

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Evaluation of the stomach before and after surgery using gastroscopy is essential for treating various diseases of the stomach, including malignancy.12 In particular, gastroscopy can be used for clinical staging, tumor localization, treatment of early gastric cancer, complication management, and post-gastrectomy surveillance.3456
In Korea, most gastroscopies are performed by a gastroenterologist, and they are involved in all aspects of a broad endoscopic area.7 Gastroenterologists usually focus on diagnosing and treating a wide range of diseases using endoscopy, not only malignancy but also benign diseases such as motility disorders or functional diseases. Therefore, the endoscopy education system for gastroenterologists is more systematic, detailed, and strict to produce endoscopy experts.89 In contrast, gastrointestinal (GI) surgeons are more interested in the narrow area of endoscopy, such as localization for gastrectomy, intraoperative gastroscopy, and post-gastrectomy surveillance.1011 In addition, gastroscopy education for GI surgeons was not much developed due to surgeons’ low interest.
Currently, the necessity of surgeons’ endoscopy is being raised because minimal invasive approach is adopted and performed actively in every field of surgery. In particular, intraoperative endoscopy has an important role as an assistant of minimal invasive surgery. Several studies reported the advantages of intraoperative gastroscopy in terms of precise localization of the tumor during laparoscopic surgery, and image-guided surgery using indocyanine green (ICG).2121314 In such situation, education system of endoscopy for surgeon is needed to increase the surgeon’s understanding of gastroscopy, meet the increasing demands of intraoperative gastroscopy, and to make a smooth communication between gastroenterologists and GI surgeons.1516 However, there is a lack of a well-organized gastroscopy education program for surgeons in Korea.
This study aimed to describe the first systematic gastroscopy education program for surgeons in Korea.
METHODS
Education program
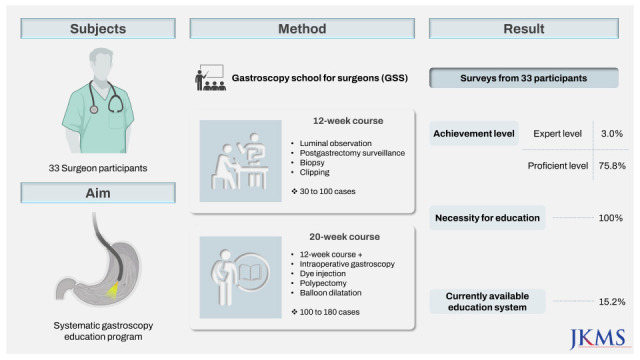
The surgeon’s gastroscopy education program at Seoul St. Mary’s Hospital started in 2010. Initially, it was conducted for senior surgical residents and clinical fellows who trained at the Division of Gastrointestinal Surgery, Department of Surgery of Seoul St. Mary’s Hospital. In August 2017, a systematic gastroscopy education program, entitled the Gastroscopy School for Surgeons (GSS), was launched.
The GSS is divided into 12 and 20 weeks, depending on the breadth and depth of training. The 12-week course is aimed at senior surgical residents and general surgeons (including colorectal, hepatobiliopancreatic, breast, general surgeons, but excluding GI surgeons). Training before clinical practice consists of an introductory lecture, dry lab hands-on training, and simulations. The introductory lecture includes 1) sedation and patient monitoring; 2) indications, limitations, and contraindications of gastroscopic procedure; 3) complications and management; 4) preparation and informed consent with the ethical issue; 5) various gastroscopic findings; 6) writing reports of gastroscopic findings.8 During the clinical practice component, gastroscope insertion and luminal observation, post-gastrectomy surveillance, biopsy, clipping, etc., are taught. Approximately 30 to 100 cases of gastroscopy on actual patients are performed. The 20-week course is specifically designed for the clinical fellows of GI surgery and GI surgeons. In addition to content from the 12-week course, advanced techniques such as intraoperative gastroscopy, tumor localization with dye injection, polypectomy, and balloon dilatation are included, and approximately 100 to 180 cases are performed.
All trainers are GI surgeons, with at least several years of experience in gastroscopy. More than 1,000 cases are performed by each trainer per year. Trainer skills were standardized through meetings and consensus before teaching in the GSS.
Assessment
The actual clinical practice included scope handling, luminal observation, scope insertion, mouth to mouth, and additional procedures. During the training, the trainer evaluates the trainee’s skill using Miller’s Prism, and each step must be performed excellently before progressing to the next step.17 Self-assessment of the learner’s skill level before and one year after training was recorded using the Kirkpatrick-Phillips model.18 The current status of the surgeon’s gastroscopy experience in each participant’s institution and their perception of gastroscopy education in Korea were recorded through a post-training survey.18 The survey form is shown in Supplementary Data 1.
Participants and data collection
Participants who registered for the GSS and trained between August 2017 and November 2019 were enrolled in this study. The participants were recruited through a brochure and promotion through the Korean Surgical Society, the Korean Gastric Cancer Association, and the Korean Association of Surgeons. To ensure high-quality education, the trainer and trainee were matched 1:1, and the trainee’s performance was evaluated by the trainer during the training.
Gastroscopy was performed on patients who underwent outpatient gastroscopy at the Division of Gastrointestinal Surgery of Seoul St. Mary’s Hospital. Prospectively collected data on the condition of the stomach, reconstruction method, and procedures during gastroscopy were analyzed.
Statistical analysis
Descriptive statistics were reported as numbers (percentages) and medians (interquartile ranges). Categorical variables were analyzed using the χ2 test and Fisher’s exact test to compare the groups. Statistical significance was set at P < 0.05. All statistical analyses were performed using SPSS for Windows (ver. 21.0; SPSS, Inc., Chicago, IL, USA).
RESULTS
Characteristics of the participants
In total, 33 participants were included in this study. The mean age was 35 years old. Twenty-five participants completed the 12-week course, and eight the 20-week course. The median number of gastroscopy cases was 62. The trainees consisted of three GI surgeons, nine general surgeons, 20 surgical residents, and one physician (Table 1).
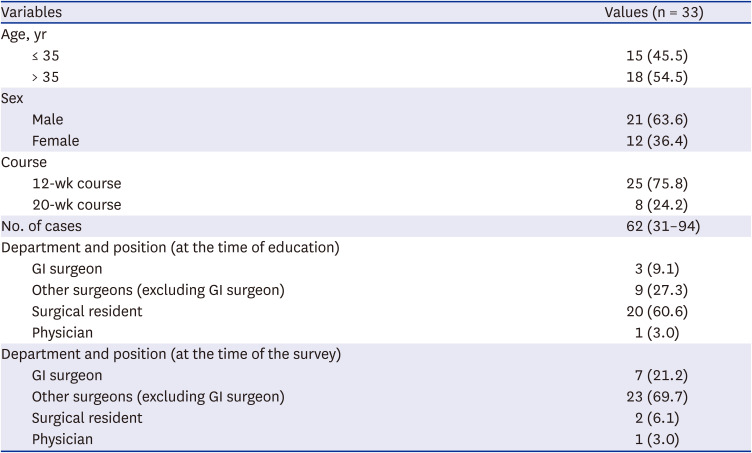
Table 1
Characteristics of the participants
![]()
Details of the gastroscopy cases
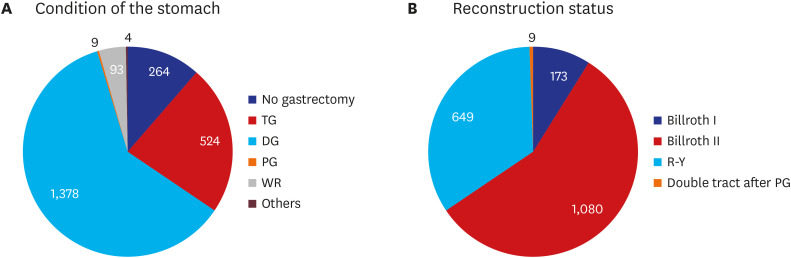
Of the 2,272 cases of gastroscopy, 264 (11.6%) cases had no history of gastrectomy, and 2,008 (88.4%) cases had a history of any type of gastrectomy. Among the gastrectomy cases, the most common history of gastrectomy was distal gastrectomy (60.7%), followed by total gastrectomy (23.1%). Proximal gastrectomy, gastric wedge resection, and other types of gastrectomy were reported at 0.4%, 4.1%, and 0.1%, respectively. The reconstruction method after 1,378 distal gastrectomies consisted of Billroth I gastroduodenostomy (12.6%), Billroth II gastrojejunostomy (78.4%), and Roux-en-Y gastrojejunostomy (9.1%). Roux-en-Y esophagojejunostomy was performed for all gastrectomy cases. After proximal gastrectomy, double-tract reconstruction was performed in all patients (Fig. 1). Among the 2,272 cases of gastroscopy, additional procedures (other than luminal observation) performed were biopsy (18.0%), clipping (0.6%), injection (0.2%), dye spreading (0.4%), and balloon dilatation (0.6%). Severe gag reflex was the most common adverse event during a gastroscopy (29 cases). Mucosal injury, minor bleeding, and incomplete luminal observation were observed in one, nine, and four cases, respectively. All adverse events were resolved without special management (Supplementary Table 1).
Survey’s results I: participant’s gastroscopy experience after education
After more than one year of training, a self-assessment of gastroscopy performance survey was completed by all 33 participants. One year after the training, the participants’ positions were seven GI surgeons, twenty-three general surgeons, two surgical residents, and one physician (Table 1). Currently, three participants performed gastroscopy as their main work (3 or more times/week), and seven performed gastroscopies weekly or more. In contrast, 16 participants have not performed gastroscopy in their work (Fig. 2A). One participant self-assessed their gastroscopy skills to be at the expert level (able to train others), and 25 evaluated themselves as good performers (without the need for supervision) or better. Notably, not a single participant evaluated themselves as incompetent in gastroscopy (Fig. 2B). All participants were able to perform basic procedures, such as luminal observation and biopsy. A total of 19 patients underwent minor procedures, such as clipping, injection, dye spreading, or balloon dilatation, and four underwent major procedures, such as stent insertion, polypectomy, or endoscopic submucosal dissection. Moreover, ten participants were able to perform intraoperative gastroscopy, and one was able to perform advanced procedures, such as endoscopic retrograde cholangiopancreatography (ERCP) or enteroscopy (Fig. 2). There was no significant difference in the skills and confidence level of the participants regardless of the training course (12-week vs. 20-week) completed. However, the skills level was relatively lower among participants who were trained in less than 60 cases (Supplementary Table 2).
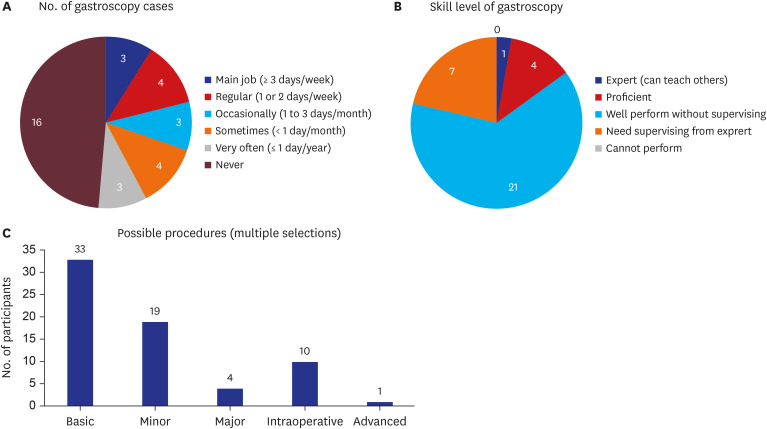
Fig. 2
Participant characteristics. (A) The number of gastroscopy cases. (B) Self-assessed skill level in gastroscopy. (C) Possible procedures. Basic procedures: luminal observation and biopsy. Minor procedures: clipping, dye injection, and balloon dilatation. Major procedures: stent insertion, polypectomy, and endoscopic submucosal dissection. Advanced procedures: endoscopic retrograde cholangiopancreatography and enteroscopy.
![]()
Survey’s results II: current status of surgeons’ gastroscopy
The survey also collected information on the gastroscopies performed by surgeons at the participant’s institution. At the time of the survey, 20 participants worked at seven tertiary university hospitals, seven were in private clinics, and six were in military service for their duty. The role of the surgeon in performing gastroscopy was diversely distributed by institutions, from all procedures were performed for all the cases to impossible to perform any procedures at all (Fig. 3A). There was no systematic gastroscopy education program for surgeons in any of the institutions except Seoul St. Mary’s Hospital (our institution). There were a few smaller training sessions conducted by surgeons or gastroenterologists (Fig. 3B). Despite the lack of formal gastroscopy training, surgeons reported that more than half of intraoperative gastroscopy procedures were performed by surgeons (Fig. 3C).

Survey’s results III: subjective opinions of the participants
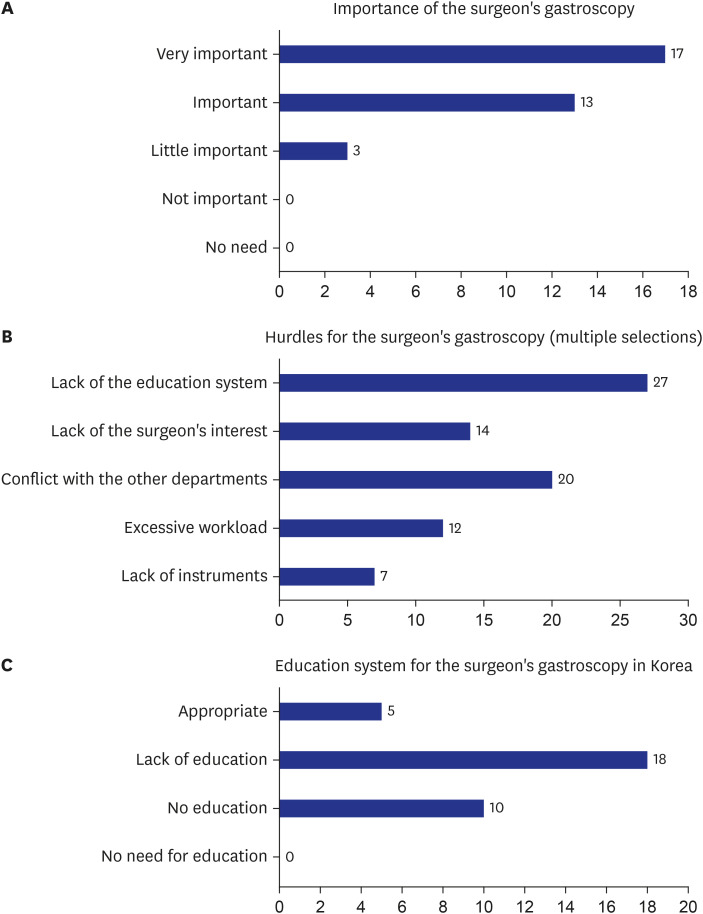
All participants recognized that gastroscopy was important to surgeons (Fig. 4A). The lack of a systemic education system was considered the primary barrier to surgeons performing gastroscopy. Additionally, conflict with the other departments was also recognized as a major hurdle. Furthermore, there was a perceived lack of interest among surgeons and the excessive workload was also problematic (Fig. 4B). Most participants stated that the gastroscopy education system for surgeons in Korea was insufficient (Fig. 4C).
The participants provided their subjective opinions on the surgeon’s gastroscopy in the survey. A total of 87.9% identified the current problems associated with gastroscopy and highlighted the limitations of preoperative information and postoperative complication management when gastroscopy is performed by a non-surgeon, such as a gastroenterologist. The lack of a gastroscopy training system was also articulated. Second, 90.9% responded to the question regarding the merits of surgeons performing gastroscopies. The participants said that surgeons’ gastroscopy is useful in determining the detailed surgical plan preoperatively, and various reconstruction methods can be easily determined during postoperative surveillance. Finally, 54.5% provided suggestions for the development of the surgeon’s gastroscopy. Participants confirmed that it is necessary to increase the quality and quantity of gastroscopy education, with more training centers, and official support from professional associations and societies (Supplementary Table 3).
DISCUSSION
Historically, endoscopy was initiated by surgeons. After Mikulicz performed the first practical gastroscopy in 1880, the first sigmoidoscopy in 1895, the first ERCP in 1968, and the first colonoscopic polypectomy in 1969, were all performed by surgeons.1920 Currently, the clinician responsible for performing endoscopy differ among countries. In some countries, both gastroenterologists and surgeons are major providers. In other countries, gastroenterologists perform most of the endoscopy.2122 In Korea, most endoscopies are performed by gastroenterologists. Surgeons or physicians perform endoscopies only in a few hospitals. Therefore, access to endoscopy among surgeons is not very common. Several studies have reported the importance of providing tailored treatment by determining the extent of surgery based on precise preoperative or intraoperative localization.2111223 Moreover, studies on intraoperative gastroscopy, such as fluorescence image-guided surgery using ICG or laparoscopic-endoscopic cooperative surgery, have been actively reported.1424252627 Gastroscopy is also widely used for post-gastrectomy complication management.52829 Currently, reconstruction after gastrectomy is becoming increasingly complex and diversified. Hence, it is critical for the clinician performing gastroscopic surveillance to have an excellent understanding of post-gastrectomy anatomy.303132 As the use of endoscopy during and after surgery has increased, the importance of the surgeon’s understanding of endoscopy has been further emphasized. Furthermore, as shown in the present study, surgeons are increasingly interested in learning and performing gastroscopies.
Practical and systematic education is essential for proper and safe endoscopy. There have been various reports of this in the gastroenterology field. The American Society for Gastrointestinal Endoscopy presented the principles for safe and effective endoscopy.3334 The Korean Society of Gastrointestinal Endoscopy also reported the status of endoscopy training for gastroenterologists.89 In contrast, there are limited reports on endoscopy training for surgeons. There are a few reports from professional associations and societies in Canada and the United States.1635363738 In contrast, there is only a single report in Korea: the initial gastroscopy training program for senior surgical residents and clinical fellows in GI surgery and the results related to the learning curve in 2012.39 After then, the importance of gastroscopy for surgeons and the need for gastroscopy training at the professional association and society level has increased. In response, the GSS, a systematic education program, was launched.
The GSS is a program without long history and has not been externally verified. Also, it is insufficient in terms of quantity and detail compared to the endoscopy education program implemented by the Korean Society of Gastrointestinal Endoscopy.8 However, the GSS is not designed to train at the same level as expert gastroenterologists or endoscopy specialists. The purpose of the GSS is to increase the understanding of gastroscopy and enable smooth communication with a gastroenterologist by learning basic gastroscopic techniques such as localization before or during surgery and routine surveillance after surgery as a GI surgeon. In addition, maximizing the advantages of intraoperative gastroscopy and improving surgical outcomes is another goal. Although the quantity of clinical practice of the GSS seems to be insufficient, several reports suggested the minimum quantity of clinical practice required to overcome the learning curve in limited endoscopic training for surgeons.163940 Moreover, the GSS consists of various educational methods, such as basic theory classes, dry lab hands-on practices, and simulations used for safety training. Trainers were all GI surgeons with extensive gastroscopy experience and matched 1:1 with trainees to conduct training. This allowed immediate and appropriate feedback for learning, and tailored training could also be provided. As a result, most of the participants could perform gastroscopy independently without a supervisor, and some had reached a level where they could train others. This result corresponds to the “Return On Investment” in the Kirkpatrick-Phillips model. Therefore, the results of this study revealed the effectiveness of a systematic gastroscopy education program for surgeons.18 Based on this report, the GSS should be developed more systematically and receive validation from an external judge of endoscopy experts in the future.
In Korea, surgeon’s gastroscopy is actively performed in a few institutions, while most institutions do not. In particular, only our institution has a systematic educational program for surgeons for gastroscopy education. Recognizing the importance of gastroscopy in surgery, several surgical societies, such as the Korean Surgical Society and the Korean Gastric Cancer Association, have widely promoted gastroscopy education programs in every aspect. As mentioned by the participants, available training programs are still insufficient at present. Surgeons’ gastroscopy education programs need to be developed through various routes, with the support and policy promotion at the professional association and society level. Every surgeon and surgical institution should have an interest in developing the surgeon’s gastroscopy skills and knowledge, including intra- or perioperative gastroscopy. Furthermore, it is critical to develop more training centers and reach a consensus with the gastroenterologists at the professional body level.
The present study has several limitations. First, the quantity of clinical practice of the GSS is insufficient compared to education program for the gastroenterologist. However, as mentioned above, since the final goal of the two educations is different, the GSS could be considered as consisting of the minimum requirement of educational content, duration, and quantity to achieve its final goal. The development of more educational programs from more training centers could provide a higher-quality education for surgeons in the future. Second, the survey was completed only by participants who sympathized with the importance of surgeons’ gastroscopy and felt the need for gastroscopy education. Also, a few questions tend to reflect only the subjective opinions of respondents. Although the selection bias and lack of objectivity, we believe it would be minimal, considering that surgeons’ interest and desire for gastroscopy training have already been voiced in many congresses and reports.15 In addition, one of the most critical purposes of this report is to awaken surgeons’ awareness of the importance of the development and expansion of the surgeon’s gastroscopy education program. Consequently, although the survey results could be subjective, such opinions would also be necessary. Third, the gastroscopy cases performed by participants in this study were largely limited to post-gastrectomy. For surgeons who have a better understanding of post-gastrectomy status than gastroenterologists, gastroscopy for post-gastrectomy status is important. In addition, to expand the surgeon’s scope of practice relating to gastroscopy, it is essential to focus on post-gastrectomy surveillance.
In conclusion, the present study introduced the first systematic gastroscopy education program for surgeons in Korea. Our systematic education could meet the clinical needs of surgeons. We also suggested a future direction for gastroscopy training among surgeons. For the expansion and development of gastroscopy among surgeons, the efforts of individual surgeons must be accompanied by the endeavor to expand infrastructure and training facilities for gastroscopy by surgeons at the society and institutional level.
 XML Download
XML Download