

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Hepatocellular carcinoma (HCC) is the 6th most common cancer, with increasing incidence, and the third leading cause of cancer-related death worldwide [1]. Curative resection is the optimal treatment for patients with well-preserved liver function [2]. However, most patients fail to undergo curative resection, owing to the clinical characteristics of HCC (local invasion, distant metastasis, and the absence of symptoms in the early stages) [34]. Despite improved diagnosis and treatment, prognosis remains poor. Therefore, more attention should be paid to the investigation of prognostic factors [5].
The presence of a systemic inflammatory response is associated with poor survival in various malignancies [67]. Albumin-to-globulin ratio (AGR) has previously been identified as an independent prognostic factor for overall survival (OS) in patients with HCC [8]. Additional prognostic markers include CRP-to-albumin ratio (CAR) [9], neutrophil-to-lymphocyte ratio (NLR) [10], prognostic nutritional index (PNI) [11], and platelet-to-lymphocyte ratio (PLR) [12]. Despite evidence that these markers predict prognosis, optimal predictors of HCC recurrence remain unclear.
Lymphocyte-to-CRP ratio (LCR) is a novel prognostic biomarker in colorectal cancer that has proved useful for perioperative management and postoperative follow-up [1314]. LCR has also been shown to be an independent prognostic marker in patients with surgically resected HCC [151617]. However, data on its ability to predict recurrence are lacking. Therefore, we explored the clinical significance of LCR as a prognostic marker, especially for recurrence, in patients with surgically resected HCC.
Go to : 
METHODS
Patients
Between July 2010 and October 2021, 173 consecutive patients who underwent surgical resection for pathologically confirmed HCC at our institution were analyzed. All data were blinded. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. The study design was approved by the Ethical Review Board of the National Hospital Organization Fukuyama Medical Center (No. R2-34). The requirement for written informed consent was waived owing to the retrospective nature of the study.
Data collection
The following clinicopathological characteristics were obtained from medical records: demographic data (sex, age at surgery, and body mass index), laboratory data (CRP, lymphocyte count, neutrophil count, platelet count, total bilirubin, ALT, γ-GT, albumin, globulin, total protein, α-FP, and HBV/HCV status), LCR, AGR, CAR, PLR, NLR, PNI, comorbidities (hypertension, diabetes mellitus, cardiac disease, and stroke), operative data (type of resection, blood loss, surgical duration, and blood transfusion), and tumor characteristics, including stage (American Joint Committee on Cancer/Union for International Cancer Control, 8th ed) [18], number, size, microvascular invasion, and differentiation. Liver function was assessed using the Child-Pugh classification. LCR was calculated as lymphocyte count (number/mL) / CRP (mg/dL) [17]. AGR was calculated as albumin / (total protein – albumin). CAR was calculated as the ratio of CRP to albumin [19]. NLR and PLR were calculated as the neutrophil and platelet counts divided by the lymphocyte count, respectively [2021]. PNI was calculated as 10 × albumin (g/dL) + 0.05 × total lymphocyte count (/mm3) [22]. Postoperative complications were defined as complications of Clavien-Dindo grade of ≥III [23].
Follow-up
All patients were followed up until October 2021. Postoperative follow-up included laboratory and imaging studies every 3–6 months for ≥5 years. Recurrence-free survival (RFS) and OS were defined as the time from the date of surgery to the date of recurrence or the date of death or last follow-up, respectively.
Statistical analyses
Data are presented as mean ± standard deviation. Univariate analysis was performed using the chi-square test and Mann-Whitney U-test. Diagnostic accuracy was evaluated using the area under the receiver operating characteristic curve (AUC). The optimal cutoff value of each inflammation-based marker was determined by maximizing the Youden index (sensitivity + specificity – 1) [24]. RFS and OS curves were plotted using the Kaplan-Meier method and compared using the log-rank test. Prognostic factors for RFS and OS were determined using Cox regression. Variables that were significant in the univariate analysis were entered into the multivariate analysis. All statistical analyses were conducted using JMP ver. 11 (SAS Institute, Cary, NC, USA). A P-value of <0.05 was considered statistically significant.
Go to :
RESULTS
Patient characteristics
The patients’ baseline characteristics are shown in Table 1. The study population comprised 144 male and 29 female patients (mean age, 71 years). Sixty-six patients had HBV; 60, HCV; 21, neither HBV nor HCV; 20, alcoholic hepatitis; 5, non-alcoholic fatty liver disease; and 1, autoimmune hepatitis. Most patients (95.9%) were Child-Pugh class A. The mean tumor diameter was 4.1 ± 3.3 cm. Multiple tumors were found in 37 patients. The mean operative time was 402.2 ± 143.1 minutes (mean blood loss, 912.7 ± 139.5 mL). Forty-seven patients required blood transfusion. Partial hepatectomy was performed in 8 patients, subsegmentectomy in 84, sectionectomy in 51, hemihepatectomy in 28, and trisectionectomy in 2. Tumors were well-differentiated in 46 patients, moderately differentiated in 102, poorly differentiated in 14, and unknown in 46. Twenty-nine patients had postoperative complications of Clavien-Dindo grade ≥IIIa. The mean postoperative hospital stay was 15.9 days.
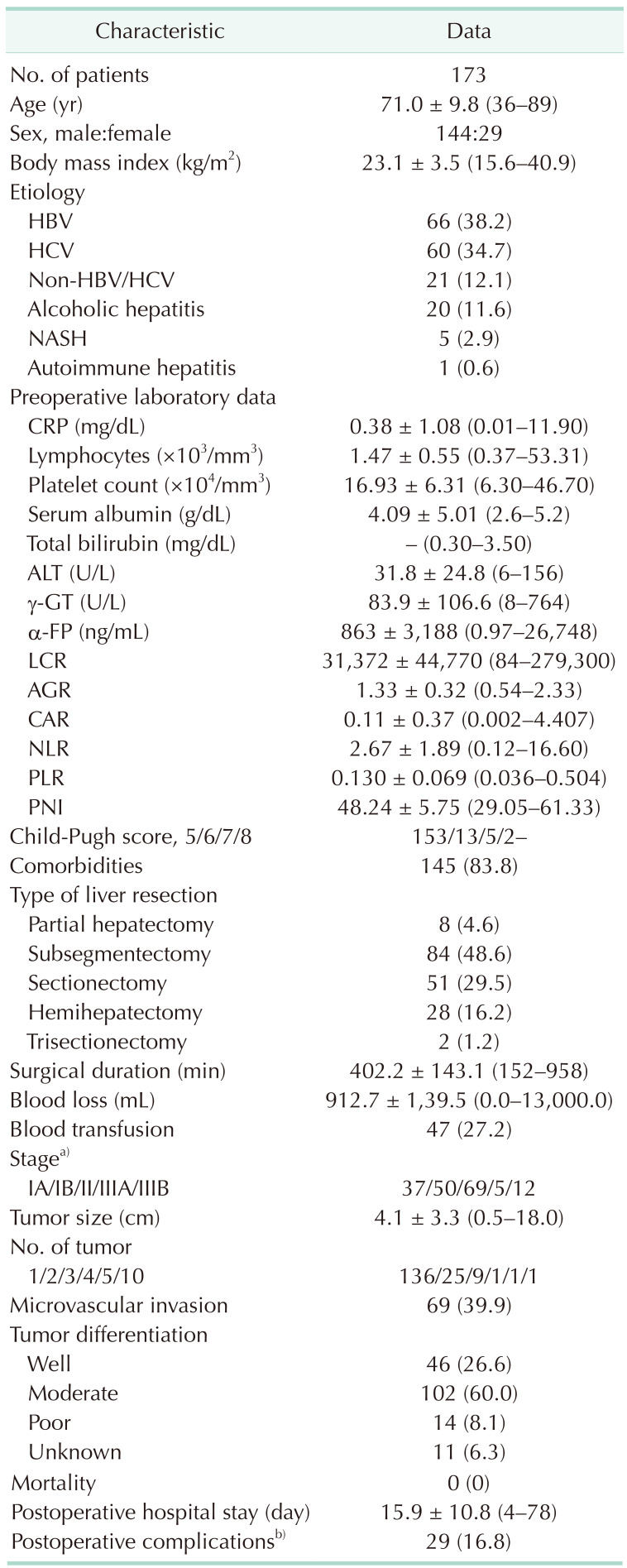
Table 1
Patient demographic and clinical characteristics
Values are presented as number only, mean ± standard deviation (range), or number (%).
NASH, non-alcoholic fatty liver disease; AGR, albumin-to-globulin ratio; AJCC/UICC, American Joint Committee on Cancer/Union for International Cancer Control; CAR, CRP-to-albumin ratio; LCR, lymphocyte-to-CRP ratio; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; PNI, prognostic nutritional index.
a)According to AJCC/UICC (American Joint Committee on Cancer/Union for International Cancer Control), 8th ed. b)Clavien-Dindo grade of ≥IIIa.
![]()
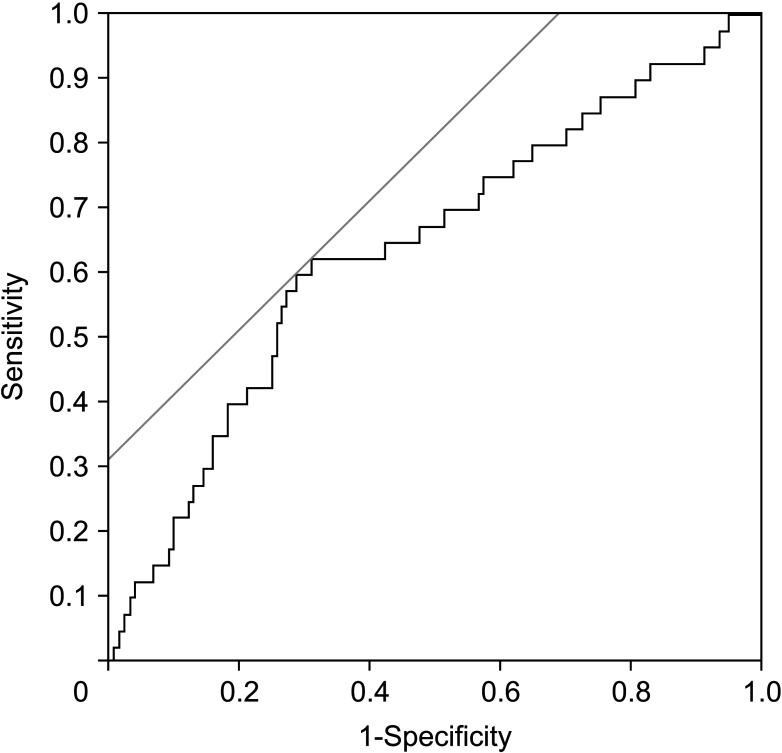
Receiver operating characteristic curve analysis
The cutoff value of LCR was 9,500 (sensitivity, 62.5%; specificity, 69.2%; AUC, 0.643) (Fig. 1). Based on the cutoff value, patients were stratified into high (≥9,500, n = 108) and low (<9,500, n = 65) LCR groups. The AUC values for the other inflammation-based markers were as follows: AGR, 0.631; CAR, 0.632; NLR, 0.590; PLR, 0.506; and PNI, 0.611.
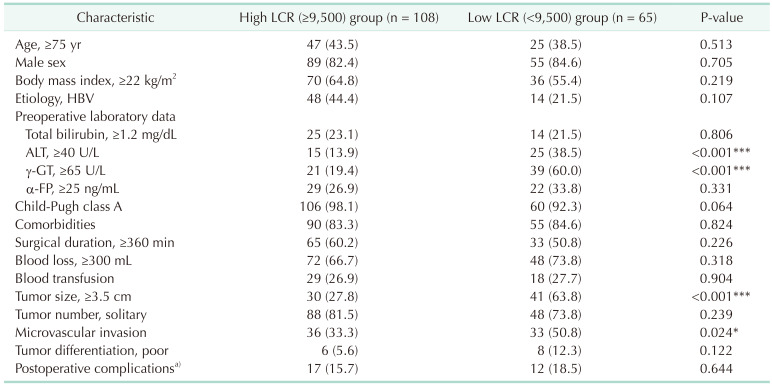
Association between clinicopathological characteristics and lymphocyte-to-CRP ratio
The association between clinicopathological characteristics and LCR is shown in Table 2. Compared with the high LCR group, the low LCR group had significantly higher serum ALT and γ-GT levels, more microvascular invasion, and a larger tumor size.
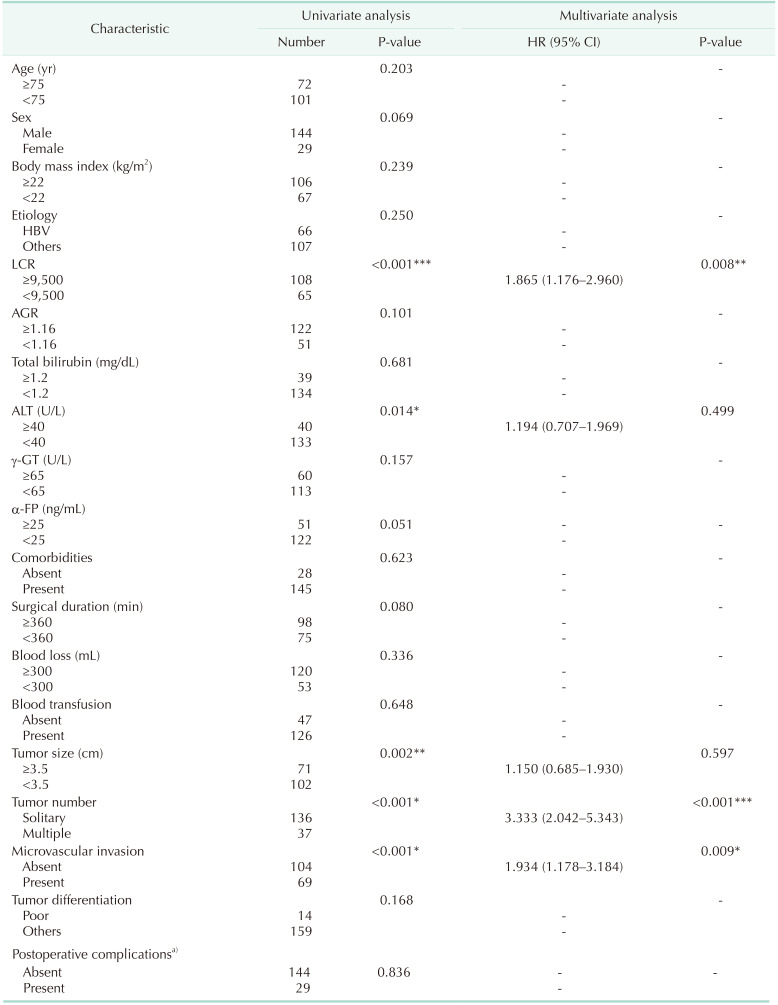
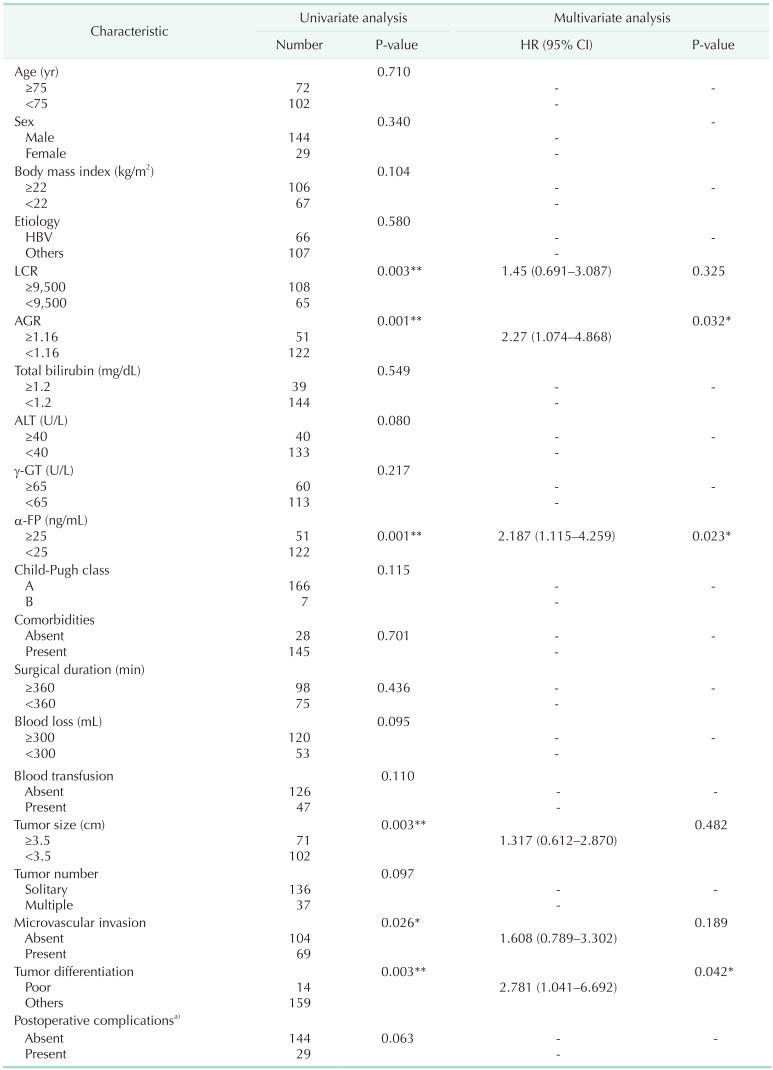
Univariate and multivariate analysis of survival
The median RFS and OS were 24.5 months (range, 1.0–122.4 months) and 124.9 months (range, 1.0–130.6 months), respectively. The 1-, 3-, and 5-year RFS and OS rates were 73.6%, 50.1%, and 40.3% and 90.8%, 80.5%, and 68.2%, respectively. Patients in the high LCR group had longer RFS and OS than those in the low LCR group (Fig. 2). Tables 3 and 4 show the relationships between clinicopathological characteristics and RFS and OS after surgery. In univariate analysis, low LCR, ALT of ≥40 U/L, tumor size of ≥3.5 cm, multiple tumors, and microvascular invasion were significantly associated with poor RFS, whereas low LCR, low AGR, α-FP of ≥25 ng/mL, tumor size of ≥3.5 cm, microvascular invasion, and poor tumor differentiation were significantly associated with poor OS. In multivariate analysis, low LCR (hazard ratio [HR], 1.865; 95% confidence interval [CI], 1.176–2.960; P = 0.008), multiple tumors (HR, 3.333; 95% CI, 2.042–5.343; P < 0.001), and microvascular invasion (HR, 1.934; 95% CI, 1.178–3.184; P = 0.009) were independent predictors of RFS, whereas low AGR (HR, 2.270; 95% CI, 1.074–4.868; P = 0.032), α-FP ≥ 25 ng/mL (HR, 2.187; 95% CI, 1.115–4.259; P = 0.023), and poor tumor differentiation (HR, 2.781; 95% CI, 1.041–6.692; P = 0.042) were independent predictors of OS.
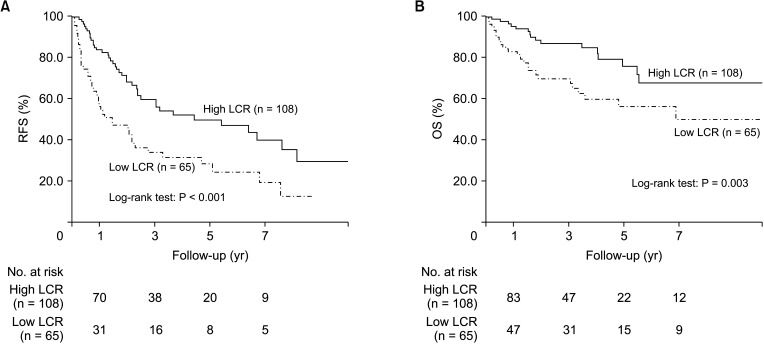 | Fig. 2Kaplan-Meier curves of (A) recurrence-free survival (RFS) and (B) overall survival (OS) in the high and low lymphocyte-to-CRP ratio (LCR) groups. The high (≥9,500) and low (<9,500) LCR groups are represented by solid and dashed lines, respectively.
|
Go to :
DISCUSSION
This study explored the prognostic value of LCR in patients with surgically resected HCC. We showed that low LCR was an independent risk factor for recurrence and that the AUC was higher for LCR than for other inflammation-based markers, suggesting that LCR was a superior predictor of RFS.
LCR has been shown to predict recurrence, prognosis, and postoperative morbidity in various malignancies [1825]. It has also been shown to be superior to other inflammation-based markers for predicting the prognosis of patients with surgically resected HCC [141516]. However, in the aforementioned studies, the AUC analysis of LCR showed poor prognostic performance, and AGR was not considered as a potential prognostic marker. AGR was previously reported to be an independent predictor of OS, but not RFS, in patients with surgically resected HCC [8]. In this study, LCR, which was not investigated previously, was found to be an independent predictor of RFS. To our knowledge, this is the first study to report the effectiveness of LCR in predicting HCC recurrence in an analysis including AGR.
The mechanism underlying the association between LCR and surgical outcomes in patients with HCC has not been fully elucidated. Tumor growth and metastasis result from interactions between tumor cells and the tumor immune microenvironment (TIME) [26]. Tumor-infiltrating lymphocytes are indicators of the cytotoxic immune response [27]. Lymphopenia is associated with poor host immunological competence in malignant disease and predicts oncologic outcomes [28]. Iseda et al. [15] showed that patients with high LCR had fewer vessels encapsulating tumor clusters and higher intratumoral CD8+ T-cell counts than those with low LCR, suggesting that LCR is associated with TIME status. Conversely, serum CRP reflects a systemic inflammatory response. High CRP is associated with early recurrence and poor survival after liver resection [29]. High CRP is also associated with reduced infiltration of CD4+ tumor-infiltrating lymphocytes, which correlates with cancer-specific survival [30]. Therefore, LCR may reflect the antitumor cytotoxicity of the intratumoral immune response in the TIME and affect tumor progression and survival after recurrence. This evidence supports our main finding that low LCR status is an independent prognostic factor for RFS but not OS.
We revealed significant associations between low LCR and impaired liver function and tumor progression. Low LCR was significantly associated with high ALT and γ-GT levels. Child-Pugh scores in the low LCR group were higher than those in the high LCR group, although not significant. These findings may reflect liver inflammation and poor liver function. Low LCR was also significantly associated with larger tumor size and more microvascular invasion than high LCR, suggesting that low LCR is associated with a more aggressive and invasive phenotype than high LCR. LCR reflects the inflammatory and immune status and may be a more sensitive indicator of recurrence. Thus, LCR may better reflect the intrinsic malignant properties of tumor cells.
In multivariate analysis, LCR did not remain an independent predictor of OS in patients with surgically resected HCC. We showed that low AGR (which may reflect nutritional status), α-FP of ≥25 ng/mL, and poor tumor differentiation were independent predictors of OS, as previously reported [8]. Nutritional status and the malignant properties of tumor cells may affect OS more sensitively than RFS.
We consider that LCR, which is accessible, objective, and noninvasive, may be a preferable prognostic factor. It has the potential to assist treatment stratification and guide the management of patients with surgically resected HCC.
There are some limitations to this study. First, it was a small retrospective study at a single institution. Second, our cohort included patients treated with postoperative ablation, endovascular treatment, and molecularly-targeted drugs, which may have influenced the prognosis of these patients. Finally, the AUC value of LCR was not high enough to predict prognosis. Larger multicenter prospective studies are needed to confirm our findings.
In conclusion, preoperative LCR is an independent predictor of RFS in patients with surgically resected HCC. It is superior to other inflammation-based prognostic markers, including AGR. LCR-based risk stratification can be performed before surgery using a standard blood sample for perioperative management. Therefore, LCR could benefit treatment decision-making.
Go to :
 XML Download
XML Download