

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
A gastrostomy tube is used when a nasogastric tube is required for more than 1 month to provide sufficient nutrition when oral feeding is impossible.1 It is already well known that nutrition through gastrostomy tubes improves malnutrition status of children with neurodisabilities or oncologic conditions, has a positive effect on prognosis, and induces longer survival.2 Gastrostomy tube placement can be performed with upper gastrointestinal (UGI) endoscopy or surgical methods. Some centers have implemented radiological methods that use fluoroscopy instead of UGI endoscopy. Recently, pediatric endoscopists in Korea have been performing percutaneous endoscopic gastrostomy (PEG) using UGI endoscopy. In the past, PEG was mainly performed using the pull method, and it was recommended to use it initially. Complications such as infection and dislodgement have been reported to be higher than with the surgical method. Recently, some institutions choose to use the push method in children.34
With the implementation of laparoscopy, the disadvantages of conventional open surgery have greatly improved.5 To date, PEG methods using UGI endoscopes have been recommended as a better way to implement them without complications and are easier than other methods for pediatric gastrostomy tube placement. However, if PEG procedures are difficult due to structural problems of the stomach or if fundoplication is required due to gastroesophageal reflux disease (GERD), a surgical method is required.2 Although various methods for gastrostomy tube replacement such as the pull-method PEG, push-method PEG, open surgery, laparoscopic surgery, and radiological methods have been implemented, large complications are likely associated with the individual characteristics of patients rather than the procedure itself.
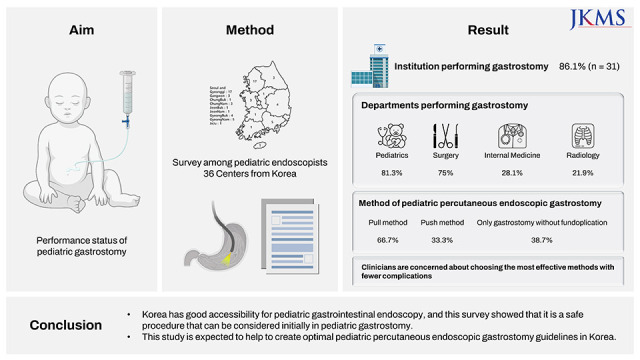
In this study, we aimed to investigate the performance status of pediatric PEG in South Korea and to report indications and appropriate methods for domestic situations. We also aimed to compare questionnaire variables according to different groups in order to examine associations between variables.
METHODS
Survey
In October 2021, a survey was conducted at 48 institutions that conduct UGI endoscopy in South Korea. In the questionnaire, the availability of pediatric gastrostomies, the average number of procedures per year, and the method of implementation were investigated. In the case of PEG, the method of PEG (pull vs. push), the type of tube used, and the implementation method according to the weight of the child were also investigated. Further questions included whether replacement of the gastrostomy tube was possible at each institution, which department performed the replacement, whether gastroscopy was performed after gastrostomy, and whether fundoplication was performed with gastrostomy. Lastly, complications that occurred after gastrostomy, when the gastrostomy was removed, when re-surgery was conducted, whether the nutritional status of children actually improved, and whether the re-hospitalization rate was reduced by gastrostomy were investigated.
We also compared questionnaire variables between groups divided according to the number of annually performed pediatric gastrostomies at each center, the specialist performing pediatric gastrostomies, and recently used PEG method.
Statistical analysis
For statistical comparisons between groups, the χ2 test or Fisher’s exact test was used for categorical variables. Comparative data for categorical variables were reported as numbers and percentage. Statistical significance was defined as a P value ≤ 0.05. All statistical analyses were performed using R version 3.2.3 (R Foundation, Vienna, Austria).
RESULTS
Questionnaire answers
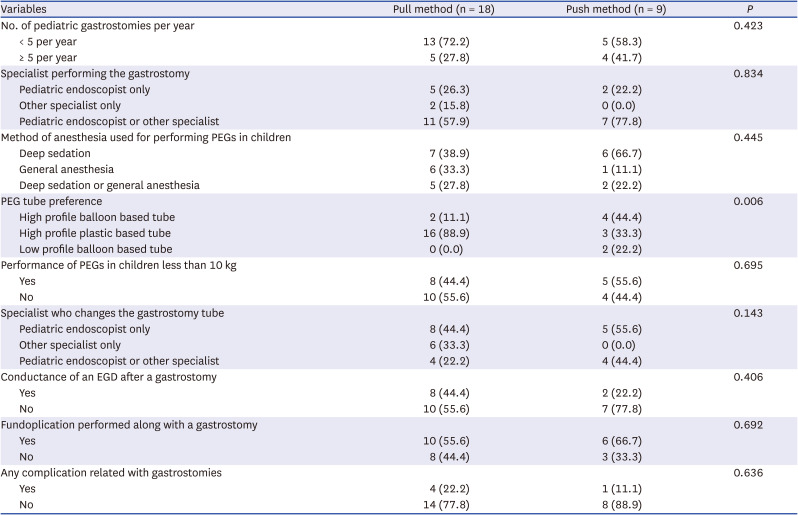
Of the 48 institutions where the survey was requested to be applied, 36 (75.0%) responded. The geographic locations of the 36 institutions are shown in Fig. 1. Of the 36 institutions, gastrostomy was performed in 31 (86.1%). Regarding the number of gastrostomies performed annually, 19 institutions (61.3%) answered that they performed fewer than five gastrostomies/year (Table 1). The gastrostomy was performed by only pediatric endoscopists at 7 institutions (22.6%), by other specialist only at 6 institutions (19.4%), and by pediatric endoscopists or other specialists at 18 institutions (58.1%). PEGs were performed in 27 institutions (87.1%). When performing PEGs, 13 institutions (48.1%) performed deep sedation, 7 institutions (25.9%) performed general anesthesia, and 7 institutions (25.9%) performed either deep sedation or general anesthesia. There were 18 institutions (66.7%) using the pull method for PEG and 9 institutions (33.3%) using the push method. High-profile balloon-based tubes were used in 6 institutions (22.2%), and 19 institutions (70.4%) used high-profile plastic-based tubes. Two institutions (7.4%) used low-profile balloon-based tubes (Table 1).
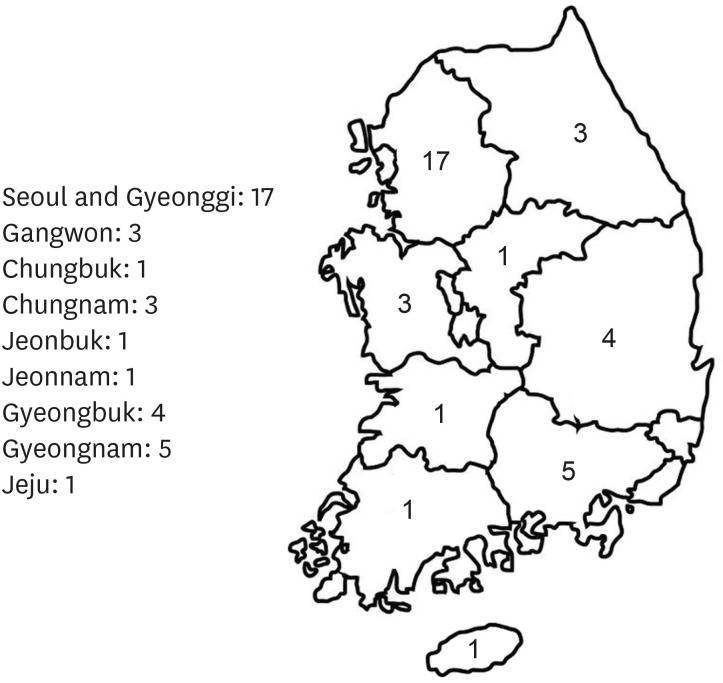
Table 1
Questionnaire items and answers of the survey

When asked if children under 10 kg underwent gastrostomies, 13 institutions (48.1%) answered yes. The replacement of gastrostomy tubes was performed by only pediatric endoscopists at 15 institutions (48.4%), by other specialist only at 7 institutions (22.6%), and by pediatric endoscopists or other specialists at 9 institutions (29.0%). When asked whether esophagogastroduodenoscopy (EGD) was conducted at least once after gastrostomy, 21 institutions (67.7%) answered that they had never performed it. When performing gastrostomies, fundoplication procedures to prevent GERD were performed in 19 institutions (61.3%) if deemed necessary. However, 12 institutions (38.7%) answered that gastrostomy was always implemented alone (Table 1).
When asked whether they experienced a situation in which the gastrostomy tube had to be removed after gastrostomy, 3 institutions (9.7%) answered yes. The reasons for gastrostomy tube removal were: oral nutrition became possible and therefore, the tube was no longer necessary, buried bumper syndrome, and the general rigidity became too severe to use the gastrostomy tube. When asked whether they experienced reoperation after gastrostomy, 5 institutions (16.1%) answered yes. The reasons for these were buried bumper syndrome in 2 cases, site infection in 1 case, and tube migration in 1 case, and incorrect tube location after open surgery, leading to feeding problems in 1 case. When asked whether gastrostomy tube treatment was thought to improve patients’ nutritional status, 31 institutions (96.8%) answered yes. When asked whether gastrostomy tube treatment seemed to reduce the patient’s hospitalization rate, 27 institutions (87.1%) answered yes (Table 1).
Comparison between questionnaire variables between groups
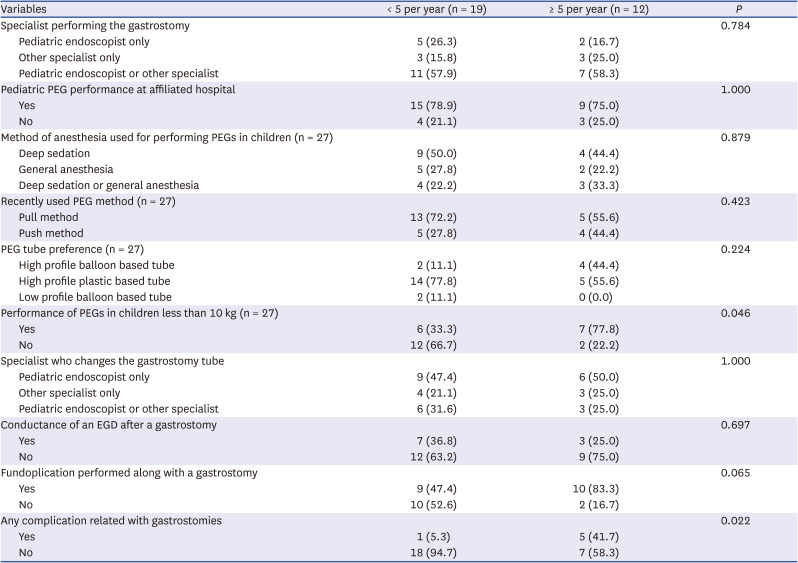
According to the comparison between the groups divided according to the number of to the number of annually performed pediatric gastrostomies at each center, the rate of PEG performance in children less than 10 kg was significantly higher in centers that had answered that they were conducting ≥ 5 gastrostomies per year than those that had answered that they were conducting < 5 gastrostomies per year (77.8% vs. 33.3%, P = 0.046). Complications related with gastrostomies were also significantly higher in in centers that had answered that they were conducting ≥ 5 gastrostomies per year than those that had answered that they were conducting < 5 gastrostomies per year (41.7% vs. 5.3%, P = 0.022) (Table 2).
Table 2
Comparison of groups divided according to the number of annual pediatric gastrostomies (N = 31)
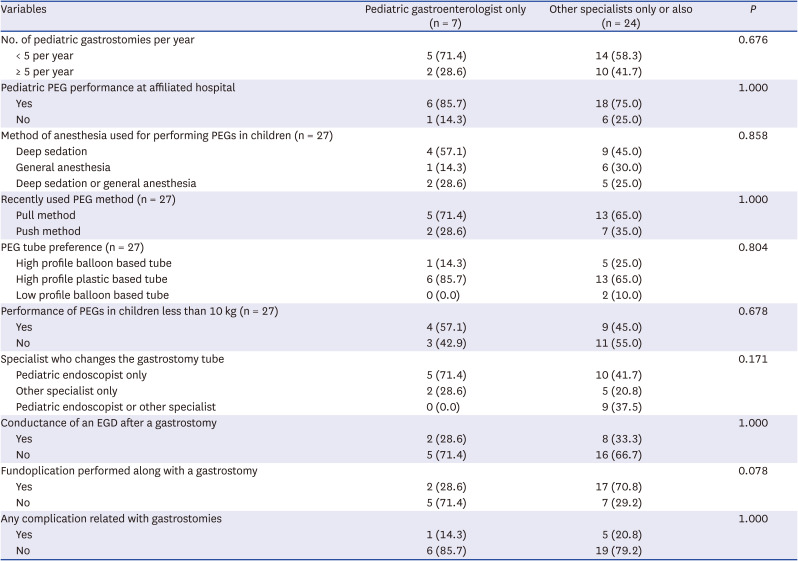
According to the comparison between groups divided according to the specialist performing pediatric gastrostomies, no significant difference in questionnaire variables were observed between the “pediatric endoscopist only” group and the “other specialists" group (Table 3).
Table 3
Comparison of groups divided according to the specialist performing pediatric gastrostomies (N = 31)
According to the comparison between groups divided according to the recently used PEG method, PEG tube preference was statistically significant between the ‘pull method’ group and the ‘push method’ group (P = 0.006). Those using the pull method preferred the high profile plastic based tube (88.9%), while those using the push method preferred the high profile balloon based tube (44.4%) (Table 4).
Table 4
Comparison of groups divided according to recently used PEG method (N = 27)
DISCUSSION
There are very few endoscopy centers in Korea where pediatric endoscopy is possible. The demand for pediatric gastrostomy is also not high compared to that of adults, but it is an important procedure from the perspective of the nutritional treatment of patients. Through this survey, we observed that although there are not many cases of pediatric gastrostomy in Korea, pediatric PEG and pediatric surgical gastrostomy (SG) are performed to a similar extent. Some centers perform PEG with the help of endoscopists from the Department of Internal Medicine, and very rarely perform gastrostomy by imaging. Gastrostomy can be performed in various ways because there is no treatment method that has enough advantages to give absolute priority. With the development of gastrostomy methods, there are fewer complications, and it can be performed without difficulty with less time and cost. Some studies have reported that gastrostomy was performed safely with the collaboration of endoscopists and surgeons, and that could decrease the risks for each method.6
Gastrostomy was performed using only SG until 1980. PEG was initiated by Ponsky, a surgeon specialized in adults, who developed the pull method. It is referred to as the pull method because the thread from the abdominal skin is removed from the mouth using an endoscope, and the gastrostomy tube is tied and then pulled outward from the abdomen and held in position.7 Although the procedure time is short owing to the simplicity of the method, it cannot be used if the esophagus is narrow because the gastrostomy tube passes through the mouth to the esophagus. In addition, it is associated with a risk of infection. Therefore, if a patient has a narrow esophagus or a high risk of infection, other methods should be considered first.28 In addition, the pull method requires the use of a gastrostomy tube made of a plastic bumper. In this survey, 70.4% of institutions were found to use high-profile plastic-based tubes, where the pull method was performed, and buried bumper syndrome occurred only in institutions using the pull method. Buried bumper syndrome occurs when the bumper digs into the abdominal wall and dislodgement occurs and is thought to be a consequence of the plastic bumper part of the tube rather than the procedure method.3
The push method uses an introducer that performs gastropexy from the abdominal skin and inserts and mounts the gastrostomy tube directly. EGD is performed, but because the gastrostomy tube does not pass through the mouth and esophagus, it can be performed even if the esophagus is narrow, and reduce the risk of infection, compared to the pull method.89 In this study, among the 7 out of 9 institutions that answered that the main method of implementation was the push method using an introducer, 7 institutions used the high-profile balloon-based tube from the time of the procedure, while 2 institutions used the low-profile balloon-based tube from the beginning. Although rare, using a balloon-based tube is more appropriate for preventing buried bumper syndrome.9 Some studies have reported that the bleeding rate is high in the push method, includes procedures such as gastropexy or introducers on the abdomen.10 However, a small-scale study comparing the pull and push methods in adults in Korea reported that there was no significant difference in infection or bleeding, and no buried bumper syndrome was reported.11 Another study comparing outcomes between primary gastrostomy tubes and buttons (G-tube and G-button) in pediatric patients reported that primary G-tube offers no significant advantage in overall, minor or major complications when compared to primary G-button.12 Large-scale studies comparing pull and push methods are required.
In this study, 61.3% of the procedures were performed together with fundoplication when required. SG is conducted when fundoplication is performed too or when PEG is expected to be difficult due to structural problems.2 SG may be advantageous for the operator because it is performed under general anesthesia. However, the duration of gastrostomy is relatively longer than that of PEG, and general anesthesia may cause dangerous situations depending on the patient’s general condition. In addition, the cost and recovery time after the procedure also has disadvantages compared with those of PEG.13 As in this survey, the priority consideration for pediatric gastrostomy procedures in Korea is PEG, and SG is selected in situations where PEG is difficult. SG has also been developed in a way that compensates for its limitations. Recently, laparoscopy has been used instead of open surgery, which leaves a large scar. However, fundoplication or gastrostomy using laparoscopy cannot shorten the procedure time or eliminate the need for general anesthesia, although a recent study reported that laparoscopic PEG may be safer than conventional PEG in high-risk pediatric patients with severe thoracoabdominal deformity, previous abdominal surgery, ventriculoperitoneal shunt, and abdominal tumors.1415 In addition, the difference in the procedures time depends more on the ability of the operator than on the procedure method. In this study, among the cases in which gastrostomy was performed again, there was a case in which the stormy site was placed too close to the pylorus, causing ballooning to interfere with gastric emptying. This may occur more often when open surgery is performed for gastrostomy in young children. Laparoscopy is more advantageous for site selection than open surgery. However, this complication can never occur in PEGs that focus on the stomach. Although the laparoscopic method is a recent trend in surgical procedures, it has inevitable disadvantages in terms of fundoplication. Fundoplication is a procedure in which the lower esophagus is wound around the muscle and tightened by the operator. Depending on the proficiency of the operator, reflux may continue because of tightening too loosely, and there may be cases where the liquids cannot be swallowed because of the tightening was too hard. Therefore, a recent study published in Korea reported that concomitant EGD during fundoplication was better than fundoplication alone regarding optimal tightness inside the esophagus.16
Compared to other countries, Korea has better access to pediatric endoscopy, and many pediatric endoscopy specialists are active in various parts of the country.17 According to the questionnaire data obtained in this study, it was observed that each center has implemented methods according to each hospital’s situation to reduce complications, procedure time, and costs. Thus, it was found that most centers did not have frequent complications and maintained the procedure method. Most of them recognized gastrostomy as an essential technique for children to improve the nutritional status of the patient, reduce the hospitalization rate, and impose great advantages on the clinical course.1819 Approximately 50% of the institutions used general anesthesia, which could be related to the sedation method of pediatric endoscopy. Most pediatric endoscopists are responsible for managing PEG and gastrostomy tubes. A 38.7% of the institutions did not consider fundoplication, and initially implemented PEG gastrostomy. For pediatric endoscopists, this survey showed that PEG is a safe procedure that should be considered as a first-line treatment. In addition, based on the results of this survey, a multicenter chart review of patients undergoing these procedures should be conducted.
 XML Download
XML Download