

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Radiation therapy (RT) plays an important role as a definitive or adjuvant treatment for patients with head and neck cancer [1]. On the other hand, the ionizing effect of radiation is known to alter microvascular endothelial cells and accelerate atherosclerotic changes in large vessels [2]. Radiation-induced carotid stenosis (RICS) is an example of the adverse effects of RT. Owing to the different anatomic and pathologic nature of RICS compared to typical atherosclerotic lesions [34], RICS has been considered to carry a higher risk for an open surgical approach than endovascular treatment in terms of the risk of cranial nerve injury (CNI) and delayed wound healing [5]. In the literature review, heterogeneous results of carotid revascularization outcomes in RICS were found; some authors reported outcomes favoring carotid artery stenting (CAS) with a lower rate or no CNI or wound complications [6], while some others mentioned worse morbidity profiles, including restenosis and late neurologic events in CAS [7].
This study aimed to identify any differences in lesion characteristics between RICS and non-RICS and compare surgical and neurologic outcomes between carot id endarterectomy (CEA) and CAS in patients with RICS.
Go to : 
METHODS
This study was approved by the Institutional Review Board of Samsung Medical Center (No. 2022-04-026) and obtaining informed consent from patients was waived due to retrospective nature of this study.
This study was a single-center retrospective review of all consecutive patients who underwent CEA or CAS between November 1994 and June 2021 at Samsung Medical Center. Among the screened patients, those satisfying the following criteria were excluded: concomitant CEA with coronary artery bypass grafting or open aortic surgery; CEA required for mobile carotid thrombus; carotid stenosis due to non-atherosclerotic causes other than previous neck irradiation, such as Takayasu’s arteritis; stent fracture after CAS; no use of embolic protection device during CAS; and post-CAS carotid artery dissection. For the analyses of the included patients, the following information was retrieved from electronic medical records and imaging studies: demographics, comorbid medical conditions, carotid lesion characteristics, surgical complications, neurologic outcomes, and mortality.
RICS was defined as carotid stenosis (>50%) with a prior history of neck irradiation for cancer treatment on either side. The degree of stenosis (≥70%) was determined according to the NASCET (North American Symptomatic Carotid Endarterectomy Trial) criteria [8] on preoperative images of computed tomographic angiography or magnetic resonance angiography, or according to the velocity criteria (peak systolic velocity [PSV] >230 cm per second with the internal carotid artery/common carotid artery PSV ratio >4.0) on duplex ultrasonography. A lesion that is too high is defined as carotid stenosis extending above the upper border of the C2 vertebral body. A lesion that is too low is defined as carotid stenosis extending below the clavicle. According to the Society of Vascular Surgery clinical practice guidelines, carotid revascularization was indicated for symptomatic carotid stenosis of 50% or greater and for asymptomatic carotid stenosis of 70% or greater. According to the criteria above, restenosis was defined as the presence of >50% stenosis in the most recent imaging study available during the follow-up period.
In terms of patient selection for CEA in RICS, we first considered anatomic feasibility. Additional considerations in these specific patients were their life expectancy based on oncologic status and surgical risks.
All CEA procedures were performed using conventional endarterectomy method under general anesthesia with routine carotid shunting (Pruitt-Inahara Carotid Shunts; LeMaitre Vascular, Burlington, MA, USA) and systemic heparinization before arterial clamping. The closure method, patch angioplasty or primary closure, was determined at each surgeon’s discretion. Neurointerventionists performed all CAS procedures in our center via a transfemoral approach with the procedural routine and selection of devices depending on the interventionist’s preference. Antiplatelet agents were started on the first postoperative day after CEA. After CAS, antiplatelet agents were prescribed before the procedure and continued after CAS.
Our institution’s follow-up schedule after carotid revascularization was scheduled at 1 month and 6 months after the procedure and yearly thereafter, with a vascular surgeon or neurologist. Duplex ultrasonography was the primary modality for follow-up studies before each outpatient visit unless unusual findings were detected.
For the analysis, the RICS and non-RICS groups were compared. In particular, lesion characteristics and treatment outcomes were compared between CEA and CAS in patients with RICS.
Statistical analysis
Continuous variables were expressed as the median and interquartile range (IQR) and compared using Student t-test in unadjusted analyses. Categorical variables are shown as counts with percentages and were compared using Fisher exact tests in unadjusted analyses. A propensity score matching methodology was used to overcome selection bias due to differences in sample sizes between the RICS and non-RICS groups. A 1:1 nearest-neighbor matching algorithm without replacement was utilized without a caliper. Matching factors included demographics, medical comorbidities (age, hypertension, diabetes mellitus, hyperlipidemia, and coronary artery disease), smoking, prior radial neck dissection, contralateral carotid occlusion, and degree of carotid stenosis. Successful matching was determined if standardized differences in the covariates between 2 groups were <10%. Treatment outcomes were compared using logistic regression analysis and the logrank test. P-values less than 0.05 were considered statistically significant. Statistical analyses were performed using IBM SPSS Statistics ver. 27 (IBM Corp., Armonk, NY, USA).
Go to :
RESULTS
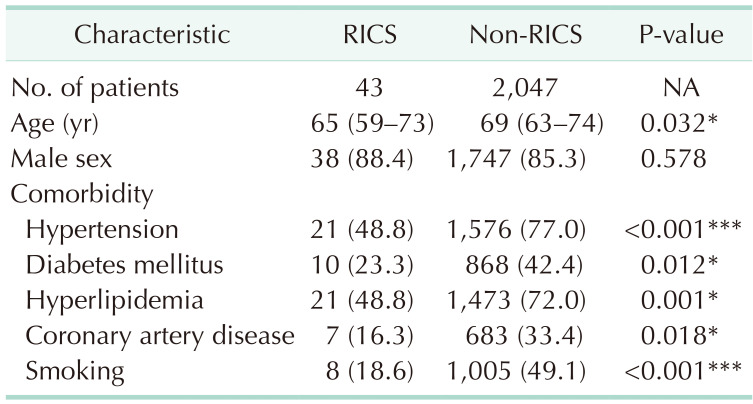
During the study period, 43 patients with RICS and 2,407 patients with non-RICS underwent carotid revascularization by either CEA or CAS for 48 carotid arteries of RICS and 2,247 carotid arteries of non-RICS in our center. The median patient age was 65 years (IQR, 59–73 years) in the RICS group and 69 years (IQR, 63–74 years) in the non-RICS group (P = 0.032). In both groups, the majority of the patients were men. Comorbid conditions were found to be more prevalent in the non-RICS group than in the RICS group (Table 1). Among the patients in the RICS group, indications for cervical irradiation were laryngeal cancer (n = 12), nasopharyngeal cancer (n = 9), tonsillar cancer (n = 9), and other malignancies (n = 13).
Contralateral carotid occlusion was more prevalent in the RICS (16.7%) than in the non-RICS (7.2%) group (P = 0.023). Severe stenosis greater than 70% was also prevalent in RICS (97.9%) than in non-RICS group (86.7%) (P = 0.022). More symptomatic patients were found in the RICS group than in the non-RICS group, but this difference was not statistically significant. The median time from symptom onset to carotid revascularization did not differ between the 2 groups (Table 2).
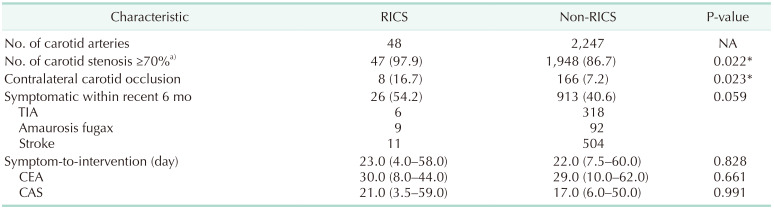
Table 2
Carotid lesion characteristics in patients with RICS and non-RICS
Values are presented as number only, number (%), or median (interquartile range).
RICS, radiation-induced carotid stenosis; NA, not applicable; TIA, transient ischemic attack; CEA, carotid endarterectomy; CAS, carotid artery stenting.
a)Defined as peak systolic velocity (PSV) >230 cm/sec with internal carotid artery/common carotid artery PSV ratio >4.0 on duplex ultrasonography or measured stenosis according to NASCET (North American Symptomatic Carotid Endarterectomy Trial) criteria.
*P < 0.05.
![]()
Table 3 compares detailed lesion characteristics between CEA and CAS within patients with RICS. CAS was more frequently performed than CEA (77.1% vs. 22.9%) in the RICS group. Carotid lesions treated by CAS seemed to have multiple lesions as compared to those by CEA, without statistical significance. There also was no significant difference in location of the main stenotic lesion, length of a stenosis, incidence of contralateral carotid occlusion, total dose of cervical irradiation, and time from the last dose of RT to revascularization between CEA and CAS within the RICS group. Unfavorable anatomy for CEA accounted for 36.4% for CEA and 67.6% for CAS among the RICS group, but without statistical significance (Table 3).
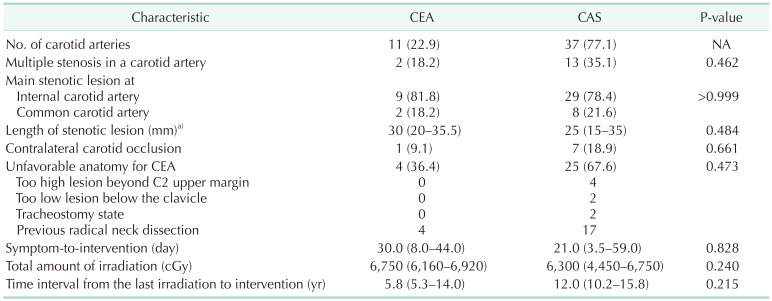
Table 4 compares treatment outcomes between the RICS and non-RICS groups using a 1:1 propensity score-matched analysis. During the median follow-up period of 3.8 years (IQR, 1.5–6.4 years) for RICS and 5.3 years (IQR, 2.4–8.3 years) for the non-RICS group (P = 0.255), there was no significant difference in the incidence of postoperative complications, early and late neurologic outcomes, the occurrence of restenosis, and overall death rate, although there were 2 transient vocal cord palsy in the RICS group and none in the non-RICS group.
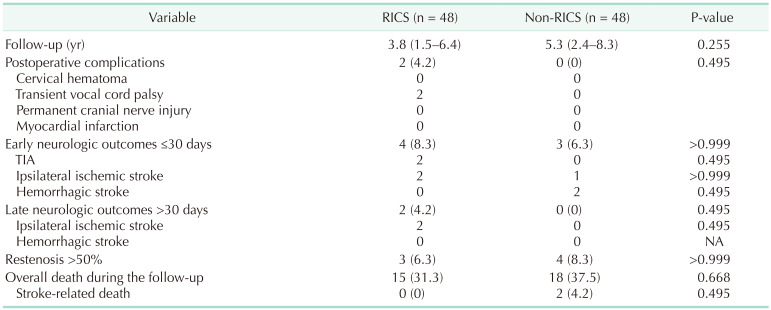
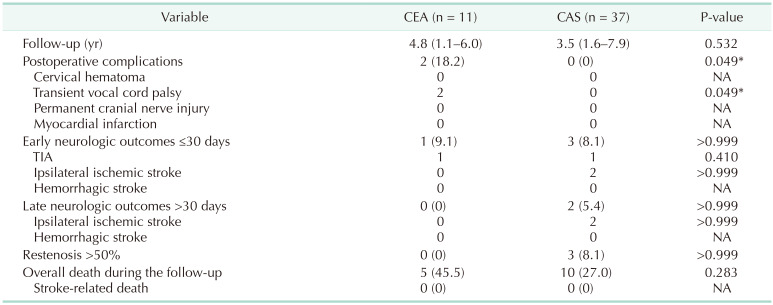
The comparison of treatment outcomes between CEA and CAS within the RICS group is shown in Table 5. During the median follow-up period of 4.8 years (IQR, 1.1–6.0 years) after CEA and 3.5 years (IQR, 1.6–7.9 years) after CAS (P = 0.532), transient vocal cord palsy occurred more frequently in CEA (18.2%) than in CAS (0%) (P = 0.049). Otherwise, no significant difference was found between CEA and CAS within the RICS group.
Go to :
DISCUSSION
The incidence of RICS varies among studies; however, RICS is an unavoidable complication in some patients who undergo cervical-area RT. In addition to the therapeutic benefits of radiation to neoplastic tissues, radiation causes atherosclerotic changes in affected blood vessels [29]. According to Scott et al. [10], the risk of cerebrovascular events increased after cervical RT compared to that in nonirradiated patients. Other investigators have explained that the high risk of cerebrovascular events in RICS patients is attributed to an unstable plaque of RICS, which becomes an embolic source [51112]. Our series was also in line with a similar tendency; severe carotid stenosis and contralateral carotid occlusion were more prevalent in RICS than in non-RICS, despite coexisting medical comorbidities accelerating atherosclerosis, which were significantly more prevalent in non-RICS patients. There were more symptomatic patients in RICS than in the non-RICS group, although the difference did not reach statistical significance.
RICS is known to have distinct anatomic characteristics of the affected lesions, such as long segment involvement and stenosis at atypical locations [13]. In our patients, severe stenosis greater than 70% was more prevalent in RICS than in the non-RICS group. Ionizing radiation also affects soft tissue and skin, resulting in fibrotic changes [6]. Thus, surgeons consider that CEA for RICS is technically demanding in terms of identifying surgical planes and is associated with poorer neurologic outcomes, adjacent CNI, and even wound healing problems [514]. In our study, the comparison of lesion characteristics between CEA and CAS within the RICS group showed that unfavorable anatomic factors for CEA were higher in CAS; however, the difference did not reach statistical significance. Not all patients were eligible for CEA in the RICS group, and we believe this might have affected the results.
CAS upholders reported 8% periprocedural transient ischemic attack and 4% nondisabling stroke rates as favorable outcomes in their prospective study of 24 symptomatic RICS patients [15]. Yu et al. [16] reported similar safety and effectiveness of CAS in the RICS and non-RICS groups, showing no difference in 30-day periprocedural stroke or death rates and ipsilateral stroke rates, based on their 6-year prospective randomized study comparing the outcomes of CAS between the RICS and non-RICS groups.
In our cohort, treatment outcomes, including surgical complications, neurologic outcomes, restenosis rate, and overall mortality, were not significantly different between the 2 groups. Within the RICS group, patients undergoing CEA experienced more transient vocal cord palsy than those undergoing CAS (18.2% vs. 0%, P = 0.049); however, there was no permanent CNI in CEA and CAS groups. Considering that post-CEA CNI rate ranges from 0% to 23% as per previous literature [51718], our results were within an acceptable range. Of note, principles of surgical technique for CEA in RICS were not different from those in non-RICS. However, we tried to minimize peri-arterial dissection to avoid cervical nerve injury during CEA in RICS patients.
In a recent report on results of CEA for RICS, 2.5% early postoperative cerebrovascular events, 96% 3-year primary patency rates, and 98% 3-year freedom from neurologic events were noted [17]. In comparing early and late neurologic event rates between CEA and CAS in RICS patients, we observed statistically nonsignificant results for early (9.1% vs. 8.1 %) and late (0% vs. 5.4%) neurologic event rates.
Since the number of patients was limited, our results might seem worse than other results. However, it is worth noting that difference in neurologic outcomes and overall death rate did not reach statistical significance between CEA and CAS within the RICS group in our study. A recent meta-analysis [7] of stenting versus surgery in RICS supported our results. According to the study, CNI risk was higher in CEA (9.2%; 95% confidence interval, 3.7–21.1) than in CAS group (0%); however, there was no significant difference in the risk of any perioperative cerebrovascular adverse events between CEA and CAS groups. Batarseh et al. [19] recently reported the results of perioperative outcomes comparing transfemoral CAS (TFCAS), transcarotid artery revascularization (TCAR), and CEA in RICS patients. Although their conclusion suggested that TCAR might be the preferred revascularization method for RICS, their results still showed similar rates of perioperative outcomes between TFCAS and CEA.
Regarding carotid restenosis, no significant difference was observed between RICS and non-RICS groups in our study. The restenosis rate after carotid revascularization is reportedly higher after CAS than after CEA [202122]. In our results, carotid restenosis greater than 50% only developed after CAS but not after CEA in the RICS group. However, the difference did not reach statistical significance.
The limitations of this study were as follows. This was a single-center retrospective study with inherent selection bias. In comparing treatment outcomes between the RICS and non-RICS groups, we did not separate them according to the type of revascularization (CEA or CAS). Thus, modality-specific factors may have affected our results. In addition, RICS included CEA-feasible lesions, which may have affected the results. Although our results suggest that both CEA and CAS seem acceptable for RICS revascularization, a randomized trial is needed to evaluate the advantages and disadvantages of each method in this specific group of patients.
In conclusion, RICS requires more attention than non-RICS, considering its lesion characteristics and a higher rate of symptomatic cases. However, the treatment outcomes between RICS and non-RICS patients were not significantly different in terms of early and late neurologic complications. The treatment outcomes between CEA and CAS in RICS patients also were not significantly different, except for more common cranial nerve palsy after CEA than after CAS. If CEA is selectively performed considering individual patient conditions and lesion characteristics, CEA shows acceptable results in RICS patients.
Go to :
 XML Download
XML Download