

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
According to the World Health Organization data, between 2020 and 2040, the incidence of colorectal cancer is estimated to increase by 120% among individuals aged over 65 years in the Republic of Korea [1]. Consequently, the number of elderly patients requiring colorectal cancer surgery is expected to increase. Usually, the elderly are defined as people aged 65 years or older [2]. Frailty is defined as a condition of increased vulnerability to acute and chronic stressors, including an increased risk of disability, dependence, need for long-term care, and mortality, as a result of a significant decrease in physiological reserves [3]. Frail elderly patients with colorectal cancer who have undergone surgery are more likely to have longer hospital stays; higher rates of postoperative complications, including delirium, pneumonia, and urinary tract infection; and higher mortality rates than younger patients [345]. Therefore, elderly patients require accurate preoperative evaluations and individually tailored treatment plans.
Comprehensive geriatric assessment (CGA) is a multidimensional, interdisciplinary diagnostic process focused on medical, psychological, physical, functional capability, and social characteristics. CGA is used to detect vulnerability and assess geriatric conditions that may be associated with frailty [6]. Because preoperative CGA can identify frail elderly patients who are at risk of mortality, postoperative complications, institutionalization after discharge, and prolonged length of hospital stay, CGA can help in surgical decision-making in frail elderly patients [7]. In addition, the multidimensional frailty score (MFS) based on CGA is more useful than the American Society of Anesthesiologists physical status classification in predicting mortality and postoperative complications in elderly patients undergoing surgery [8].
It is difficult for a surgeon to establish a treatment plan alone because multiple subject domains must be considered in elderly patients with colorectal cancer. Through a geriatric multidisciplinary oncology clinic (GMOC), including radiation oncologists, medical oncologists, radiologists, geriatricians, and coordinating nurses, it is possible to comprehensively evaluate and establish proper treatment plans to provide tailored treatment to elderly patients [9]. However, no study has analyzed the factors that relate to the decision to undergo surgery for elderly patients in the GMOC, and the corresponding patient survival outcomes. Thus, this study aimed to evaluate the clinical efficacy of a GMOC by analyzing the surgical treatment decision-making process and outcomes.
METHODS
This retrospective chart review study involving human participants was in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The Institutional Review Board of Seoul National University Bundang Hospital approved this study (No. B-2201-733-105), and the need for informed consent was waived.
Patients
From 2015 to 2021, 165 elderly patients visited the GMOC at a tertiary referral hospital comprehensive cancer center. Of these patients, we analyzed 74 patients who had colorectal cancer.
Geriatric multidisciplinary oncology clinic
The GMOC makes decisions with patients and their families based on CGA, MFS data, and expert opinions. The GMOC held weekly meetings to discuss elderly patients who met with surgeons, radiation oncologists, medical oncologists, radiologists, and geriatricians to establish a treatment plan. In each department, the decision about the type of treatment to be given to elderly patients with colorectal cancer was marked as a “decision,” and the treatment plan decided upon after the GMOC meeting was marked as a “recommendation.” When a patient actually underwent the treatment, it was marked as “actually performed.” The clinical adherence rate was defined as the ratio of “actually performed” to “decision.”
Comprehensive geriatric assessment
CGA is a systematic assessment tool for geriatric patients, including comorbidities, physical function, nutrition, polypharmacy, psychological status, and risk of postoperative delirium [7]. Comorbidities were estimated using the Charlson comorbidity index (CCI), consisting of 19 comorbidity categories; weights were assigned to each category based on the adjusted relative risk of 1-year mortality, and all individual weights were summed to calculate a single comorbidity score for each patient [10]. Physical function was evaluated based on activities of daily living (ADL) and instrumental ADL (IADL). ADL was evaluated using the modified Barthel Index, which includes 10 subscales: grooming, eating, bathing, toilet use, dressing, fecal and urinary continence, walking in a hallway, and the ability to go up and down stairs [11]. IADL was evaluated using the Lawton and Brody index, which includes 5 subscales for men: shopping, ability to use a telephone, responsibility for own medication, traveling via public transportation or car, and financial management. For women, 3 additional items were also included (housekeeping, food preparation, and laundry) [12]. Nutrition was assessed using the Mini Nutritional Assessment (MNA), with scores ranging from 0 to 30; scores below 17 indicated malnutrition [13]. A diagnosis of polypharmacy was determined through a thorough medical review and detailed history of the patient. Polypharmacy was defined as taking more than 5 medications regularly, and inappropriate medications were determined using the Beers criteria [14]. The Mini-Mental State Examination in the Korean version of the Consortium to establish a registry for Alzheimer’s disease assessment packet (MMSE-KC) was used to evaluate psychological status, with scores ranging from 0 to 30. Scores ranging between 17 and 24 indicate mild cognitive impairment, whereas those less than 17 indicate dementia [15]. To screen for depressive symptoms, a short form of the Korean Geriatric Depression Scale was used to score between 0 and 15; a score of 10 or higher was considered severe depression [16]. The Nursing Delirium Screening Scale, with scores ranging from 0 to 5, was used to assess the risk of postoperative delirium. A score of ≥2 indicates an increased risk of postoperative delirium [17].
Multidimensional frailty score
The MFS consists of 9 items: malignant disease, CCI, albumin, ADL, IADL, MMSE-KC, risk of delirium, MNA, and midarm circumference. Each item is scored from 0 to 2, and patients are classified into the high-risk group when 5 points are exceeded. This is more useful for predicting the outcome of geriatric patients undergoing surgery than conventional methods [8].
Outcome measures
The factors that influenced the recommendation for surgery at GMOC were analyzed. In local diseases, we compared the 1-year survival outcomes of the groups that recommended surgery and those that did not recommend surgery, as well as those who underwent surgery and those who did not undergo surgery. In the group that underwent surgery, we analyzed the operation time, estimated blood loss, hospital stay, postoperative complications, and readmission within 30 days.
Statistical analysis
Categorical variables are presented as numbers (percentages) and continuous variables as medians (interquartile ranges, IQRs). Fisher exact test or the chi-square test was used to compare categorical variables, while the Mann-Whitney U-test was used to compare continuous variables. The 1-year overall survival (OS) was calculated using the Kaplan-Meier analysis. The OS was calculated from the date of diagnosis to the date of death. Statistical significance was set at P < 0.05. All statistical analyses were performed using MedCalc ver. 20 (MedCalc Software, Ostend, Belgium) and IBM SPSS Statistics ver. 22 (IBM Corp., Armonk, NY, USA).
RESULTS
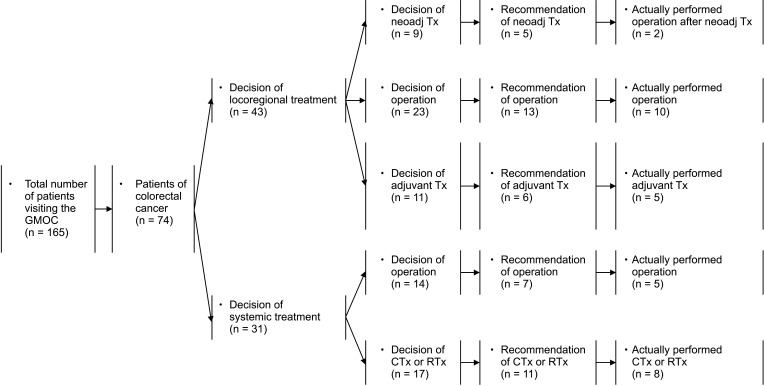
A total of 165 geriatric patients with cancer visited the GMOC, and 74 had colorectal cancer (mean age, 85.5 years [range, 81.2–89.0 years]; 39 males [52.7%]). There were 43 (58.1%) and 31 patients (41.9%) with locoregional and systemic diseases, respectively. The clinical adherence rate to the medical recommendations for all patients was 40.5% (30 of 74). The treatment plans for locoregional diseases were divided into neoadjuvant chemotherapy followed by surgery (n = 9), surgery (n = 23), and chemotherapy (n = 11). Among the surgical candidates, 18 patients (56.2%) were recommended for surgical treatment through the GMOC, and finally, 12 (37.5%) underwent radical surgery. Treatment plans for systemic treatment were divided into surgery (n = 14) and chemotherapy (n = 17); 7 patients (50.0%) were recommended for surgical treatment, and finally, 5 (35.7%) underwent palliative surgery (Fig. 1).
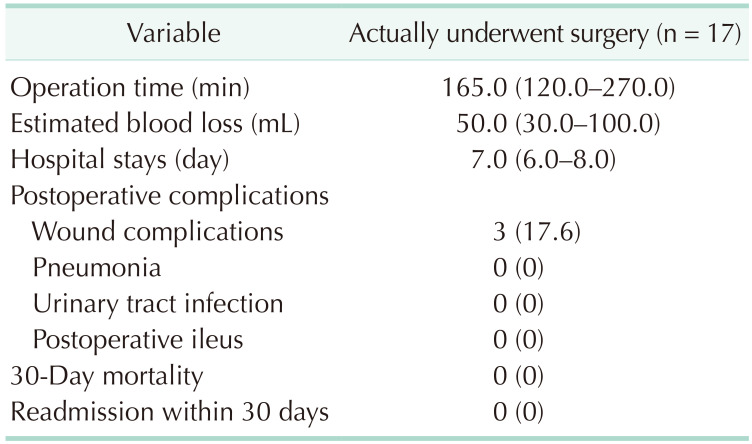
Of the 46 patients considered for surgical treatment, 25 who were recommended for surgery and 21 who were not recommended for surgery were analyzed in the 2 groups. The median age of the groups recommended and not recommended for surgery was >80 years. There were no differences in baseline characteristics (Table 1). However, ADL (P = 0.024), IADL (P = 0.001), MMSE-KC (P = 0.014), delirium risk (P = 0.039), and MFS (P = 0.001) differed between the 2 groups (Table 2). Among the 17 patients who underwent surgery, the median (IQR) of operation time was 165.0 minutes (120.0–270.0 minutes), estimated blood loss was 50.0 mL (30.0–100.0 mL), and hospital stay was 7.0 days (6.0–8.0 days). Only 3 patients had wound complications after surgery, and there was no other anastomotic leakage, intestinal obstruction or ileus, 30-day mortality, or readmission within 30 days (Table 3).
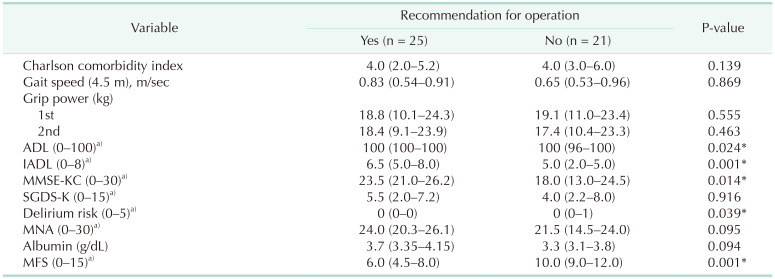
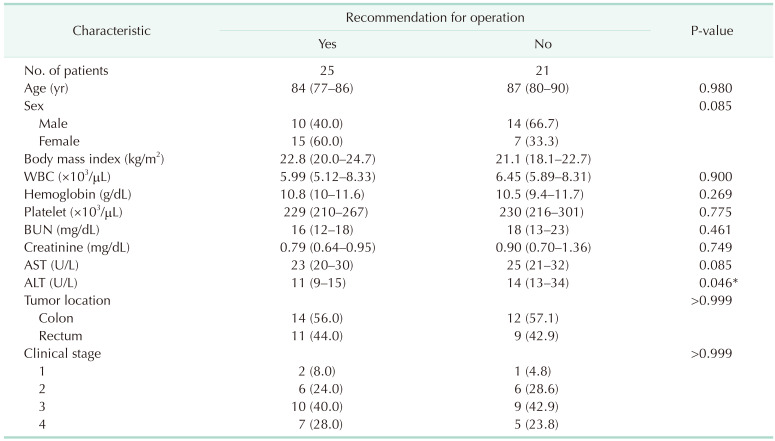
Table 2
Comprehensive geriatric assessment and multidimensional frailty score influencing the recommendation for surgical treatment
Values are presented as median (interquartile range). Missing values are excluded.
ADL, activities of daily living; IADL, instrumental activities of daily living; MMSE-KC, Mini-Mental State Examination in the Korean version of the Consortium to Establish a Registry for Alzheimer’s Disease Assessment Packet; SGDS-K, Korean version of the short form of the Geriatric Depression Scale; MNA, Mini Nutritional Assessment; MFS, multidimensional frailty score.
a)Those in parentheses indicate the range of scores on the questionnaire.
*P < 0.05, statisticaly significant.
![]()
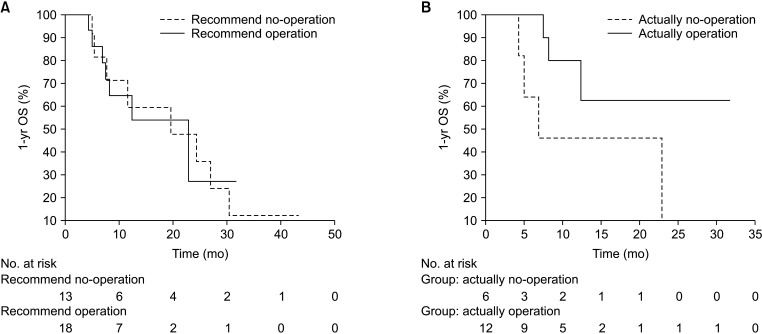
In the locoregional treatment group, the 1-year OS of patients who were recommended for surgery (n = 18) was not different from that of those who were not recommended for surgery (n = 14, P = 0.980), and there was no difference between the group that underwent surgery (n = 12) and the one that did not (n = 6, P = 0.109) (Fig. 2).
DISCUSSION
This is one of a few studies to objectively evaluate CGA and MFS in elderly patients with colorectal cancer, select surgical treatment through GMOC, analyze the results, and report on the effectiveness of GMOC. Elderly patients with colorectal cancer who received a recommendation for surgery through the GMOC had significantly different physical functions, psychological functions, and MFS compared with those of patients who did not receive a recommendation for surgery. There was no statistically significant difference in the 1-year OS between the 2 groups. However, the group that underwent surgery tended to have higher survival rates. Postoperative complications, such as anastomotic leakage, bleeding, and perforation, were not observed, and the only problem was wound healing. The hospital stay was no longer, and there were no 30-day readmissions or mortalities. Therefore, if surgical treatment is selected for frail elderly patients through the GMOC, favorable postoperative results can be obtained.
It is difficult to make surgical decisions in frail elderly patients because of the heterogeneity of their health status and the lack of tools available to predict the risks of surgery. The most commonly used postoperative complication predictors have considerable limitations, most of which are based on a single organ system, and none are based on a patient’s physiological reserve [7]. However, the American Geriatrics Society and the American College of Surgeons National Surgical Quality Improvement Program jointly released best-practice guidelines for the optimal perioperative care of geriatric patients [18]. In addition, the recent National Comprehensive Cancer Network and American Society of Clinical Oncology clinical guidelines recommend the use of CGA in elderly patients [1920]. CGA is important because it can be used to predict complications following surgery [7]. Cognitive impairment may also contribute to increased risks for postoperative delirium [21]. Elderly patients with severe comorbidities, impaired IADL, depression, and malnutrition are associated with postoperative complications and mortality [22]. MFS based on CGA is more useful than conventional methods for predicting postoperative complications and mortality [8].
The GMOC plays a key role in optimizing patient outcomes and providing tailored care for each individual patient. In elderly patients, colorectal cancer requires a combination of treatments, including radiation therapy, chemotherapy, and surgery; therefore, multidisciplinary collaboration is needed to determine treatment options. Furthermore, survival is not the primary outcome of concern, and remaining independent is often more significant [23]. The GMOC can reduce the number of incomplete decisions that are made by individual physicians, and treatment policies have been changed in more than 10% of cases [24]. Furthermore, it has been shown that the number of complications and length of hospital stay are reduced [25]. The process of evaluating a patient takes some time, and there is also time spent in decision-making in the GMOC. However, it is preferred by the GMOC and patients, and making optimal treatment decisions can improve patient outcomes and avoid worse outcomes [26].
This study has a few limitations. First, it was a retrospective, single-institution study, and there was unavoidable selection bias. Second, there was no difference in survival outcomes between the group that was recommended for surgery and the group that was not recommended for surgery through the GMOC because the recommended group included patients who did not undergo surgery. Among the groups that were recommended for surgery, when comparing the group that actually underwent surgery to the group that did not, the survival rate was not statistically significant, but the group that underwent surgery tended to have a slightly better survival rate. In addition, the small number of follow-up patients and short follow-up duration may have influenced the results. Third, qualitative measures such as the elderly patient’s quality of life were not assessed. A large, well-designed, prospective, multicenter study is needed to confirm the efficacy of the GMOC in determining surgical treatment in frail elderly patients with colorectal cancer. Although the actual commencement rate of standard treatment in frail elderly patients with colorectal cancer was low through the GMOC, evaluation based on CGA of fragile geriatric patients and appropriate counseling and determination of surgical treatment could lead to appropriate management and favorable outcomes. Moreover, structured prehabilitation is more likely to produce better outcomes when actively conducted in the clinic. A large-scale prospective study is needed to establish objective indicators of the decision-making process and to follow the long-term outcomes of geriatric patients who decide to undergo surgery through the GMOC.
 XML Download
XML Download