusion scan revealed no thrombosis. The initial blood cultures, antinuclear antibodies, anti-neutrophil cytoplasmic antibodies, and serology for various viral infections, leptospirosis, and rickettsial disease were all negative. The patient was diagnosed with MIS-A (level 1 of diagnostic certainty—definitive case) after BNT162b2 mRNA COVID-19 vaccination (Fig. 4). We started oral prednisolone 0.3 mg/kg/d (20 mg once daily) with colchicine (0.6 mg twice daily) and low-molecular-weight heparin (enoxaparin, 40 mg once daily) to prevent venous thromboembolism (Fig. 4). Within the first 24 hours, all clinical symptoms and signs showed dramatic improvement. On hospital day 7, a repeated transthoracic echocardiography showed a decrease in pericardial effusion to a small amount, and no other new findings were observed. The laboratory findings also gradually normalized over 2 weeks. The patient was discharged on hospital day 15. Prednisolone was tapered over 2 months and colchicine was administered for a total of 3 months. At the 2-month follow-up after discontinuation of all medications, the patient was still in good condition and all laboratory findings were within normal range.
Fig. 3
Transthoracic echocardiography. Apical four-chamber view (A) and substernal four-chamber view (B) show a moderate amount of pericardial effusion (asterisks).
LA = left atrium, LV = left ventricle, RA = right atrium, RV = right ventricle.
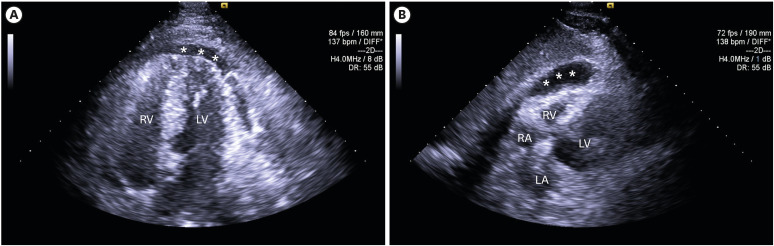
Fig. 4
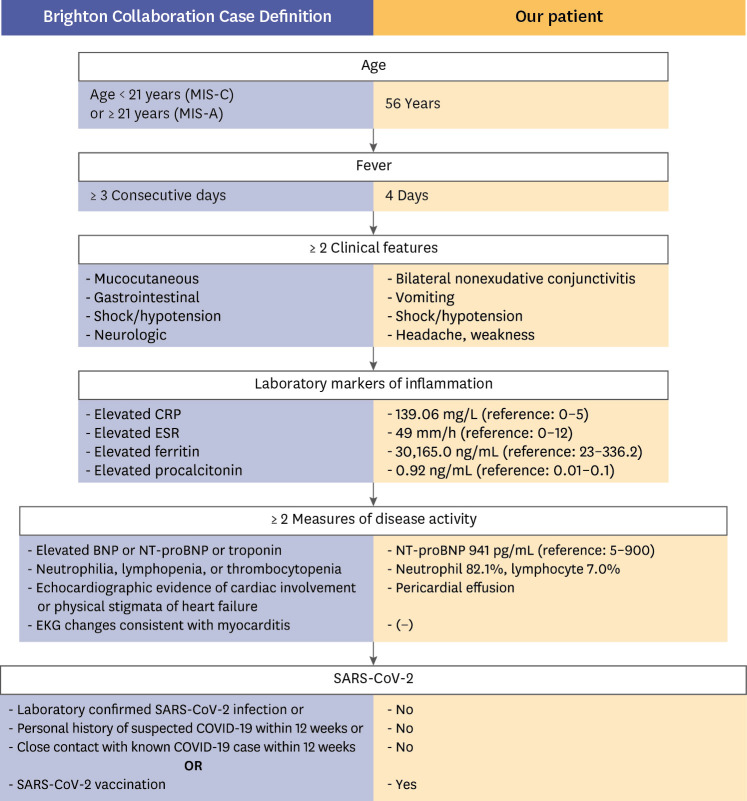
Diagnostic algorithm for the definitive case of MIS-A following SARS-CoV-2 vaccination in the patient: left column (blue), Brighton Collaboration Case Definition; right column (yellow), our patient.
COVID-19 = coronavirus disease 2019, CRP = C-reactive protein, EKG = electrocardiogram, ESR = erythrocyte sedimentation rate, MIS-C/A = multisystem inflammatory syndrome in children and adults, BNP = B-type natriuretic peptide, NT-proBNP = N-terminal pro-B-type natriuretic peptide, SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2.
DISCUSSION
We report a patient with diagnosis of vaccine-related MIS-A on the basis of age, fever, clinical features (conjunctivitis, vomiting, hypotension, and headache), elevated inflammatory markers and NT-proBNP, neutrophilia, lymphopenia, and pericardial effusion. The patient’s SARS-CoV-2 PCR was repeatedly negative. He received the COVID-19 mRNA vaccines 62 days and 20 days prior to the onset of symptoms and had no personal history of COVID-19 or close contact with a known COVID-19 case within 12 weeks. Our patient was successfully treated with medium-dose steroids and colchicine.
MIS-C was first recognized in the United Kingdom in April 2020.3 A life-threatening hyperinflammatory shock 4–6 weeks after primary SARS-CoV-2 infection in children was termed MIS-C. However, the clinical signs and symptoms of MIS-C/A overlap with other disorders, and there is no specific test to diagnose MIS-C/A. In May 2020, case definitions for MIS-C were published by the Royal College of Paediatrics and Child Health, the United States Centers for Disease Control and Prevention, and the World Health Organization.567 Since then, a similar clinical syndrome has also been reported in adults after primary SARS-CoV-2 infection and after COVID-19 vaccination.48910111213 In February 2021, the Brighton Collaboration created the standardized case definition for MIS-C/A as an adverse event following immunization with three levels of diagnostic certainty: definitive (level 1), probable (level 2), and possible case (level 3).14 The Brighton Collaboration Case Definition of MIS-C/A could facilitate the diagnosis of MIS-C/A after vaccination and allow comparability worldwide.
The current understanding of the pathophysiology of MIS-C/A is growing but still unclear. To date, there are no established guidelines on the management of MIS-C/A. General supportive care and close monitoring for potential compromise are crucial. High-dose steroids have also been used as an anti-inflammatory agent in most reported MIS-A cases after COVID-19 vaccination.8910111213 However, there are concerns about a decrease in vaccine efficacy and undesirable side effects due to the immunosuppressive effect of high-dose steroids. Therefore, it is beneficial to use the lowest effective dose of steroid as much as possible. Colchicine is an anti-inflammatory agent that inhibits activation, degranulation, and migration of neutrophils and disrupts the inflammatory cycle. Colchicine is recommended in combination with other anti-inflammatory agents for all patients with acute idiopathic or viral pericarditis because of its better remission rates and lower risk of recurrence.1516 In addition, it is used to treat gout, coronary disease, and familiar Mediterranean fever. In the COVID-19 pandemic, colchicine was one of the drugs being explored for repurposing as a potential anti-inflammatory drug based on its mechanism of action.17 Similarly, it can be hypothesized that colchicine may be helpful in treating MIS or preventing the recurrence of hyperinflammation.
Our case fulfilled the level 1 definition (definitive case) of MIS-A as an adverse event following immunization and there was no evidence of alternative diagnoses. He had no prior diagnosis of COVID-19 and received the BNT162b2 mRNA COVID-19 vaccine 62 days and 20 days before the onset of symptoms. The Brighton Collaboration Case Definition did not define a time interval between immunization and the onset of the event. However, the Working Group commented that a timeline similar to MIS-C/A after infection of SARS-CoV-2 seems reasonable, i.e., 4–6 weeks for children and up to 12 weeks for adults.14 As soon as possible we recognized that our case met the case definition of MIS-A after vaccination, and steroids were administered immediately. We started with the lowest dose recommended in patients with acute pericarditis (0.2–0.5 mg/kg/d).18 This was based on the following reasons: 1) the optimal dose of steroids for MIS-A treatment is unknown, 2) the goal of steroid therapy is to maximize the anti-inflammatory effect and minimize side effects, and 3) moderate-dose steroids were superior to high-dose steroid for treatment failure or recurrent pericarditis. Colchicine was also given because it may at least be helpful in the treatment of MIS-A with complications of acute pericarditis. The co-administration of medium-dose steroids and colchicine improved dramatically the patient’s clinical signs and symptoms, and the event has not recurred after the end of treatment.
Even though all of the approved COVID-19 vaccines have been carefully tested and ensured safety, fears about adverse events of COVID-19 vaccination remain a critical hurdle for the mass vaccination campaigns. A limited number of adults who developed MIC-A following SARS-CoV-2 vaccination had been reported. To detect and respond to rare adverse events, vaccine safety monitoring and investigation of any adverse events should continue. When a patient develops a fever, hypotension, and elevated inflammatory markers after COVID-19 vaccination, clinicians should perform a thorough history, physical examination, and laboratory investigation to rule out other conditions. If clinical suspicion of MIC-A is high, it should not delay potential treatment. International research collaboration is essential to establish the best treatment options for MIC-A.
 XML Download
XML Download