

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Inflammatory bowel disease (IBD) is characterized by chronic inflammation of the gastrointestinal tract. Approximately 25% of patients with IBD are diagnosed at younger than 20 years of age.1 Once IBD is diagnosed in children, the goals of therapy consist of eliminating symptoms, normalizing quality of life, restoring growth, and preventing complications while minimizing the adverse effects of medications.12 In addition, pediatric IBD has a more aggressive disease course than adult-onset disease. Therefore, early introduction of immunomodulators including anti-tumor necrosis factor (TNF) agents is required.34
Vedolizumab (VDZ) is a humanized monoclonal immunoglobulin (Ig) G1 antibody against α4β7-integrin that inhibits the binding of leukocytes to the endothelium of blood and lymphatic vessels located in the gastrointestinal tract. The gut-selective mechanism of action of VDZ has the advantage of greater safety compared to other biological agents.567 VDZ is currently approved in adults with CD and ulcerative colitis (UC).8910 Compared with adults, there is limited experience with VDZ therapy in pediatric IBD. Anti-TNF agents, such as infliximab (IFX) and adalimumab, are the only biological agents approved for usage in pediatric IBD, whereas VDZ is only available for off-label administration.1011
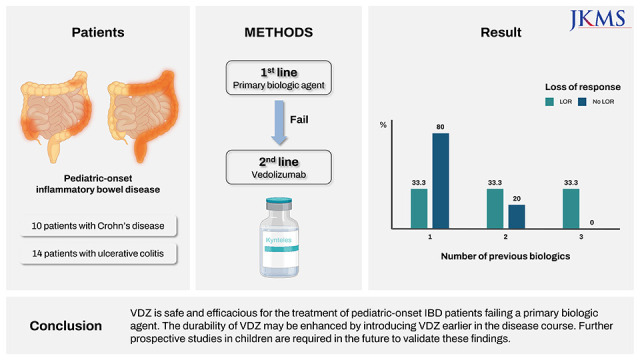
In the present study, we aimed to investigate the clinical course of pediatric-onset IBD following initiation of VDZ as more than a secondary biologic agent. We also aimed to identify factors associated with secondary loss of response (LOR) and durability of VDZ treatment.
Go to : 
METHODS
Patients and study design
This retrospective observational study was conducted at the Department of Pediatrics of two centers in Korea, between 2018 and 2020. Pediatric-onset IBD patients who had been diagnosed under 18 years of age who had received vedolizumab as more than a secondary biologic agent were included. Clinicodemographic data including sex, diagnosis age, age at VDZ start, disease type, number of biologics before VDZ, reason for changing to VDZ, clinical disease status at VDZ start were recorded at baseline. Factors such as age, duration from VDZ start, LOR during VDZ treatment, duration to LOR, concomitant medication, surgery during VDZ treatment, and sustained VDZ treatment were investigated at maximum follow-up. The primary outcome was rate of LOR during VDZ treatment and sustained VDZ treatment at last follow-up. Comparative analysis was conducted between groups divided according to the development of secondary LOR during VDZ treatment. Secondary LOR was defined as a worsening of clinical symptoms and a significant increase in CRP levels at two consecutive visits plus a status that required dose intensification. Dose intensification by interval shortening from 8 weeks to 4 weeks was conducted when secondary LOR occurred.
Statistical analysis
For comparative analysis between groups, the χ2 test or Fisher’s exact test were used for categorical variables and Student’s t-test or the Wilcoxon rank-sum test were used for continuous variables. Continuous variables are reported as medians with interquartile range or means with standard deviation. Kaplan-Meier survival analysis was used to determine rates of LOR to VDZ. Univariate and multivariate Cox proportional hazard regression analyses were used to evaluate factors associated with time-to-LOR during VDZ treatment and VDZ durability at 95% confidence level. Statistical significance was defined as P < 0.05. All analyses were conducted on SAS software version 9.4 (SAS Institute, Cary, NC, USA).
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Kyungpook National University Chilgok Hospital and informed consent was waived due to the retrospective nature of this study (IRB No. 2021-10-005).
Go to :
RESULTS
Baseline characteristics
Overall, 24 patients were included in this study. Ten patients had been diagnosed with CD and 14 patients with UC. The mean age at diagnosis was 14.6 ± 2.5 years. The mean age at initiation of vedolizumab was 20.5 ± 2.8 years. Three patients received off-label vedolizumab before the age of 18 years. The age of these patients was 15.9, 16.8, and 16.9 years, respectively. Nine patients (37.5%) had received two or more biologic agents before initiation of VDZ. Switching to VDZ occurred due to loss of response in 19 patients and due to adverse events during treatment with previous biologic agents in 5 patients (Table 1). Other baseline demographics and clinical characteristics are summarized in Table 1.
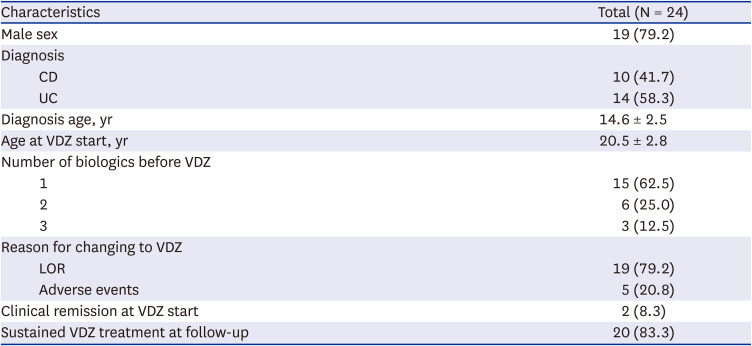
Table 1
Baseline characteristics
Values are expressed as mean ± standard deviation or number (%).
VDZ = vedolizumab, LOR = loss of response.
![]()
At maximum follow-up
During a median follow-up duration of 0.9 years after initiation of VDZ, 9 patients (37.5%) experienced loss of response requiring interval shortening. The median duration to LOR was 0.6 years. Eight patients received concomitant immunomodulators and 13 patients received concomitant mesalazine during VDZ treatment. One patient required bowel surgery and one patient underwent perianal surgery during VDZ treatment. At the last follow-up visit, 20 patients (83.3%) remained on VDZ treatment (Table 2).
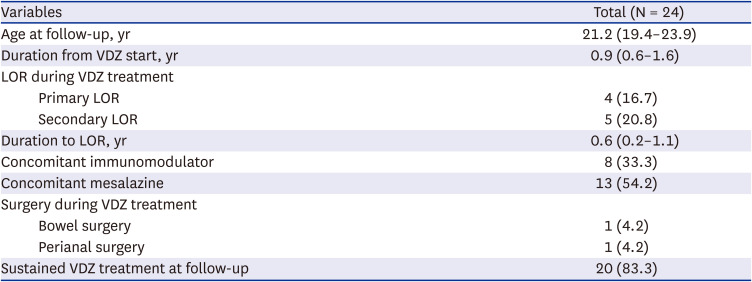
Table 2
At maximum follow up
Values are expressed as medians (interquartile range) or number (%).
VDZ = vedolizumab, LOR = loss of response.
![]()
Comparison between patients with and without LOR
The number of biologic agents received prior to VDZ therapy significantly differed between patients with and without LOR. In the group without LOR, 80% had received only one biologic agent before VDZ. Meanwhile, 33% of patients had received only one biologic agent before VDZ in the LOR group. There were no significant differences in other variables between the two groups (Table 3).
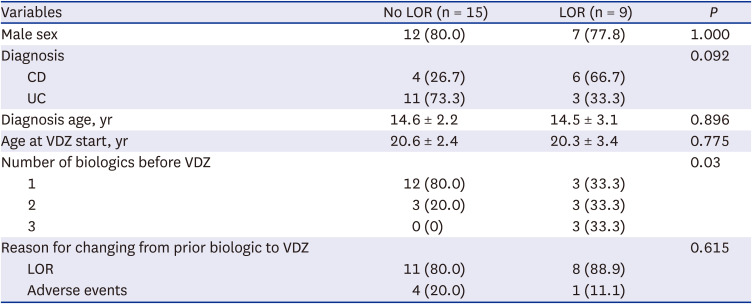
Table 3
Comparison between patients with and without LOR
Values are expressed as mean ± standard deviation or number (%).
LOR = loss of response; CD = Crohn’s disease, UC = ulcerative colitis, VDZ = vedolizumab.
![]()
Factors associated with time-to-LOR during VDZ treatment
Multivariate Cox proportional hazard regression analysis demonstrated a history of two or more biologic agents prior to VDZ treatment was the only factor associated with LOR (hazard ratio [HR], 5.6; 95% confidence interval [CI], 1.026–30.559; P = 0.047; Table 4).
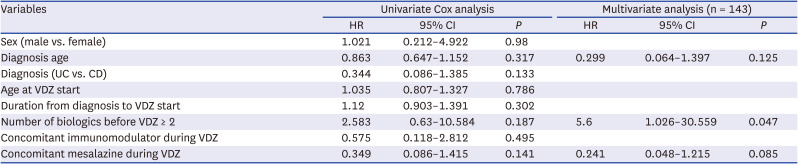
Table 4
Cox proportional hazard regression analysis of factors associated with time to LOR during VDZ treatment
LOR = loss of response, VDZ = vedolizumab, HR = hazard ratio, CI = confidence interval, UC = ulcerative colitis, CD = Crohn’s disease.
![]()
Factors associated with VDZ durability
A history of two or more biologic agents prior to VDZ treatment was the only factor negatively associated with VDZ durability (HR, 0.169; 95% CI, 0.043–0.656; P = 0.01; Table 5). No serious adverse events were observed during treatment with VDZ.
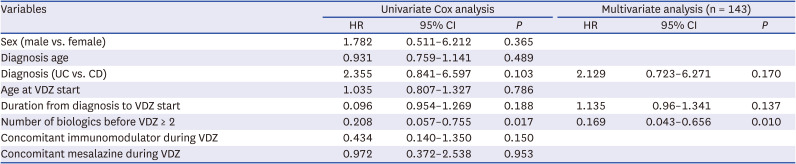
Table 5
Cox proportional hazard regression analysis of factors associated with VDZ durability
VDZ = vedolizumab, HR = hazard ratio, CI = confidence interval, UC = ulcerative colitis, CD = Crohn’s disease.
![]()
Go to :
DISCUSSION
Experience with VDZ treatment in pediatric IBD patients is limited compared with adults. In the present study, LOR was less frequent in those whom VDZ was introduced after one biologic than those in whom VDZ was introduced after more than one biologic agent. We found that the use of less biologics and earlier introduction of VDZ may reduce LOR and improve durability in pediatric-onset IBD patients. This is the first study to evaluate factors related to the LOR and durability of VDZ in patients with IBD diagnosed during childhood and adolescence.
According to the European Crohn’s and Colitis Organisation (ECCO)/European Society for Paediatric Gastroenterology Hepatology and Nutrition (ESPGHAN) guideline, although VDZ is currently not yet approved for use in children, VDZ may be considered as a second-line biologic therapy after anti-TNF failure in patients with chronically active or steroid-dependent pediatric UC.11 In addition, VDZ can be considered for off-label use in pediatric CD patients who are unable to maintain clinical remission on anti-TNF agents despite dose optimization and immunomodulator use, or in situations of severe tuberculosis infection.1012 In an observational prospective cohort study of children with refractory IBD who had failed anti-TNF therapy prior to initiation of VDZ therapy, clinical response was observed in 31.6% at week 6 and 57.9% by week 22. Steroid-free remission was seen in 5% of subjects at 6 weeks, 15% at 14 weeks, and 20% at 22 weeks.13 A multicenter retrospective study showed that VDZ was safe and effective in children with IBD. This study included 64 children with IBD who had previously been treated with anti-TNF agents. Remission without corticosteroid was seen in 37% and 39% of UC patients and 14% and 24% of CD patients at week 14 and at final clinic visit (median follow-up period of 24 months), respectively.14 Another retrospective study of 52 children with IBD included 5 anti-TNF-naïve patients. At week 14, clinical remission was observed in 76% of UC patients and 42% of CD patients. At week 22, anti-TNF-naïve patients had higher remission rates than anti-TNF exposure patients (100% vs. 45%; P = 0.04).15 These studies of VDZ treatment in pediatric IBD demonstrate VDZ as effective and safe in children. Studies of VDZ in very early-onset IBD (VEO-IBD) are even more limited. In a study of the safety and efficacy of VDZ in VEO-IBD (defined as aged < 6 years), 56.3% patients had clinical response at 14 weeks. Further, there was improvement in nutritional state including body mass index.16
LOR to biologic therapy is a relatively common issue in clinical practice. LOR may occur due to factors such as antibody formation, changes in drug clearance, and non-TNF-induced inflammatory mechanisms.17 Accordingly, it is important to be able to predict and manage LOR to biologics. In our study, the median duration to LOR was 0.6 years and 9 patients (37.5%) experienced LOR requiring interval shortening. There are limited previous studies regarding predictors of LOR to VDZ in adults. A retrospective study including a total of 788 IBD patients treated with VDZ reported rates of LOR to VDZ of 20% at 6 months and 35% at 12 months. In that study, LOR to anti-TNF agents prior to VDZ administration was associated with an increased risk of LOR to VDZ and higher baseline serum C-reactive protein level was reported as an important predictor of LOR.18
In our study, the number of biologics received prior to initiation of VDZ was found to be associated with LOR. Predicting response and LOR to biologics is clinically challenging. Previous studies reporting predictive factors of response to biologic therapy in patients with IBD remain controversial,192021 and there is currently no clear consensus regarding patient-related and disease-related factors. For VDZ, no single prognostic indicator has yet been reported, although a scoring system to predict outcomes of VDZ treatment has been recently developed and validated.2223242526272829
Although the reason for changing to VDZ was not identified as a statistically significant factor in our study, a study by Singh et al.30 found that response to second-line biologics differed depending on the reason for discontinuing primary therapy in patients with IBD. In this study, patients with primary non-response to anti-TNF agents were less likely to respond to secondary non-TNF biologics compared to patients who discontinued treatment for secondary LOR or intolerance. In another study comprising 41 patients in clinical remission, switching from anti-TNF agents to VDZ for reasons other than LOR was analyzed. Most patients switched treatment due to adverse events (56.1%) or infection (14.6%). After change, follow-up endoscopy was performed in 30 patients, with 25 patients (83.3%) confirmed to be in endoscopic remission.31 In the GENIMI 1 study, rates of response to VDZ and placebo at week 6 were 53.1% and 26.3%, respectively, in patients with naïve to anti-TNF and 39.0% and 20.6%, respectively, in patients with anti-TNF failure. At week 52, rates of remission with VDZ and placebo were 46.9% and 19.0%, respectively, in patients naïve to anti-TNF, and 36.1% and 5.3%, respectively, in patients with anti-TNF failure.32 The GEMINI 2 and 3 trials evaluated 516 anti-TNF naïve patients and 960 anti-TNF failure patients and reported 48.9% of anti-TNF naïve and 27.7% of anti-TNF failure patients were in remission with VDZ at week 52.33 These results may be due to differing pharmacokinetics and pharmacodynamics of anti-TNF agents in individual patients.
Pediatric IBD has a complex and aggressive disease course.1 Therefore, timely and appropriate treatment is essential to prevent deterioration that may require surgical intervention. In the treatment of pediatric IBD, it is most important to maintain growth and minimize drug side effects in addition to controlling symptoms. In this study, no serious adverse events were observed during VDZ treatment, corroborating previous studies of VDZ in pediatric IBD.131415 Only one patient underwent bowel surgery and 20 patients (83.8%) had sustained VDZ treatment at the final follow-up visit.
This study has several limitations. First, this study had a retrospective design and was limited by a small sample size. Thus, caution is required when interpreting the results of this study. Although, we had concluded that the durability of VDZ may be enhanced by introducing VDZ earlier in the disease course, the reason that VDZ was not efficacious in those with a previous treatment history of various biologics may be merely due to the fact that the disease severity of these patients was severe to not respond to any biologics. Larger prospective studies in pediatric IBD are warranted. Second, a further limitation is that selection bias may have occurred. Third, data on the application of VDZ in young children were insufficient. Only three patients used off-label VDZ before the age of 18 years. Evaluation of the safety and efficacy of VDZ at younger ages would require licensing approval and further research. Furthermore, data regarding growth could not be evaluated in the present study since patients were mainly young adults. The effect of VDZ on patient growth, an important pediatric consideration, should be evaluated through long-term follow-up in pediatric patients with IBD.
The findings of the present study demonstrate VDZ as safe and efficacious for the treatment of pediatric-onset IBD in patients failing a primary biologic agent. The durability of VDZ may be enhanced by introducing VDZ earlier in the disease course. Future prospective studies in children are required to validate the findings of the present study.
Go to :
 XML Download
XML Download