

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
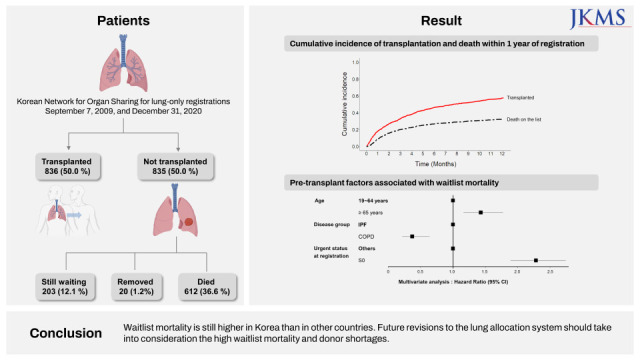
Lung transplantation provides survival and quality of life benefits in a selected subset of patients with end-stage lung disease.1 In Korea, a total of 686 lung transplants were performed between 2010 and 2019, and the number is increasing annually. In 2019, lung transplants increased by 70.7% compared with those in the previous year.2 Furthermore, the number of patients on the waitlist is rapidly rising, with an annual growth rate reaching 15% in 2019.2 Unfortunately, a huge mismatch between the demand for lung transplantation and the supply of donors’ lungs is arising.3 Therefore, the waitlist mortality rate has increased, with a 7.9% annual rise in 2019.2
In the US, donors’ lungs are transplanted first in patients based on the waiting time. Since waitlist mortality steadily increased, the lung allocation score (LAS) system for donor lung allocation was introduced in 2005.4 The LAS system was designed to allocate donor lungs according to the medical urgency and possibility of success after transplantation.5 The new allocation system induced positive results, such as decreased median wait time and waitlist mortality, and increased transplant rate without adverse effects on post-transplant outcomes.678 However, the Korean lung allocation system is based on medical urgency, which is different from the LAS system of the US that considers transplant benefits.9 Therefore, status 0 patients on mechanical ventilation (MV) or extracorporeal membrane oxygenation (ECMO) are given the highest priority for transplantation in Korea.10
In this regard, analyzing and understanding the current status of patients on the lung transplant waitlist is essential to improve the current lung allocation system in Korea. We evaluated the waitlist outcome of patients waiting for lung transplantation and the clinical factors that affect waitlist mortality.
METHODS
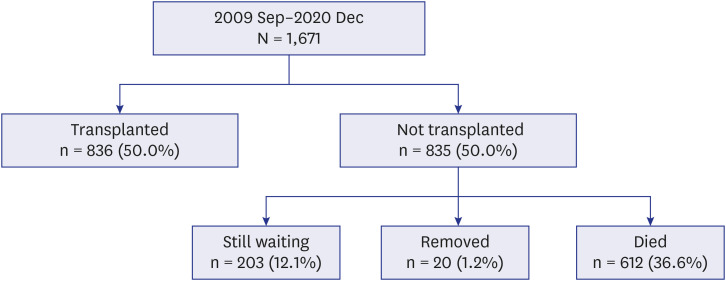
The patients comprised all lung-only registrations between September 2009 and December 2020. The survival status and date of death were collected until June 2021 for all patients included in this study. Collected data contained donor, candidate information, such as age, sex, date of registration, diagnosis, ABO blood type, urgency status at registration, death on the waitlist, date of transplantation, urgency status at transplantation, and date of death after transplantation. On the lung recipient registration forms, primary diseases were recorded and categorized into four groups for analysis, which were as follows: group A (chronic obstructive pulmonary disease, bronchiectasis, cystic fibrosis, and lymphangioleiomyomatosis), group B (primary pulmonary hypertension and Eisenmenger syndrome), group C (idiopathic pulmonary fibrosis [IPF], sarcoidosis, asbestosis, and bronchiolitis obliterans syndrome following transplant), and group D (all other lung diseases). Patients were classified as status 0, 1, 2, 3, and 4 according to their medical urgency status, based on a previous study.10 Patients with a status 0 were defined as those who required MV or ECMO. Patients with status 1 were defined as those having one or more of the following conditions: 1) New York Heart Association (NYHA) IV and PaO2 < 55 mmHg on arterial blood gas test without oxygen administration; 2) NYHA IV and mean pulmonary arterial pressure > 65 mmHg or mean right atrial pressure > 15 mmHg, and 3) cardiac index < 2 L/min/m2. Post-registration outcomes were as follows: transplanted, still awaiting, removed, or died while on the waitlist (Fig. 1).
Waitlist mortality within 1 year
Among the 1,671 patients listed for transplantation, 1,611 completed the 1-year follow-up. The study cohort included 1,611 patients. Survival since registration was defined as the time from listing until death. Candidates who were removed from the transplant waitlist for reasons other than death were censored at the time of removal from the waitlist. All factors at the time of listing were considered potential predictors of waitlist mortality, including demographic factors and urgency status.
Time to transplant
The time to transplant was defined as the time from listing to the time of transplant. These data were censored at one of the three time points: the date of removal from the list, death on the list, or date of data extraction, if the patient was still waiting on the list at that time.
Statistical analysis
Data are expressed as the mean ± standard deviation of the mean or number (%), unless otherwise specified. Student’s t-test was performed to analyze continuous variables with normal distributions, and the Mann-Whitney U test was conducted for non-normal continuous variables. Categorical variables were analyzed using the χ2 test or Fisher’s exact test. Cox proportional hazard regression modeling was used to examine clinical factors that affected waitlist mortality, time to transplant, and 1-year post-transplant mortality. The probability of transplantation for patients on the waitlist was estimated with the K-M method and compared using the generalized Wilcoxon test. A forest plot shows the hazard ratio (HR) and 95% confidence intervals associated with variables considered in the multivariate Cox regression analysis. All statistical analyses were performed using R software, version 3.0.1 (R Foundation, Vienna, Austria; http://www.R-project.org). All tests were two-sided, and P values < 0.05 were considered statistically significant.
Ethics statement
Data were obtained from the Korean Network for Organ Sharing. This study was approved by the Institutional Review Board of Pusan National University Yangsan Hospital (approval number: 05-2022-059). The requirement for informed consent from patients was waived because this study was observational research that used anonymized data.
RESULTS
Registrations
The study cohort comprised 1,671 patients who were registered between September 2009 and December 2020 and were categorized as group A (n = 121, 7.2%), group B (n = 111, 6.6%), group C (n = 821, 49.1%), and group D (n = 618, 37.0%, Table 1).

Table 1
Distribution of registrations according to disease group
| Status at registration | Disease group | |||
|---|---|---|---|---|
| A | B | C | D | |
| 0 | 14 (11.6) | 24 (21.6) | 140 (17.1) | 283 (45.8) |
| 1 | 46 (38.0) | 38 (34.2) | 357 (43.5) | 150 (24.3) |
| 2, 3, 4 | 61 (50.4) | 49 (44.1) | 324 (39.5) | 185 (29.9) |
All data are presented as number (%).
Group A (chronic obstructive pulmonary disease, bronchiectasis, cystic fibrosis, and lymphangioleiomyomatosis), group B (primary pulmonary hypertension and Eisenmenger), group C (idiopathic pulmonary fibrosis, sarcoidosis, asbestosis, and bronchiolitis obliterans syndrome following transplant), and group D (all other lung diseases).
Patients with status 0 were defined as those who required mechanical ventilation or extracorporeal membrane oxygenation (highly urgent status). Patients with status 1 (urgent status) were defined as having one or more of the following conditions: 1) NYHA IV and PaO2 < 55 mmHg on arterial blood gas test measured without oxygen administration, 2) NYHA IV and mean pulmonary arterial pressure > 65 mmHg or mean right atrial pressure > 15 mmHg, and 3) cardiac index < 2 L/min/m2.
NYHA = New York Heart Association.
![]()
Transplants
Overall, 836 (50.0%) of the 1,671 registered patients received transplanted at the time of data extraction. The transplant rate differed across the disease groups (P < 0.001). Specifically, 62% (n = 75) of patients in group A were transplanted, followed by 53.2% (n = 437) in group C, 48.1% (n = 297) in group D, and 24.3% (n = 27) in group B. The distribution of transplants performed at status 0 in each disease group was significantly different (P < 0.001, Table 2).

Table 2
Distribution of transplants by disease group
All data are presented as number (%).
Group A (chronic obstructive pulmonary disease, bronchiectasis, cystic fibrosis, and lymphangioleiomyomatosis), group B (primary pulmonary hypertension and Eisenmenger), group C (idiopathic pulmonary fibrosis, sarcoidosis, asbestosis, and bronchiolitis obliterans syndrome following transplant), and group D (all other lung diseases).
Patients with status 0 were defined as those who required mechanical ventilation or extracorporeal membrane oxygenation (highly urgent status). Patients with status 1 (urgent status) were defined as having one or more of the following conditions: 1) NYHA IV and PaO2 < 55 mmHg on arterial blood gas test measured without oxygen administration, 2) NYHA IV and mean pulmonary arterial pressure > 65 mmHg or mean right atrial pressure > 15 mmHg, and 3) cardiac index < 2 L/min/m2.
NYHA = New York Heart Association.
![]()
Waitlist outcomes
Data from 1,611 patients were used to analyze 1-year post-registration outcomes, which were classified as transplanted (46.1%, n = 743), still awaiting (21.1%, n = 340), removed (0.9%, n = 15), and death on waitlist (31.8%, n = 513). The cumulative incidence of transplantation and death within 1 year of registration is presented in Fig. 2. The annual outcomes according to the year of registration are shown in Supplementary Fig. 1. No significant difference was observed in the transplant rate according to the year of registration. However, significant differences were found in the waitlist mortality rates (P = 0.008) and the still awaiting rates (P = 0.009). The rate of transplantation within 1 year of registration in each disease group was significantly different (P < 0.001, Table 3). Furthermore, the rate of death within 1 year of registration in each disease group was significantly different (P < 0.001).
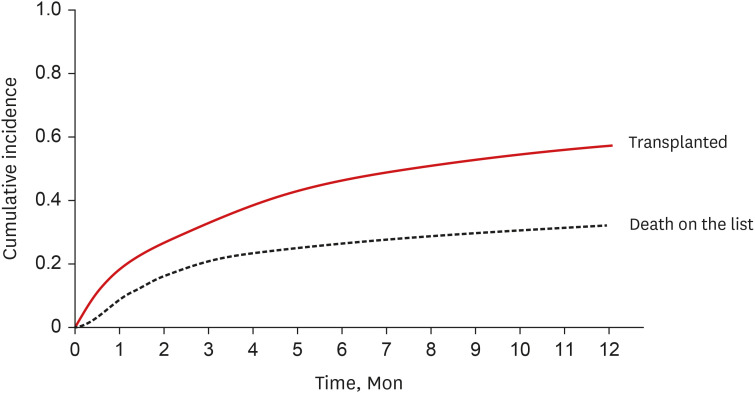

Fig. 2
Cumulative incidence of transplantation and death within 1 year of registration for the overall cohort. The red solid line represents the cumulative incidence of transplantation, and the black dotted line represents the cumulative incidence of death over time.
![]()
Table 3
Post-registration outcomes at 1 year according to disease group
All data are presented as number (%).
Group A (chronic obstructive pulmonary disease, bronchiectasis, cystic fibrosis, and lymphangioleiomyomatosis), group B (primary pulmonary hypertension and Eisenmenger), group C (idiopathic pulmonary fibrosis, sarcoidosis, asbestosis, and bronchiolitis obliterans syndrome following transplant), and group D (all other lung diseases).
![]()
Regarding blood type, patients with blood type AB had a greater chance of transplantation than those with other blood types. The possibility of lung transplantation varied significantly among patients with the various blood groups (Fig. 3, χ2: 66.45, P < 0.001). Patients with blood group O had a longer wait time for transplant than patients with other blood types (P < 0.001). They also had the highest waitlist mortality compared to patients with all other blood types (P < 0.001, Table 4).
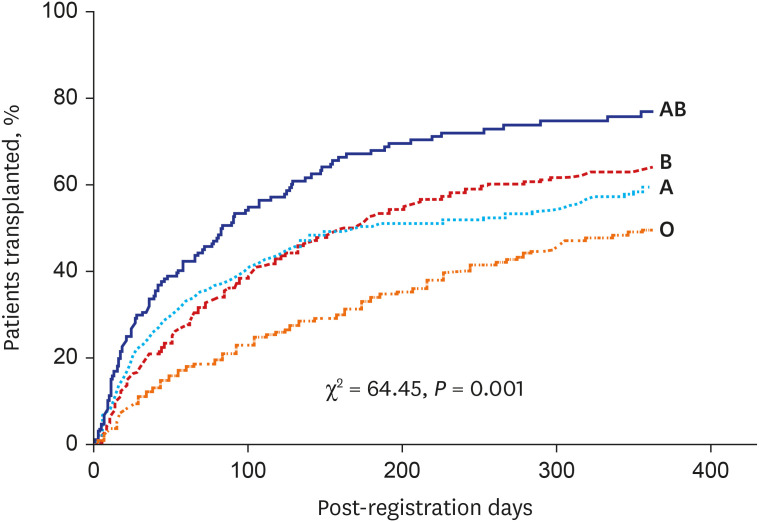

Fig. 3
Cumulative incidence of transplantation by blood group. The possibility of lung transplantation varied significantly among patients with the various blood groups (generalized Wilcoxon test, P < 0.001).
![]()
Table 4
Post-registration outcomes at 1 year according to blood type
![]()
Regarding the age group, patients aged < 18 years had the highest waitlist mortality (41.9%, n = 49). They also had a lower chance of receiving a transplant within 1 year of registration than those in other age groups (35%, n = 41, Supplementary Table 1).
Time to transplant
The clinical factors found to significantly affect the time to transplant are shown in Fig. 4 and Supplementary Table 2. Patients in disease groups B (P < 0.001) and D (P = 0.011) had significantly lower chances of transplantation than those in the other disease groups. Patients aged < 18 years (P = 0.014) and those > 65 years (P = 0.003) had significantly lower chances of transplantation. Patients with statuses 0 and 1 had significantly higher chances of transplantation than those with other urgency statuses (P < 0.001).
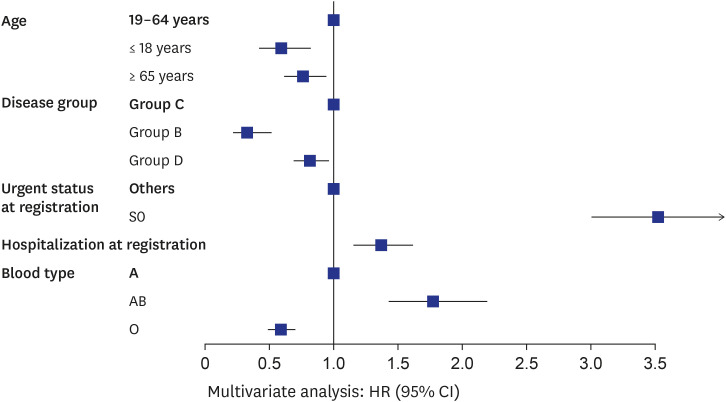
Fig. 4
Pre-transplant factors associated with time to transplant. A forest plot shows the HR and 95% CIs associated with variables considered in the multivariate Cox regression analysis. Patients aged < 18 years (HR, 0.66, P = 0.014), those > 65 years (HR, 0.73, P = 0.003), group B disease (HR, 0.33, P < 0.001), group D disease (HR, 0.81, P = 0.011), S0 at registration (HR, 4.73, P < 0.001), S1 at registration (HR, 2.02, P < 0.001), blood type AB (HR, 1.81, P < 0.001) and blood type O (HR, 0.60, P < 0.001) were significantly associated with time to transplantation.
HR = hazard ratio, CI = confidence interval.
![]()
Waitlist mortality within 1 year
The variables found to be significantly associated with the time to death are shown in Fig. 5 and Supplementary Table 3. Three factors were found to be significantly associated with waitlist mortality within 1 year of registration; in particular, patients aged > 65 years (HR, 1.48, P < 0.001) and those with status 0 at registration (HR, 2.10, P < 0.001) were more likely to die while on the list. Whereas patients with group A disease (HR, 0.36, P < 0.001) were less likely to die while on the list.
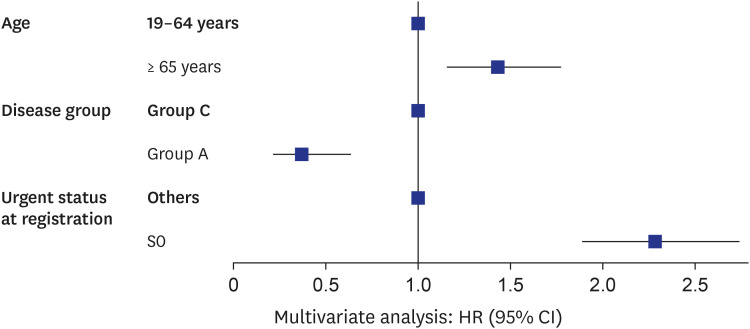
Fig. 5
Pre-transplant factors associated with waitlist mortality. A forest plot shows the HR and 95% CIs associated with variables considered in the multivariate Cox regression analysis. Patients aged > 65 years (HR, 1.48, P < 0.001), status 0 at registration (HR, 2.10, P < 0.001), and patients with group A disease (HR, 0.36, P < 0.001) were significantly associated with waitlist mortality.
HR = hazard ratio, CI = confidence interval.
![]()
DISCUSSION
This study describes the outcome of the lung transplant waitlist and the factors associated with the allocation and waitlist mortality in Korea. Within 1 year of waitlist registration, approximately half of the patients (46.1%) underwent transplantation, and 31.8% of patients died without receiving a lung transplant. IPF was the most common underlying disease in group C. In group C, half of the patients received a transplant while one-third died on the waitlist within 1 year of registration. The waitlist mortality rate in Korea appears to be higher than that in other countries. It was significantly associated with age, disease category, and urgency of registration.
In this study, the outcome of the waitlist in Korea was poor compared with that of the US or UK but similar to that of Japan.111213 In the US, 71.7% of patients ultimately received a transplant, and 14.4% of adult patients died or were removed from the waitlist for becoming too sick to undergo a transplant.11 In the UK, 45% of patients received a transplant within 1 year and 17% died while on the waitlist within 1 year.12 However, in Japan, 37% of patients received a transplant while 36.1% died on the list; this is comparable to our data.13 There are potential reasons for these inter-country differences. First, the donor pool varies with cultural background and laws regarding organ donation. In far East Asia, people are reluctant to donate their organs because of the cultural and ethical background of Confucianism.14 In addition, Korea has a high percentage of marginal donors and a relatively low utilization rate.3 Second, the efficiency of the organ allocation system could be one of the reasons for the poor outcome of the waitlist.15 Third, differences may exist depending on the time of recipient registration.16
In 2005, the US developed a revised system for lung allocation, moving from a time-based system to one that combined medical urgency and transplant benefits to reduce waitlist mortality.4 The LAS system reduces the wait time to transplant, increases transplantation opportunities, and reduces waitlist mortality without compromising post-transplant outcomes.517 In the UK, prior to 2017, donor lung allocation to patients on the lung transplant waitlist was at the discretion of the transplant center where they were listed based on clinical assessment. With the recent introduction of a super-urgent lung allocation scheme and the urgent lung allocation scheme in the UK, patients at high risk of death without a lung transplant are prioritized at the national level.18 In Japan, lung allocation was previously dependent on waiting time; however, it has recently been changed to an urgency-based system owing to an increase in waitlist mortality.13 In the previous wait-time-based system, the waiting time was extremely long, and patients with fibrosis had greater mortality rates. In Korea, the current system selects recipients based on urgency, but the waitlist mortality is still greater than that in other countries. This may be owing to high registration rates at the highly urgent status, such as MV or ECMO (27.5%) compared to those of other countries (US < 10%) and donor shortage.919
In urgency-based systems, transplants of patients with status 0 are prioritized, and the proportion of highly urgent recipients is likely to grow.10 In Korea, half of the patients on the waitlist have IPF or other interstitial lung diseases; they are at risk of rapid deterioration or are highly urgent.2021 Another potential reason is that the Korean Society of Lung Transplantation is still in the learning phase.2223 Lack of awareness among patients and/or their physicians about lung transplantation may delay referral to transplant centers. The general population need to be educated regarding lung transplantation and specialists dealing with respiratory diseases and medicine. Modifying the allocation system will help reduce waitlist mortality and provide equal opportunities for transplants.
In this study, patients aged < 18 years were less likely to undergo transplantation. In particular, they were more likely to die within 1 year of transplantation than other patients. This is consistent with observations made in the US. The current US system is unfavorable to children; therefore, this cohort has higher waitlist mortality compared with their older counterparts.11 Despite the advent of novel surgical techniques to transplant larger organs into smaller thoracic cavities, pediatric patients are still affected by size restrictions, and some pediatric patients are limited to pediatric organ donors.15 Therefore, a more efficient allocation system should be set up to ensure maximum transplantation opportunities for pediatric patients.
The number of lung transplant candidates in Korea has been increasing annually. The rapid transition from the early to mature period of the national lung transplant program raises many issues around the priority of the waitlist. To mitigate related issues, the current status of lung transplant allocation and the performance of existing waitlist systems should be regularly investigated. This study showed that the Korean allocation system has some characteristics of high waitlist mortality in specific disease groups, blood types, and pediatric groups. None of these issues will be resolved with the revision of the allocation system because the causes are multifactorial and mostly due to donor shortages. However, regular follow-up of the performance of the allocation system, including waitlist and post-transplant outcomes, is required to improve the national lung transplant program. This will provide meaningful data for initiating and activating behavior for quality improvement of the national allocation system.
 XML Download
XML Download