

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Obstructive sleep apnea (OSA), affecting 9% - 49% of the general population,12 is featured by intermittent complete or partial collapse of the upper airway structures during sleep, resulting in airflow pausing or reduction.3 OSA is accompanied by sleep fragmentation and nocturnal hypoxemia which can inevitably lead to a variety of comorbidities and their sequelae.4 Many previous studies have focused on the consequences of untreated OSA such as cardiovascular diseases, cognitive impairment, and increase risk of mortality.56789 Therefore, prompt diagnosis and management of OSA is critical for reducing the possibilities of developing its comorbidities.
A bidirectional link between poor sleep quality and a variety of pain conditions, particularly musculoskeletal pain disorders has been proposed.101112131415 The relationship between OSA and systemic inflammation appears to have an impact on the development and aggravation of pain symptoms.16 Hypoxemia in OSA has been proven to increase the expression of proinflammatory cytokines such as interleukin 6 and tumor necrosis factor-α and overexpression of opioid receptors 1617 both of which influence central and peripheral pain sensitization and pain amplification mechanisms.161819 The relationship between sleep fragmentation and pain sensitization have been proposed, also.112021 Pain management in OSA patient is complex owing to complicated pain mechanisms and pathophysiology of OSA, therefore the clear management guidelines or treatment protocol have not been proposed yet.
Temporomandibular disorder (TMD) is a collective term referring pain conditions and functional jaw disabilities occurring in the masticatory muscles, temporomandibular joints, and their related structures.22 Several previous studies have emphasized the relationships between sleep disorders and TMD.10111318192324 Approximately, 36% of TMD cases met insomnia diagnostic criteria and over 28% met criteria for OSA.18 Otherwise, 51% of OSA patients had TMD signs and symptoms compared to normal controls.10 In addition, one long term cohort study suggested OSA as a risk factor for the development of first onset TMD.19 The effects of hypoxemia and sleep fragmentation owing to oxygen desaturation and respiratory arousal during night on peripheral and central sensitization in other pain conditions have been postulated from previous reports, however, the clear interactions among oxygen desaturation, sleep fragmentation, and pain-related TMD has not been elucidated, so far. Hence, the aim of the present study was to clarify the potential role of OSA on severity of orofacial pain and jaw function in patients with chronic pain-related TMD using polysomnography (PSG) data.
Go to : 
METHODS
Participants and procedure
This was a cross-sectional study, conducted using the clinical records of TMD and PSG data from 60 adults (male/female, 48/12; mean age, 41.7 ± 13.2 years; age range, 19–74 years) who had been referred to the department of dentistry at a tertiary university hospital, owing to chronic orofacial pain and/or sleep disturbance at night. For more than six months, all participants experienced pain-related TMD. Participants with neurodegenerative disorders, fibromyalgia, chronic fatigue syndrome, craniofacial anomalies, regular use of analgesic and psychotic medications, history of botulinum toxin injection in the masticatory and cervical muscles within 6 months of study entry, and communication incapability were all excluded.
The participants were divided into three groups accordance with the level of OSA. Participants in the control group did not have OSA, whereas those in the mild-moderate and severe OSA group did. All participants underwent assessment of height, weight, size and position of the tongue, and tonsillar size by a trained technician. To evaluate the size and position of the tongue, the modified Mallampati’s score was applied25 and tonsillar size were determined using a grading system proposed in a previous report.26 Two self-administered sleep questionnaires, the Pittsburgh sleep quality index (PSQI) and the Epworth sleep index (ESS) were used to determine the subjective sleep quality and daytime sleepiness, respectively.
Polysomnography
All participants underwent a full overnight in-laboratory PSG (Embla N 7000, ResMed, Germany). The following variables were assessed; total sleep time, sleep latency, sleep efficiency, rapid eye movement (REM) latency, wake after sleep onset (WASO), apnea-hypopnea index (AHI), respiratory disturbance index (RDI), respiratory effort related arousal, oxygen desaturation index, arousal indices, and degree of oxygen saturation. Sleep montages for electroencephalography, electromyogram, nasal airflow using a pressure cannula, oral airflow using a thermistor, snoring recorded using a microphone attached near the thyroid cartilage, respiratory thoracic and abdominal effort measured using plethysmography belts, transthoracic two-lead electrocardiogram, and pulse oximetry were all determined.
Diagnosis of OSA
OSA was determined on the basis of the definition per Center for Medicare and Medicaid Services.27 The diagnosis requires the observed apnea and hypopnea coupled with an AHI of higher than five. The AHI was calculated as the sum of obstructive and mixed apneas and hypopneas per hour of sleep as defined by the American academy of sleep medicine scoring manual.2728 All of the participants were divided into three groups. Participants with AHIs less than or equal to 5 were classified as normal controls, those with AHIs between 5 and 30 were classified as the mild-moderate OSA group, and those with AHI greater than 30 were determined as severe OSA group.29
Diagnosis of the TMD and determination of the number of myofascial trigger points (TrPs) in the masticatory and cervical muscles
TMD was diagnosed according to the Diagnostic Criteria for/TMD (DC/TMD) criteria. Clinical parameters, including amount of pain free opening and maximum unassisted opening, as well as the duration of pain-related TMD symptoms, such as difficulties in opening and/or closing the mouth, and pain in the temple, jaw, and preauricular areas were evaluated. The subjective severity of chronic orofacial pain was assessed using a visual analogue scale and Global Chronic Pain Scale (GCPS) in accordance with the DC/TMD axis II. GCPS is a reliable and valid instrument which assess pain intensity and pain related disability including two subscales, pain intensity and pain disability. Myofascial TrPs were measured bilaterally in the two masticatory and four cervical muscles including the temporalis, masseter, trapezius, sternocleidomastoid, occipitalis, and splenius capitis muscles. TrPs were determined on the basis of the criteria suggested by Simon and Travell.30 The parameters associated with TMD and the number of TrPs in the masticatory and cervical muscles were assessed by one orofacial pain specialist (JHK).
Statistical analysis
A total sample size of 60 participants in a two-way analysis of variance (ANOVA) provided a statistical power of 88.1% at a 0.05 significance level with an effect size of 0.4, according to the power analysis. The data were found to be normally distributed using the Shapiro-Wilk normality test, hence parametric analysis was applied. To compare the participants’ demographic characteristics, PSG results, and parameters related to TMD of the participants, one-way ANOVA and chi-square test were used for continuous and categorical variables, respectively.
Pearson’s correlation coefficient was applied to determine the associations between results from PSG and parameters about pain-related TMD. The variables related with PSG which showed significant differences among the groups were adopted in the correlation analysis. All tests were two-sided and P values which were less than 0.05 by one-way ANOVA and χ2 test, and less than 0.0005 by Pearson’s correlation analysis with Bonferroni’s correction, were considered statistically significant, respectively.
Ethics statement
The research protocol was approved by the Institutional Review Board of the Ajou university hospital (AJIRB-DB-2022-369) and the institutional review board waived the documentation of informed consent due to the retrospective design of the study.
Go to :
RESULTS
Demographic characteristics, subjective sleep quality, and TMD features of participants
There were no statistically significant differences of the age, sex distribution, size and position of the tongue and tonsil among the three groups. On the other hand, differences in body mass index (P = 0.007), ESS (P < 0.001), and PSQI (P = 0.015) showed statistical significance. The parameters related with pain-related TMD symptoms did not show significant differences among three groups except the number of active TrPs in the masticatory muscles and extent of chronicity of the pain-related TMD (P = 0.045) (Table 1).
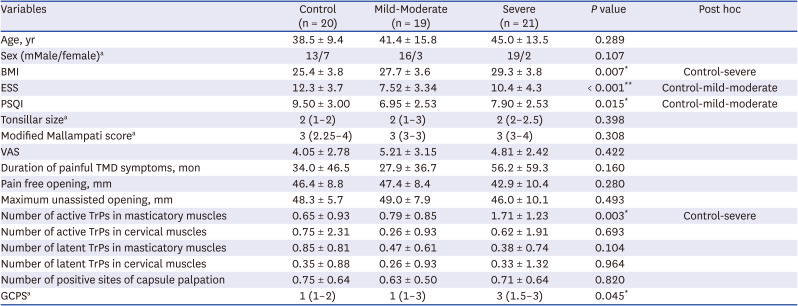
Table 1
Comparison of demographic characteristics, subjective sleep quality, and TMD features of participants
TMD = temporomandibular disorders, BMI = body mass index, ESS = Epworth sleep index, GCPS = graded chronic pain scale, PSQI = Pittsburgh sleep quality index, OSA = obstructive sleep apnea, =,TrP = trigger point, VAS = visual analog scale.
Descriptive values are shown as mean ± SD or median (25th–75th percentile). Data obtained from one-way ANOVA. Post-hoc analysis was conducted by Bonferroni’s test.
aData obtained from χ2 test.
*P < 0.05, **P < 0.001 by one-way ANOVA and χ2 test.
![]()
The distribution of DC/TMD diagnosis including intra-articular TMD and presence of degenerative joint disease and headache attributed to TMD did not show statistical significance among groups, however distribution of pain-related TMD diagnosis showed significant differences (P < 0.001) among the groups. The participants with severe OSA presented higher prevalence of myofascial pain compared to other two groups (Table 2).

Table 2
Diagnostic classification based on the DC/TMD criteria
Data obtained from χ2 test.
DD = disc displacement, TMD = temporomandibular disorders, TMJ = temporomandibular joint MFP = myofascial pain.
aThe diagnosis of intra-articular TMD, pain-related TMD, and presence of degenerative joint diseases were conducted separately in both sides of the TMJs.
*P < 0.05, **P < 0.001 by χ2 test.
![]()
PSG results
The length of REM sleep (P = 0.041) and non-REM (NREM) stage 1 (P < 0.001) and 3 sleep (P = 0.013) showed statistical differences among the groups. Moreover, differences of AHI (P < 0.001), RDI (P < 0.001), total arousal (P < 0.001), mean (P < 0.001) and lowest oxygen saturation (P < 0.001), and average oxygen desaturation (P < 0.001) showed statistical significance (Table 3).
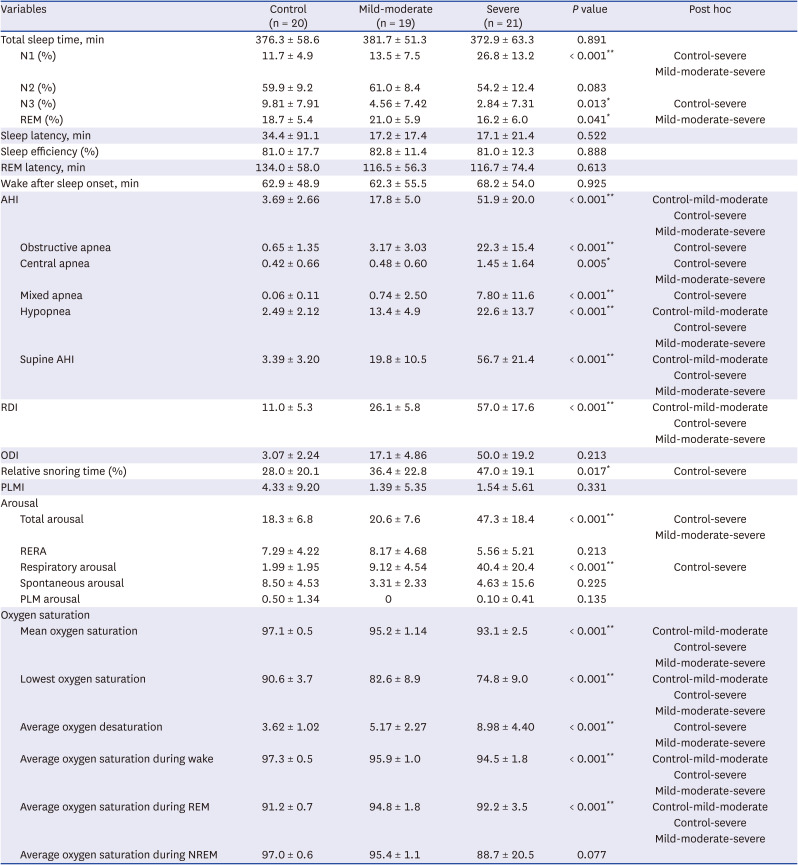
Table 3
Polysomnography results of the participants
Descriptive values are shown as mean ± SD.
Data obtained from one-way ANOVA. Post-hoc analysis was conducted by Bonferroni’s test.
N1 = NREM stage 1, N2 = NREM stage 2, N3 = NREM stage 3, REM = rapid eye movement, AHI = apnea-hypopnea index, RDI = respiratory disturbance index, ODI = oxygen desaturation index, PLMI = periodic limb movement index, RERA = respiratory effort-related arousal, PLM = periodic limb movement, NREM = non-REM.
*P < 0.05, **P < 0.001 by one-way ANOVA.
![]()
Associations among variables related with pain-related TMD and sleep apnea
The number of active TrPs in the masticatory muscles showed significant interactions with variety of apneic and arousals indices including AHI, RDI, respiratory arousal, and degree of mean oxygen saturation, average oxygen desaturation, and average oxygen saturation during REM sleep. The degree of the pain free opening and maximum unassisted opening did not present significant correlation with parameters related with sleep quality and oxygen desaturations (Table 4).
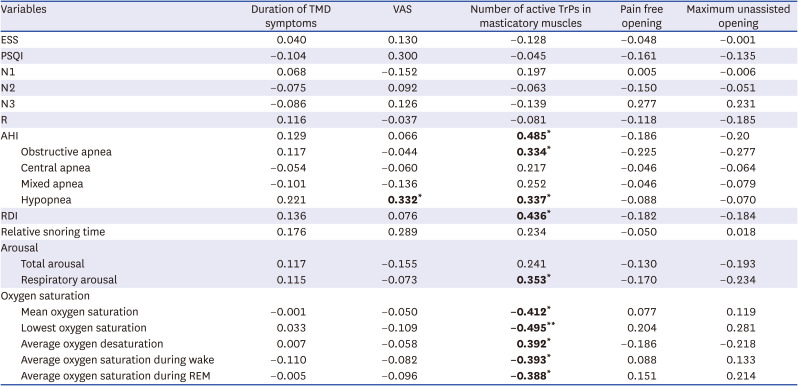
Table 4
Correlations between TMD pain parameters and sleep characteristics
The figures in bold indicate values with statistical significance.
TMD = temporomandibular disorders, VAS = visual analog scale, TrP = trigger point, ESS = Epworth sleep index, PSQI = Pittsburgh sleep quality index, N1 = NREM stage 1, N2 = NREM stage 2, N3 = NREM stage 3, AHI = apnea-hypopnea index, RDI = respiratory disturbance index, REM = rapid eye movement sleep, NREM = non-REM.
*P < 0.0005, **P < 0.00001 by Pearson’s correlation analysis with Bonferroni’s correction.
![]()
Go to :
DISCUSSION
OSA is a chronic condition which is often associated with diverse types of comorbidities including cardiovascular disease and cognitive impairment, increasing the risk of mortality.567 OSA also has an effect on pain modulating mechanism in diverse types of pain disorders.11183132333435 TMD, one of the most common musculoskeletal disorders in the general population appears to interact with sleep disorders including OSA101113181923 but the underlying mechanisms have not been revealed. The purpose of the current study was to elucidate the potential relationships among OSA, orofacial pain, and jaw function in patients with chronic pain-related TMD.
The novel findings of the present study were the significant correlations between the number of active TrPs in the masticatory muscles and the degree of oxygen desaturation. The association between higher analgesic sensitivity to opioid and nocturnal oxygen desaturation in OSA patients have been observed, previously.17 Nocturnal oxygen desaturation appeared to play a role in upregulation of pro-inflammatory cytokine levels, particularly, interleukin-6 which can influence on occurrence of hyperalgesia through enhancement of transient receptor potential vanilloid 1 activity.3637 Moreover, there has been some evidence that interleukin-6 may induce enhancement of N-methy-D-aspartate receptor activity which may lead to impaired descending pain inhibitory pathways.3839 Therefore, the nocturnal hypoxic condition in pain-related TMD patients may have associations with increased pain sensitivity and altered descending pain inhibitory pathway and finally this can have influence on development of central sensitization and hypersensitive taut bands in the masticatory muscles.
Several previous reports have proposed the relationship between sleep fragmentation and pain sensitization.112021 Aforementioned results also supported this phenomenon that respiratory arousals had significant correlations with the number of active TrPs in the masticatory muscles. Sleep deprivation can cause myalgia, tenderness, and chronic fatigue and one study suggested that sleep deprivation impairs descending pain-inhibition pathways that are crucial for controlling and coping with pain.21 Slow wave NREM sleep seems to have a role in suppression of cortisol activity in feedback loop of the hypothalamus-pituitary-adrenal (HPA) axis.40 The chronic TMD patients presented altered feedback mechanisms of HPA axis and increased the levels of orofacial pain intensity and pain-related jaw function disability.41 Hence, disrupted slow wave sleep and sleep fragmentation owing to apneic conditions during sleep might have associations with altered HPA axis feedback mechanism and descending pain-inhibitory pathway impairment. Even though, the impacts of disrupted slow wave sleep structure on pain sensitization and jaw function could not be detected from the present study, the associations among deteriorated sleep structures owing to increased respiratory arousal, altered endocrinological homeostasis, and the development of hypersensitive myofascial TrPs in the masticatory muscles could be assumed.
One intriguing finding was that the significant differences of number of TrPs among the groups were only found in the masticatory muscles, not in the cervical muscles. Because this study was conducted in TMD and orofacial pain clinic, participants in this study might report less suffering from the cervical muscles than from the masticatory muscles.
To the best of our knowledge, the present study is the first attempt to reveal the potential associations among OSA, pain sensitization, and altered jaw function in the chronic pain-related TMD patients. However, there are some restrictions. To begin with, because the present study was a hospital-based study, the participants were recruited from a tertiary university hospital rather than from the community. Secondly, owing to the relatively small sample size, particularly among female OSA patients, the statistical power is inevitably compromised. In addition, this study may provide limited information about the role of sex in pain sensitization in OSA patients. Thirdly, the precise role of oxygen desaturation burden and hypoxemia on pain modulating mechanisms could not be derived due to lack of laboratory analysis. Future research with larger samples of participants including sufficient number of both male and female OSA patients recruited from the community should be required for further investigations.
In conclusion, complicated pain modulating mechanisms and jaw function could be influenced by diverse factors including oxygen desaturation, and sleep deprivation in patients with both pain-related TMD and OSA. Because there has been no consensus on the treatment protocol for pain-related TMD with OSA, it has not been established which disease should be treated first. TMD and orofacial pain specialists should consider not only symptoms of TMD but also OSA, because OSA could cause exaggerated orofacial pain perception and altered jaw function in patients with pain-related TMD. For better management of patients with both OSA and chronic TMD, thorough understanding of significant interactions between these two different conditions would be warranted. Interdisciplinary treatment including a physician, a dentist and an otolaryngologist is also warranted.
Go to :
 XML Download
XML Download