

 PDF
PDF Citation
Citation Print
Print



Introduction
Children’s health is an important theme in public health since its impact
covers the life-course from childhood to adulthood. Children have a unique
vulnerability to health-related issues and harmful exposures compared to adults
[1,2]. Since young children go through rapid growth and development, their
metabolism is immature and more vulnerable to environmental stressors [2]. Environmental exposures affect
children’s health and create a larger burden of diseases, including
respiratory diseases (e.g., acute lower respiratory infection [ALRI], pneumonia, and
asthma) [1,3,4]. Environmental exposure is
known as an important determinant of health in both developed and developing
countries, although the patterns of exposure vary [3]. Existing literature discusses the effect of environmental exposure
on children’s health, which causes a larger burden of diseases [4]. Previous epidemiological studies have
reported the association between air pollution exposure and mortality in children
under 5 years [5–8]. Health risks caused by air pollution have a great impact in
low- and middle-income countries [3,9]. People in wealthier nations may be healthier
since economic prosperity allows them to spend more on personal health, leading to
better health outcomes [10]. However,
economic development has led to a higher level of environmental pollution which
damages people’s health [11]. We thus
argue that environmental exposure is an important determinant of health.
Another body of literature emphasizes the importance of epigenetic modifications
caused by environmental stressors such as air pollutants, particulate matter, and
metal exposure, thereby affecting children’s health [12–14].
Epigenetic change considers genetics as a factor but puts greater emphasis on
environmental circumstances that modify one’s health [14]. A comparative study of the Republic of Korea (hereafter
referred to as South Korea) and the Democratic People’s Republic of Korea
(hereafter referred to as North Korea) presents a unique opportunity to compare the
effects of a shared genetic background versus epigenetic modifications caused by
environmental stressors [12,13].
There are few empirical studies on North Korean children’s health, despite the
ample media reports of widespread malnutrition and infectious diseases. South Korea
and North Korea have been isolated from each other due to the politics of the Korean
War and the Cold War dynamics on the Korean Peninsula. Such separation from each
other while sharing the same ethnicity and early history provides a rich ground for
comparative research. However, there are few comparative studies on
children’s health in these two countries. There are two pertinent points of
comparison in this research. First is the impact of the “North Korean Famine
(1995–1998)” or “the Arduous March,” which has resulted
in children’s widespread malnutrition and stunting. South Korea did not
suffer from famine or malnutrition during the same period. A second point is the
remarkably different environmental circumstances due to the different pace and level
of economic development.
South Korea and North Korea have been divided since 1945 and their division has
solidified after the Korean War in 1950–1953 [15]. Over 7 decades, they have experienced different political regimes
and socio-economic development. We assume that the health status of children is
conspicuously different between South Korea and North Korea due to socioeconomic,
cultural, and environmental factors. Based on this assumption, we hypothesize that
harmful environmental circumstances exacerbate the gap in children’s health
in the two Koreas. Thus, this study aims to analyze the differences in
children’s health status and the correlation between the environment and
children’s health in South Korea and North Korea to answer three research
questions: (1) How different is the general status of children’s health
between South Korea and North Korea, and how has the gap changed over time? (2) What
are the disease patterns of children in the two Koreas? and (3) How much do the
environmental factors affect children’s health in South Korea and North
Korea? The comparative analysis will provide interesting findings since many
variables have been held constant due to the division. The comparative analysis will
help identify the patterns of, and gaps in, children’s health in South Korea
and North Korea from the perspective of environmental influences on disease patterns
across countries of varying levels of economic development.
A comparative study of children’s health in South Korea versus North Korea is
important for three reasons. First, it can provide a rich comparative analysis of
the effect of the environment on children’s health with many important health
factors held constant. Second, this study will help delineate how a developed, as
opposed to a developing, country’s environmental factors change as a result
of economic progress. Finally, it can contribute as a preparatory study to the
understanding of children’s health status of the two Koreas to prevent and
minimize social disturbances that can be caused by reunification.
Go to : 
Method
1. Data source
We used estimated data for North Korea since the country does not provide
official statistics on environmental and health measurements. We utilized data
provided by international organizations (for details of data source, see the
appendix [Table S1]). The collected (ecological) data are from 2000 to 2017 and
included two strands of indicators: (1) environmental indicators and (2)
children’s health status (mortality rate, prevalence). The collected data
were published by the World Bank and the World Health Organization (WHO) [16,17]. Environmental indicators include fine particulate matter
(PM2.5) exposure and air pollutant emissions, including gas
emissions and fossil fuels. In the supplementary material, we provide annual
population characteristics and medical and nutritional status collected from the
United Nations Children's Fund (UNICEF), Energy Information
Administration (EIA), World Bank, Organisation for Economic Co-operation and
Development (OECD), and Korea Statistical Information Service. We categorized
the indicators of children’s health status into four categories:
reproductive health, respiratory disease, chronic disease, and nutritional
disease.
2. Air pollution indicators
The annual mean PM2.5 concentration estimates were derived from the
Global Burden of Disease study [18–20]. These data are
estimates of the population-weighted average exposure and a general air quality
indication to inform cross-country comparisons of health risks. The population
estimation data are based on the Gridded Population of the World by NASA
Socioeconomic Data and Applications Center (version 4). The detailed description
of the exposure estimates is based on previous studies of global estimates of
air pollution and environmental risks [18–20]. The emission
data include carbon dioxide (CO2.5), nitrous oxide
(N2.5O), methane, and fossil fuel information.
3. Outcome indicators
Children’s health indicators consist of two types: (1) annual
children’s mortality rate (infant, stillbirth, neonatal, under-five,
ALRI), congenital anomalies, prematurity, birth asphyxia, diarrheal disease,
meningitis/encephalitis, sepsis and other infections) and (2) prevalence
(anemia, overweight, obesity, thinness). Infant mortality, stillbirth, and
neonatal mortality were calculated as deaths per 1,000 live births (0–4
years old). Mortality of under–five, ALRI, congenital anomalies,
prematurity, birth asphyxia, diarrheal disease, meningitis/encephalitis, sepsis
and other infections was calculated as deaths per 1,000 children (0–4
years old). We used data on the prevalence of anemia in children under 5 years
of age and that of overweight, obesity, and thinness in children 5–9
years of age. Here, overweight is defined as the Body Mass Index (BMI) exceeding
+1 SD above the median, obesity as the BMI exceeding +2 SD above the median, and
thinness means as a BMI is below median -2 SD.
4. Statistical analysis
We performed two analyses to examine how South Korea and North Korea are
differently situated after the “North Korean Famine” in terms of
air pollution and health status. First, we compared descriptive statistics for
South Korea and North Korea. Second, we performed trend analysis to observe how
children’s health status in South Korea and North Korea has changed over
time.
As the children’s health indicator data were estimated annually, we
focused on observing the changes per year. Overall, we considered three methods
for trend analysis of children’s health status: (1) Sen’s slope,
(2) Mann-Kendall trend test, and (3) linear regression. The first two methods
are used to analyze the trends for non-parametric data. If the beta coefficient
is greater than zero (β > 0), the data are considered to show a
positive trend. When there are many missing values, the Mann-Kendall trend test
can be used as a way to adjust missing data. This method validates significance
by using Kendall’s correlation coefficient.
We analyzed the correlation coefficient between environmental indicators and
children’s health status. Since our data spans from 2000 to 2017, the
number of pair samples for health status is 18. As the sample number is too
small to assume a specific distribution, we utilized Spearman’s
correlation based on the non-parametric method.
5. Sensitivity analysis
The sources of data in this study are international organizations. Since the data
we use are secondary, a direct comparison between the two Koreas is limited.
Thus, we cross-checked our results with the data reported by the OECD and the
South Korean government (Statistics Korea) for sensitivity analysis [21,22]. This study also extracted North Korean data from the South
Korean database (Statistics Korea).
Go to :
Results
Over a total span of 18 years (2000–2017), we found a distinct gap between
South Korea and North Korea in two domains: (1) children’s health status
(mortality rate, prevalence) and (2) environmental indicators. Differences were
observed despite similar demographic trends from 2000 to 2018 – growing
population, increase in life expectancy, decrease in total fertility rate, and aging
(Table 1).
Table 1.
Demographic characteristics of South Korea and North Korea
| Year | Population (1,000 people) | Life expectancy (yr) | Total fertility rate (births per 1,000 women) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| South Korea | North Korea | South Korea | North Korea | South Korea | North Korea | |||||
| Total | Male | Female | Total | Male | Female | |||||
| 2000 | 47,008 | 22,702 | 76.0 | 72.3 | 79.7 | 65.3 | 61.2 | 69.0 | 1.48 | 1.99 |
| 2001 | 47,370 | 22,902 | 76.5 | 72.9 | 80.1 | 66.1 | 62.1 | 69.7 | 1.31 | 1.99 |
| 2002 | 47,645 | 23,088 | 76.8 | 73.4 | 80.3 | 66.9 | 63.0 | 70.4 | 1.18 | 1.99 |
| 2003 | 47,892 | 23,254 | 77.3 | 73.8 | 80.8 | 67.6 | 63.8 | 71.0 | 1.19 | 1.99 |
| 2004 | 48,083 | 23,411 | 77.8 | 74.3 | 81.2 | 68.1 | 64.3 | 71.5 | 1.16 | 1.98 |
| 2005 | 48,185 | 23,561 | 78.2 | 74.9 | 81.6 | 68.4 | 64.7 | 71.7 | 1.09 | 1.98 |
| 2006 | 48,438 | 23,707 | 78.8 | 75.4 | 82.1 | 68.5 | 64.8 | 71.8 | 1.13 | 1.97 |
| 2007 | 48,684 | 23,849 | 79.2 | 75.9 | 82.5 | 68.7 | 65.0 | 72.0 | 1.26 | 1.96 |
| 2008 | 49,055 | 23,934 | 79.6 | 76.2 | 83.0 | 68.9 | 65.3 | 72.2 | 1.19 | 1.95 |
| 2009 | 49,308 | 24,062 | 80.0 | 76.7 | 83.4 | 69.2 | 65.6 | 72.5 | 1.15 | 1.94 |
| 2010 | 49,554 | 24,187 | 80.2 | 76.8 | 83.6 | 69.6 | 66.0 | 72.9 | 1.23 | 1.94 |
| 2011 | 49,937 | 24,308 | 80.6 | 77.3 | 84.0 | 70.0 | 66.4 | 73.3 | 1.24 | 1.93 |
| 2012 | 50,200 | 24,427 | 80.9 | 77.6 | 84.2 | 70.5 | 66.8 | 73.8 | 1.30 | 1.93 |
| 2013 | 50,429 | 24,545 | 81.4 | 78.1 | 84.6 | 70.9 | 67.2 | 74.2 | 1.18 | 1.93 |
| 2014 | 50,747 | 24,662 | 81.8 | 78.6 | 85.0 | 71.2 | 67.6 | 74.5 | 1.21 | 1.93 |
| 2015 | 51,015 | 24,779 | 82.1 | 79.0 | 85.2 | 71.5 | 67.8 | 74.9 | 1.24 | 1.92 |
| 2016 | 51,218 | 24,897 | 82.4 | 79.3 | 85.4 | 71.7 | 68.1 | 75.1 | 1.17 | 1.92 |
| 2017 | 51,362 | 25,014 | 82.7 | 79.7 | 85.7 | 71.9 | 68.3 | 75.3 | 1.05 | 1.91 |
| Average (SD) | 49,229.4 (1,394.1) | 23,960.5 (702.7) | 79.6 (2.1) | 76.2 (2.3) | 82.9 (2.0) | 69.2 (1.9) | 65.4 (2.1) | 72.5 (1.9) | 1.2 (0.1) | 2.0 (0.0) |
| Sen’s slope (95% CI) | 260.3 (253, 272.9) | 125.3 (120.0, 134.7) | 0.4 (0.4, 0.4) | 0.4 (0.4, 0.4) | 0.4 (0.3, 0.4) | 0.3 (0.3, 0.4) | 0.4 (0.3, 0.4) | 0.3 (0.3, 0.4) | 0.00 (–0.02, 0.01) | 0.00 (–0.01, –0.00) |
| Mann-Kendall statistics | 5.8 (P–value <0.001) | 5.8 (P–value <0.001) | 5.8 (P–value <0.001) | 5.8 (P–value <0.001) | 5.8 (P–value <0.001) | 5.8 (P–value <0.001) | 5.8 (P–value <0.001) | 5.8 (P–value <0.001) | –0.8 (P–value: 0.425) | –5.3 (P–value: <0.001) |
| β (Slope) (95% CI)* | 260.6 (252.5, 268.7) | 131.2 (125.9, 136.5) | 0.4 (0.4, 0.4) | 0.4 (0.4, 0.4) | 0.4 (0.3, 0.4) | 0.4 (0.3, 0.4) | 0.4 (0.3, 0.4) | 0.3 (0.3, 0.4) | 0.01 (–0.02, 0.00) | 0.00 (–0.01, 0.00) |
![]()
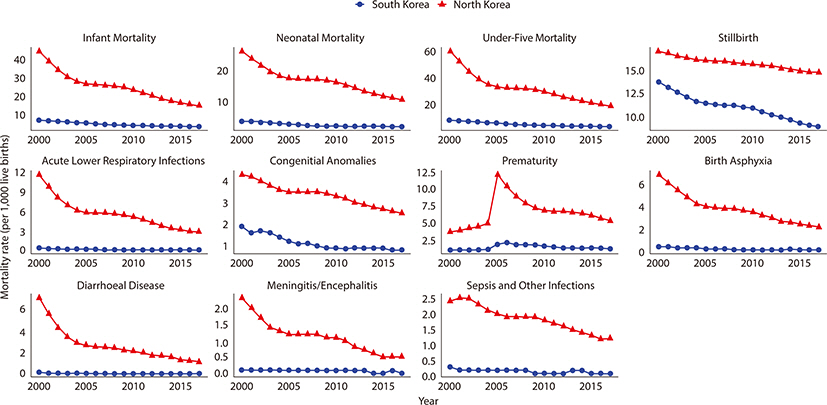
The time-plots show the trends in children’s annual mortality and prevalence
in South Korea and North Korea, respectively (Figs.
1, 2). The results of the trend
analysis are presented in the appendix (Table S2). Child mortality rates in South
Korea and North Korea are decreasing, except for prematurity. While North Korea
reported a higher death rate of children than South Korea, the gaps in
children’s mortality and their health status in both Koreas narrowed from
2000 to 2017 (Fig. 1). In particular, North
Korean children recorded a sharp decline in mortality rate indicators, especially
after 2005.
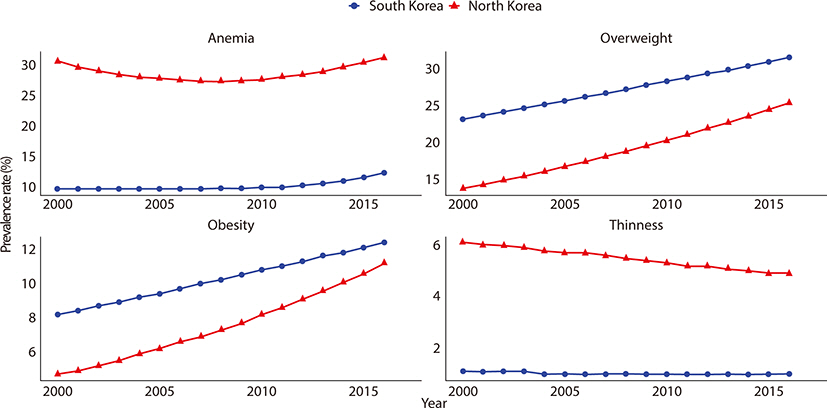
The prevalence of overweight and obesity has increased and that of thinness decreased
in both Koreas (Fig. 2). While South Korean
children showed an increasing prevalence of anemia, North Korean children decreased
and then increased again in North Korean children after 2009. For North Korean
children under the age of 5 years who had anemia, a U–shaped pattern was
observed since it decreased in the early 2000s and then increased after 2008 (Fig. 2).
We discovered differences in environmental indicators between the two Koreas. Except
for PM2.5 exposure, South Korea recorded much higher figures than North
Korea in most indicators of air pollutant emissions such as CO2.5,
N2.5O, and methane emissions (Table
2 and Fig. S1). An interesting finding is that PM2.5
concentration estimates were higher in North Korea than in South Korea. North Korea
is faced with the danger of high PM2.5 concentration which is known to
increase the risk of children’s ALRI.
Table 2.
Comparison of environmental indicators in South Korea and North Korea
![]()
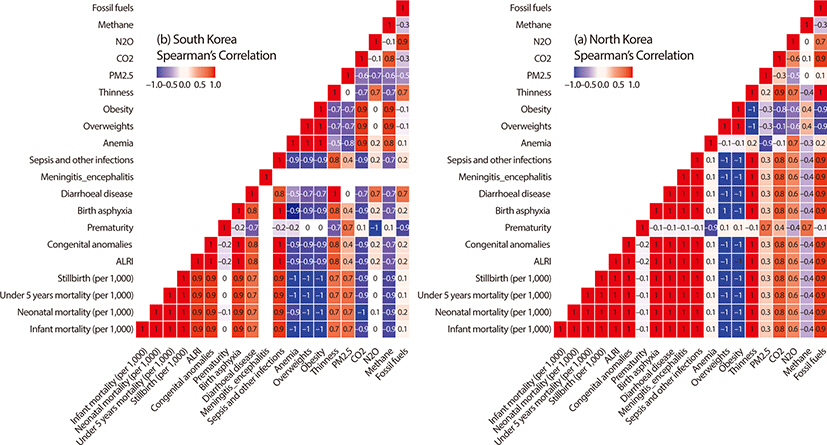
Given the differences in environmental indicators between South Korea and North
Korea, we examined the association between the environment and children’s
health. PM2.5 showed a positive relationship with infant and child
mortality indicators and a negative relationship with the prevalence of anemia,
overweight, and obesity in the two Koreas (Fig.
3). In the Poisson regression model, North Korea’s
PM2.5 exposure concentrations were related to infant mortality (%
increase: 9.07, 95% confidence interval [CI]: 3.06, 15.44), neonatal mortality (%
increase: 7.50, 95% CI: 0.52, 14.97), and under-five mortality (% increase: 8.67,
95% CI: 3.44, 14.17). Meanwhile, the correlation of CO2.5,
N2.5O, and fossil fuel emissions with health effects varied between
the two Koreas. It is positive in North Korea, while South Korea has a negative or
no correlation.
Go to :
Discussion
There is a large gap in children’s health status between South Korea and North
Korea. Children living in North Korea experienced more severe health outcomes than
those in South Korea. The death rate of prematurity, congenital anomalies, and birth
asphyxia is higher in North Korea, which indicates that newborns in North Korea are
more susceptible to these diseases than their South Korean counterparts. This trend
has continued albeit with a decreasing rate over time. The time-plot of infant
mortality rate during the North Korean famine is provided in the supplementary
appendix (Figs. S2 and S3).
While South Korea recorded higher figures in air pollutant emissions such as
CO2.5, N2.5O, and methane than North Korea,
PM2.5 concentration estimates are higher in North Korea (Table 2). Although both Koreas are affected by
air pollution, including fine particulate matters and dust flying from China, North
Korea showed a higher rate of PM2.5 concentration estimates than South
Korea. We speculate that North Korea’s use of cooking and heating fuel with
low combustion rate and low thermal efficiency, as well as low-quality coal, has
resulted in a higher exposure to PM2.5 (Fig. S4). North Korea’s
use of ineffective domestic fuel is likely to release particulate matter and
increase the level of PM2.5 concentration over that in South Korea [23]. Fossil fuels, particularly coal and heavy
oil, in thermal power plants, industrial boilers, kilns, motor cars, and households
are the major pollutants in the largest city of North Korea (Pyongyang) and in
nearby industrial districts [24].
We also found a gap in prevalence indicators between the two Koreas. The prevalence
of anemia, overweight, obesity, and thinness is lagged for estimation, and North
Korean children are faced with a greater danger of anemia and thinness while those
in South Korea experience a higher prevalence of overweight and obesity. More
interestingly, the prevalence of overweight and obesity is increasing and that of
thinness is decreasing in both Koreas. This trend in prevalence indicators is
probably caused by nutritional factors rather than air pollution. The previous study
on North Korean refugee children residing in South Korea showed that the gap in
growth (height and weight) and obesity rates between South Korean and North Korean
children was narrowed after consuming sufficient food [25]. The nutritional status of South Korean and North Korean is
provided in the appendix (Table S3 and Fig. S5). It implies that poor nutritional
intake in North Korea has led to the children’s malnutrition causing anemia
and thinness, while the higher prevalence of overweight and obesity in South Korea
is most likely caused by a Westernized dietary pattern, which contains high amounts
of saturated fatty acids and energy-dense foods that are poor in micronutrients.
The differences in environmental indicators such as air pollutant emissions between
South Korea and North Korea created gaps in the children’s health status. The
higher emissions of environmental pollutants, including PM2.5, serve as a
trigger for increasing the incidence of respiratory diseases (ALRI, pneumonia, and
asthma) [4]. This relationship was supported
by another study showing that long-term exposure to ambient fine particulate matter
(PM2.5) is inversely associated with lung function in children,
adolescents, and young adults [26]. In
addition to air pollutants, lead is more noxious to children than adults [27]. In particular, anemia is observed in young
children who have lead poisoning [27]. Iron
deficiency anemia is a risk factor for lead toxicity, as it not only promotes pica
behavior but also increases the absorption of lead from the gastrointestinal tract
[28]. Lead exposure and nutritional
deficiencies, which are prevalent in North Korea, put children in danger of growth
retardation and behavioral challenges. For instance, the active use of inefficient
cooking and heating fuel such as a tire close to the furnace increases the level of
lead exposure among North Korean children. North Korean children have a higher risk
of respiratory infections caused by indoor air pollution from low-quality fuels.
Further, this study found an interesting pattern in diseases between South Korea and
North Korea. The two Koreas have been isolated from each other since 1945, sharing
the same ethnicity and similar genetic characteristics (Fig. S6). The different
environmental circumstances for over 7 decades since the division have led to very
different disease characteristics. North Korean children suffer from infectious
diseases such as parasite infection, tuberculosis, lower respiratory tract
infections, acute infectious diarrhea, malaria, meningitis, and sepsis. Infectious
diseases are prevalent in North Korea due to poor conditions – pollution of
drinking water (Figs. S7 and S8), weak management of vaccination, and unavailability
of antibiotics. In contrast, pediatric allergic, autoimmune, and metabolic diseases
are prevalent among South Korean children. The so-called “hygiene
hypothesis” explains this by assuming that microbes such as bacteria
stimulate the immune response and the too-clean environmental and hygienic
conditions decrease immunity so that people can be more susceptible to allergies and
autoimmune diseases [29,30]. As immune polarization caused by different environmental
stressors exists in South Korea and North Korea, the disease patterns are different
[14,31,32]. The disease pattern of
North Korean children is similar to that of developing countries, whereas the
disease pattern of South Korean children is similar to that of developed countries,
as illustrated in the appendix based on the mortality rate and prevalence of each
disease (Figs. S9–S12).
This study offers two key contributions. First, the study examines the gap in
children’s health between South Korea and North Korea, explores the
association between the environment and children’s health, and finds the
disease patterns of South Korea and North Korea to be similar to the differences
found between developed and developing countries. While there have been few studies
comparing the children’s health status between South Korea and North Korea,
this study empirically highlighted the differences and patterns of children’s
health, which helps to fill the lacunae in the children’s health studies.
Second, this study is meaningful in that it compared children’s health status
and environmental circumstances between South Korea and North Korea after the two
were forcibly divided in 1945 and further distanced by a war between the two in
1950¬–1953. The two countries in the Korean Peninsula provide an
interesting test-bed for a rich comparative analysis as a social experiment to
examine how South Korea and North Korea have evolved for over 7 decades since the
division in terms of the environment and children’s health.
Our findings should be interpreted, however, in light of data limitations. First,
official data on North Korean health, environment, or nutrition are not available.
Therefore, we used data collected from multiple international organizations
including the World Bank and WHO. Second, we cannot determine a direct relationship
between air pollution exposure and health effects in South Korea and North Korea due
to data constraints. To overcome this, we conducted comparative and trend analyses.
The differences in mortality and morbidity of children in the two Koreas might be
caused by socioeconomic and cultural factors, as well as environmental factors.
Thus, it would be necessary to secure national data for precise research to improve
North Korean children’s health. Therefore, more reliable data sources
representing a larger sample or that enable longitudinal studies such as cohort
studies are needed. Third, it is difficult to access prevalence indicators since
their availability is limited compared to mortality indicators. Lastly, the dataset
does not consider regional disparities within North Korea. It would be important to
identify regional differences to help reduce the health status gaps among different
regions.
Considering the patterns and gaps in children’s health between South Korea and
North Korea, more attention and resources need to be directed towards North Korea.
The current health status of North Korean children needs intensive international
development cooperation because the necessary commodities and services to improve
the health of children are lacking in North Korea (Fig. S13). Although the
governments of South Korea and North Korea have not had a Summit since 2018, there
is hope that future official summits between South Korea and North Korea, and with
other countries including the US could open doors for cooperation and unification.
Should North Korea become open to international development cooperation, South Korea
can play an important role in assisting North Korea although its assistance cannot
be counted toward foreign aid as the two do not recognize each other as separate
countries. Nevertheless, South Korea’s shared ethnicity, language, culture,
and geographical proximity would be very useful to assist the international efforts
for development cooperation in North Korea.
These findings imply that epigenetic modification resulting from environmental
stressors has had an impact on children’s health in South Korea and North
Korea despite sharing similar genetic backgrounds. After the division of the Korean
Peninsula, different environmental circumstances modified children’s health
in the two Koreas, with genetics held constant. Considering the effect of epigenetic
modification caused by environmental factors, it would be vital to develop a
strategy for improving public health, especially targeting North Korean children if
and when unification occurs. In particular, there is a danger that infectious
diseases can spread quickly in South Korea and North Korea since people across the
Korean Peninsula have not been exposed to each other for a long time. It is likely
that infectious diseases such as measles, tuberculosis, malaria, and parasite
infection, which are common in North Korea, can spread to South Korea, while other
infectious diseases and socially driven illnesses from South Korea can spread to
North Korea [33]. As South Korea established
a relatively stronger health infrastructure than North Korea (Table S4), advances in
the health care system can contribute to reducing the mortality rate. Thus, access
to optimal management and referral systems at the primary care level, stable supply
of nutrients, and removing economic barriers in North Korea would be crucial. Based
on the children’s disease patterns of South Korea and North Korea found in
this study, it is projected that infectious diseases will become more prevalent if
we do not have preventive measures. Given the significant differences in
children’s health between South Korea and North Korea which have persisted
for more than 7 decades, it is imperative to bridge this gap.
Go to :
 XML Download
XML Download