

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The novel coronavirus (severe acute respiratory syndrome coronavirus 2 [SARS-CoV-2]) infection started in Wuhan, China in December 2019 and is spreading rapidly worldwide.12 In Korea, since the first confirmed case of coronavirus disease 2019 (COVID-19) in January 2020, cases have been continuously occurring.3 COVID-19 can show a variety of symptoms from asymptomatic to severe clinical symptoms, and the main symptoms include fever, sore throat, respiratory symptoms, muscle pain and headache; loss of smell and taste may appear.4 As this infection spreads rapidly around the world, the WHO has declared COVID-19 a pandemic. Although there are differences by country and region, COVID-19 has a higher hospitalization rate and mortality than expected and is more contagious than the new infectious diseases, severe acute respiratory syndrome, and Middle East respiratory syndrome.15
It is known that COVID-19 patients with chronic underlying diseases are more likely to progress to severe diseases.67 In patients with inflammatory bowel disease (IBD) who are using various immunomodulatory drugs, COVID-19 causes many concerns about the treatment of existing IBD, as well as complications from the infection.8 Due to thorough defense measures (COVID-19 prevention and control measures), many infectious diseases in pediatric patients have declined, and it is estimated that the frequency of chronic diseases incurred in this regard will be reduced.9 However, there is also a lack of studies on how the COVID-19 pandemic has affected IBD, especially pediatric patients (PIBD).
This study aimed to determine whether the occurrence, characteristics, initial treatment, and short-term course of PIBD patients changed due to the COVID-19 epidemic compared with the previous period. This study collected data from patients with PIBD in 17 local Korean institutions, and was the first report to study the epidemiology of COVID-19 in PIBD centers nationwide, although with a reduced number of patients. In addition, it is hoped that this multicenter study will contribute to the proper diagnosis and treatment of PIBD in the special era of the COVID-19 pandemic.
METHODS
Patients and methods
This multicenter, retrospective study was conducted in the Department of Pediatrics of 17 medical centers nationwide from January 2018 to June 2021. The subjects included in this study were pediatric patients under 18 years of age diagnosed with IBD, including Crohn’s disease (CD) and ulcerative colitis (UC), within the past 3 years. Patients without a colonoscopy, those without a confirmed Paris classification, and those for whom information could not be obtained due to poor medical records at diagnosis were excluded.
Demographic data collected included age at diagnosis, sex, height, weight, body mass index, distance from home to a hospital, and family history of IBD. Clinical information, such as initial major symptoms, symptoms at diagnosis, duration from symptom recognition to first hospital visit, duration from initial hospital visit to diagnosis, disease activity at diagnosis, endoscopic severity, disease phenotypes, laboratory tests, and fecal calprotectin results, was obtained from medical records. In addition, to determine the short-term course, drug treatment, disease activity, laboratory tests, and fecal calprotectin results were investigated at the initial stage of diagnosis and at the 6th and 12th months after diagnosis, respectively.
Disease classification and behavior were based on the Paris Classification. Disease activity was evaluated using the Pediatric Crohn’s Disease Activity Index (PCDAI) and Pediatric Ulcerative Colitis Activity Index (PUCAI).1011 To investigate endoscopic severity, we used the Simple Endoscopic Score for Crohn’s Disease (SES-CD) for patients with CD and the Modified Mayo Endoscopic Score for patients with UC.1213
The trend in the number of PIBD for 3 years was confirmed at 6-month intervals, and we compared the disease characteristics, initial treatment, and short-term course of the two groups by dividing patients diagnosed before and after January 2020, when COVID-19 began in Korea.
Statistical analysis
For statistical comparison between groups, Student’s t-test or Mann-Whitney U test was used for continuous variables, and a χ2 test or Fisher’s exact test was used for categorical variables. Comparative data for continuous variables are reported as means and standard deviations. Data were considered statistically significant if the P value was < 0.05. All statistical analyses were performed using the R software (version 4.0.2).
RESULTS
Baseline characteristics
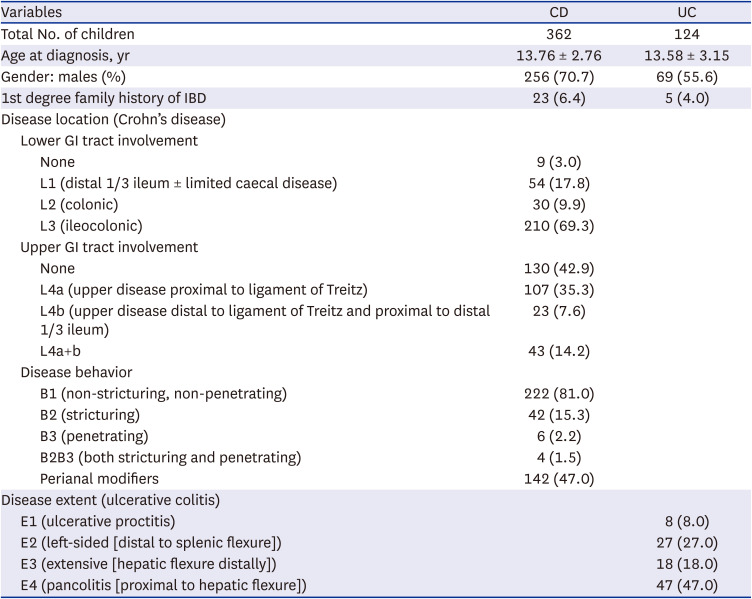
A total of 486 patients from 17 institutions were included: 362 (74.5%) patients with CD and 124 (25.5%) patients with UC. The baseline patient characteristics are presented in Table 1. The mean age at diagnosis was 13.8 years for CD and 13.6 years for UC patients. The 1st degree family history of IBD was 6.4% for CD, and 4.0% for UC. In CD, ileocolic involvement was found in 69.3% of patients; 42.9% of the cases did not have upper involvement, and perianal lesions were found in 47.0% of patients at diagnosis. In UC, 47.0% of the patients had a disease extent of pancolitis (Table 1).
Table 1
Baseline characteristics of pediatric inflammatory bowel disease
The occurrences of PIBD in the last 3 years in Korea
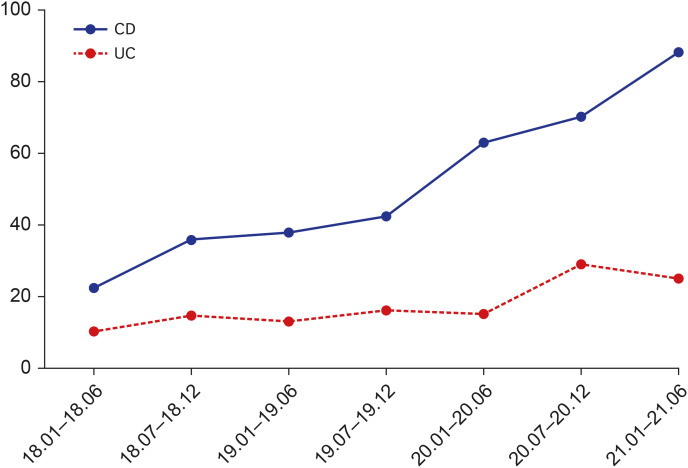
Fig. 1 shows the number of cases of PIBD who occurred during the 6-month intervals from January 2018 to June 2021 (Fig. 1). Although the number of children and adolescents in Korea has been decreasing every year, the number of patients diagnosed with CD and UC has gradually increased (139 to 223 in CD, 54 to 70 in UC), even after the COVID-19 era (Table 2).

Comparison of disease characteristics before and after the COVID-19 era in CD
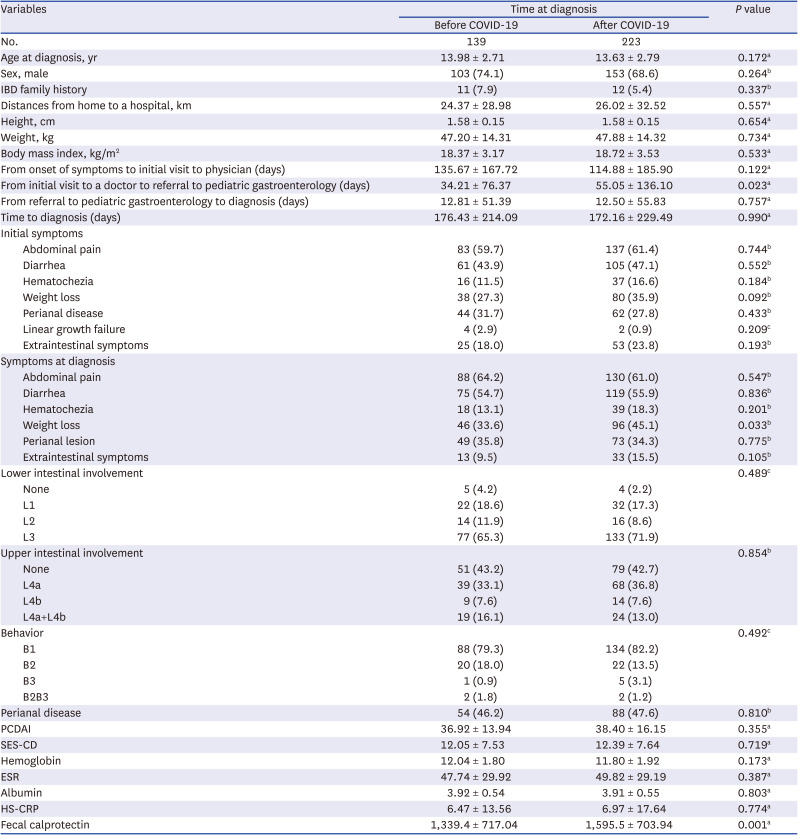
In CD patients, the duration from the initial visit to a primary care physician to the pediatric gastroenterologist referral was significantly longer after the COVID-19 era than before (34.21 ± 76.37 vs. 55.05 ± 136.10 days, P = 0.023) (Table 3). However, there was no significant difference in the total duration from the initial symptoms to diagnosis (176.43 ± 214.09 vs. 172.16 ± 229.49 days, P = 0.990). Both before and after the COVID-19 pandemic, the main symptoms were abdominal pain and diarrhea. Weight loss was significantly more common in patients diagnosed after the COVID-19 pandemic (33.6% vs. 45.1%, P = 0.033). There were no differences in the sites of gastrointestinal tract involvement, perianal lesions, laboratory tests, PCDAI, and SES-CD according to the time of diagnosis. The fecal calprotectin level was significantly higher in patients diagnosed after the COVID-19 era (1,339.4 ± 717.04 vs. 1,595.5 ± 703.94, P = 0.001) (Table 3).
Table 3
Epidemiological trends of and initial management before and after COVID-19 in Crohn’s disease
Shapiro-Wilk’s test was employed to assess the normality assumption.
COVID-19 = coronavirus disease 2019, IBD = inflammatory bowel disease, PCDAI = Pediatric Crohn’s Disease Activity Index, SES-CD = Simple Endoscopic Score for Crohn’s Disease, ESR = erythrocyte sedimentation rate, HS-CRP = high-sensitivity C-reactive protein.
aP values were derived from the Mann-Whitney’s U test; bP values were derived from χ2 test; cP values were derived from Fisher’s exact test.
Comparison of disease characteristics before and after the COVID-19 era in UC
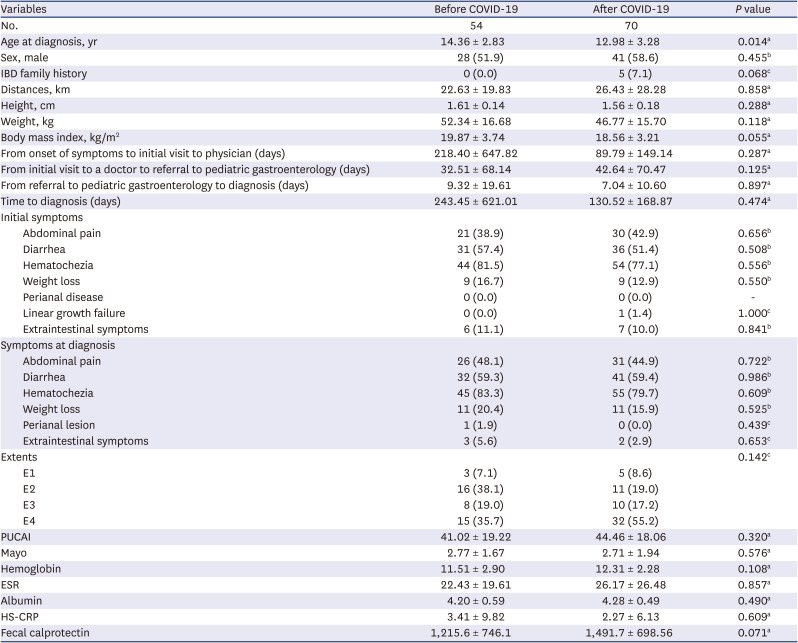
In UC, the mean age of patients diagnosed after COVID-19 era was significantly lower (14.36 ± 2.83 vs. 12.98 ± 3.28 years, P = 0.014) (Table 4). There were no significant differences between the initial symptoms and laboratory test results. Fecal calprotectin levels after and before COVID-19 era were also not significantly different (1,215.6 ± 746.1 vs. 1,491.7 ± 698.56, P = 0.071) (Table 4).
Table 4
Epidemiological trends and initial management before and after COVID-19 in ulcerative colitis
Shapiro-Wilk’s test was employed to assess the normality assumption.
COVID-19 = coronavirus disease 2019, IBD = inflammatory bowel disease, PUCAI = Pediatric Ulcerative Colitis Activity Index, ESR = erythrocyte sedimentation rate, HS-CRP = high-sensitivity C-reactive protein.
aP values were derived from the Mann-Whitney’s U test; bP values were derived from χ2 test; cP values were derived from Fisher’s exact test.
Initial management before and after the COVID-19 era
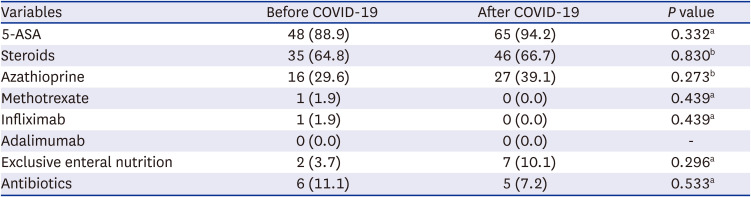
In the initial treatment of CD, patients diagnosed before the COVID-19 era mainly used 5-aminosalicylic acid (5-ASA) (78.4%) and steroids (51.1%), whereas patients diagnosed after the COVID-19 era, the use of 5-ASA (68.8%) and steroids (33.5%) decreased significantly (P = 0.046, P = 0.001), as did the use of infliximab (13.7% vs. 5.4%, P = 0.007) (Table 5). Exclusive enteral nutrition (EEN) has increased significantly in patients diagnosed with COVID-19 (46.8% vs 60.6%, P = 0.010). There was no significant difference in the initial management of UC before or after the COVID-19 pandemic (Table 6).
Table 5
Initial treatment trends before and after COVID-19 in Crohn’s disease (N = 362)
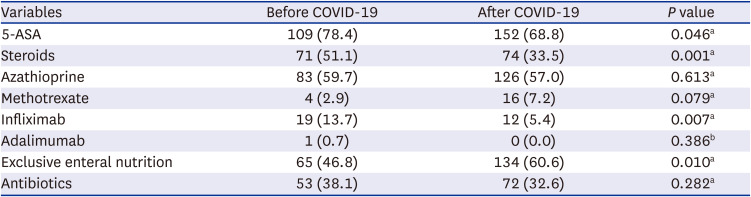
Table 6
Initial treatment trends before and after COVID-19 in ulcerative colitis (N = 124)
Short-term course of PIBD before and after the COVID-19 era
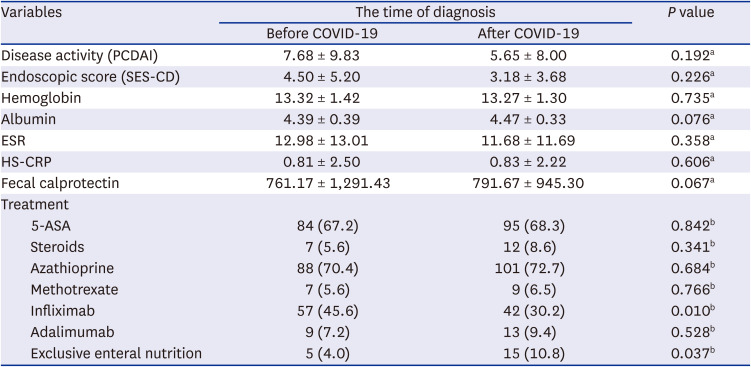
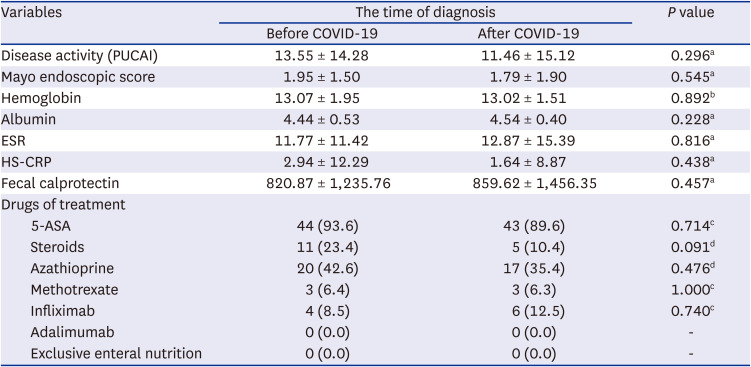
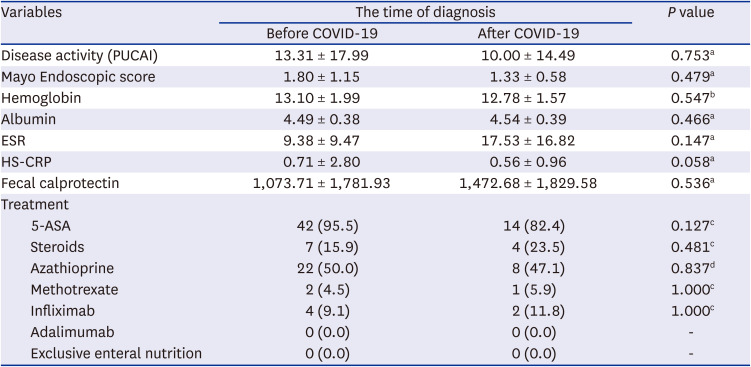
Six months after diagnosis, disease activity and endoscopic severity according to the time of diagnosis did not differ between CD and UC (Tables 7 and 8). In CD, regarding the treatment at 6 months after diagnosis, significantly fewer patients diagnosed after the coronavirus era were using infliximab (45.6% vs. 30.2%, P = 0.01) and more patients received EEN (4.0% vs. 10.8%, P = 0.037) than those diagnosed previously. Even 12 months after diagnosis, infliximab use was significantly lower in patients diagnosed after the COVID-19 era than in those diagnosed before (55.7% vs. 32.8%, P = 0.003). A comparison of the short-term courses at 12 months after diagnosis is shown in Tables 9 and 10.
Table 7
Comparison of short-term courses at 6 months after diagnosis according to the time of diagnosis in Crohn’s disease (N = 264)
Shapiro-Wilk’s test was employed to assess the normality assumption.
COVID-19 = coronavirus disease 2019, 5-ASA = 5-aminosalicylic acid, ESR = erythrocyte sedimentation rate, HS-CRP = high-sensitivity C-reactive protein, PCDAI = Pediatric Crohn’s Disease Activity Index, SES-CD = Simple Endoscopic Score for Chron’s Disease.
aP values were derived by Mann-Whitney’s U test; bP values were derived from χ2 test.
Table 8
Comparison of short-term courses at 6 months after diagnosis according to the time of diagnosis in ulcerative colitis (N = 95)
Shapiro-Wilk’s test was employed to assess the normality assumption.
COVID-19 = coronavirus disease 2019, 5-ASA = 5-aminosalicylic acid, ESR = erythrocyte sedimentation rate, HS-CRP = high-sensitivity C-reactive protein, PUCAI = Pediatric Ulcerative Colitis Activity Index.
aP values were derived by Mann-Whitney’s U test; bP values were derived from independent t-test; cP values were derived from Fisher’s exact test; dP values were derived from χ2 test.
Table 9
Comparison of short-term courses at 12 months after diagnosis according to the time of diagnosis in Crohn’s disease (N = 179)
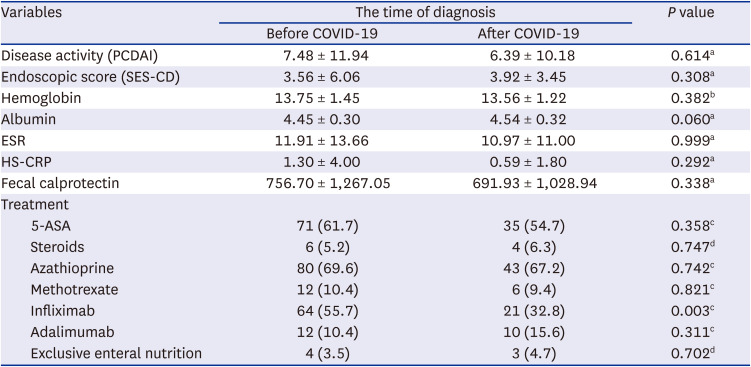
Shapiro-Wilk’s test was employed to assess the normality assumption.
COVID-19 = coronavirus disease 2019, 5-ASA = 5-aminosalicylic acid, ESR = erythrocyte sedimentation rate, HS-CRP = high-sensitivity C-reactive protein, PCDAI = Pediatric Crohn's Disease Activity Index, SES-CD = Simple Endoscopic Score for Chron’s Disease.
aP values were derived by Mann-Whitney’s U test; bP values were derived from independent t-test; cP values were derived from χ2 test; dP values were derived from Fisher’s exact test.
Table 10
Comparison of short-term outcomes at 12 months after diagnosis according to the time of diagnosis in ulcerative colitis (N = 61)
Shapiro-Wilk’s test was employed to assess the normality assumption.
COVID-19 = coronavirus disease 2019, 5-ASA = 5-aminosalicylic acid, ESR = erythrocyte sedimentation rate, HS-CRP = high-sensitivity C-reactive protein, PUCAI = Pediatric Ulcerative Colitis Activity Index.
aP values were derived by Mann-Whitney’s U test; bP values were derived from independent t-test; cP values were derived from Fisher’s exact test; dP values were derived from χ2 test.
Transfer rates during the last 3 years beyond the COVID-19 era
At the time of diagnosis, it was confirmed that the movement to other hospitals (voluntary transfer) decreased from 12.2% to 8.5%, when the COVID-19 pandemic started in patients with CD. However, no statistically significant differences were observed (Table 11). In patients with UC, the transfer rate decreased from 11.5% to 4.6%, when the COVID-19 pandemic started. There were no statistically significant differences between the groups (Table 11).
Table 11
Transfer rates according to the time of diagnosis in patients with Crohn’s disease and ulcerative colitis

DISCUSSION
In this study, the incidence of PIBD, CD, and UC, increased, despite the decline in the number of children and adolescents after the COVID-19 era. The incidence of PIBD has dramatically increased over the past 20 years. Although the incidence of PIBD varies from region to region around the world, the incidence of PIBD has been showing a steadily increase, and is also characterized by a sharp increase, especially in Asia.141516 According to a systematic review article, the incidence rates of IBD, CD, and UC in Asia were 0.5–11.4, 0.3–3.7, and 0.2–3.9 per 100,000 person-years from 1968 to 2012, respectively.15 Therefore, the increased incidence rate in this study can be explained as an extension of the existing increasing pattern. It should also be taken into account that the recent small family size raises concerns and interest in children's health and symptoms, and as access to medical services has improved, many evaluations to exclude IBD are being conducted. The increase in PIBD medical care due to the increase in pediatric endoscopy specialists and active tests to find patients more than in the past would have played a role. I also think that the development of the transfer system, which is suspected of PIBD and transported to a center that can be treated, also played a big role in increasing the incidence of PIBD. There should be more attention and research by clinicians on the increasing number of patients with PIBD, even though there has been a decrease in the population of children and adolescents due to a reduced birth rate in Korea, the overall frequency of general pediatric diseases is also decreasing.
Another point to consider is the impact of the COVID-19 pandemic. Lifestyle changes in the post-COVID-19 era may have contributed to this increase. COVID-19 has affected the incidence of various pediatric diseases. Infection-associated diseases in children have decreased and childhood obesity has increased.1718 This is a result of not only complying with quarantine rules but also due to a lack of activity, such as an increase in the time spent at home. In addition, if there was a change in the composition of intestinal microflora due to an increase of the use of food delivery services and intake of processed food, it would be associated with an increase in PIBD incidence. Changes in intestinal microflora are known to be closely related to the occurrence of IBD, and it has not yet been established as a standard treatment; however, efforts are being made to apply it to the treatment of IBD. Considering the influence of the increased number of pediatric obesity patients and the increase in the occurrence of PIBD as COVID-19 progresses, we believe that the cause and treatment of PIBD will contribute to the development of an improved PIBD management.19
Clinical manifestations of PIBD may include common symptoms such as abdominal pain, hematochezia, and weight loss, but in many cases, atypical symptoms such as linear growth failure and extraintestinal symptoms may be present.20 When comparing the disease characteristics before and after the COVID-19 era in our study, the most common clinical symptoms at initial diagnosis were abdominal pain and diarrhea in CD and hematochezia in UC, and there was no statistically significant difference between the two groups. Characteristically, weight loss was significantly more common after the COVID-19 era as a symptom of CD. In the case of weight loss, which may be relatively inconspicuous compared to other symptoms, it is possible that the detection was delayed because weight was not measured in circumstances such as isolation and restrictions on school attendance in the COVID-19 era. Weight loss is a relatively common symptom in PIBD, especially CD. However, if it is detected late and does not recover properly, it will lead to a decrease in the final adult height.2122 Therefore, early detection of weight loss is an important aspect that should not be overlooked.
In addition, the period from the primary care visit to the referral to a pediatric gastroenterologist was significantly longer after the COVID-19 era, indicating that there were some restrictions on transfer to tertiary referral hospitals during this period. It may be difficult to treat other diseases at referral hospitals owing to the COVID-19 pandemic. It is also possible that because of concerns regarding the spread of COVID-19, the patient hesitated to visit a tertiary hospital despite showing symptoms. In addition, during the COVID-19 era, the delay can have contributed to the increasing proportion of weight loss that progresses and persists slowly over time. One of the reasons for mainly selecting local PIBD centers in Korea, was to identify patients who were transferred to big centers in Seoul immediately after diagnosis. The results of the study showed that there was no significant differences in both CD and UC patients, however, before COVID-19, about one in ten patients were transferred, but due to restrictions on movement during the COVID-19 era, it is thought that only about one in six patients were transferred. In addition, children's transfers were not impacted by the pandemic, as expected in this study, and it was confirmed that the treatment was being conducted efficiently in local centers in Korea.
After the COVID-19 era, the use of steroids decreased and that of EEN increased during the initial treatment of CD. According to the guidelines of ECCO/ESPGHAN, EEN is recommended as a first-line treatment to induce remission in children with active luminal CD.2324 In several previous studies, EEN was confirmed to be effective in the treatment of pediatric CD to replace the effect of steroids.25 It reduces proinflammatory microbial components, which reduces inflammatory damage to the gut. EEN-induced remission is significant in the modulation of the gut microbiota.26 EEN induction is effective in activating early clinical, biochemical, mucosal, and transmural remission in children with luminal CD. Early complete mucosal healing with EEN predicts sustained remission and improves outcomes.27 On the other hand, the use of infliximab decreased in both CD and UC, which could be attributed to restrictions on the application of biologics due to concerns about infection in the COVID-19 era and further changes in domestic insurance policies. This results did not reflect recent treatment trends favoring top-down strategies. It is necessary to elucidate whether this result was a temporary decrease due to concerns about infection in the early stages of COVID-19 or whether it was due to restrictions on use due to the strengthening of medical insurance standards unique to Korea through additional long-term research. This study has shown that the direction of PIBD treatment in Korea is gradually changing, and that through active research and consultation, medical workers should also create optimal guidelines that consider the domestic situation.
Several adult studies have found that IBD is not a risk factor for COVID-19 infection.28 However, the COVID-19 pandemic has changed the treatment approach in patients with IBD. In actual clinical practice, there is a tendency to hesitate and stop using biologics and immunomodulators in patients with IBD.29 According to published guidelines, the use of biologics and immunomodulators should not be stopped or dose reduced, and steroids should be reduced whenever possible.30 The reduction of these treatments in the era of COVID-19 is highlighted more in pediatric IBD patients, where safety is more important. Nevertheless, no guidelines have been optimized for pediatric IBD. Based on experiences in the COVID-19 era, a revised treatment guideline for pediatric IBD is needed so that treatment can be appropriately intervened at an appropriate time without delay. Even if it is not related to the COVID-19 era, the use of biologics, which are currently used in adults due to problems such as insurance, is also very limited for patients with PIBD in Korea.
A limitation of this study is that it was a retrospective medical record study, and the recorded endoscopic score or the activity of the disease may be somewhat subjective, and it may have some errors regarding the use of biologic insurance coverage. There were many limitations in the data: reporting the exact time point reaching clinical remission (PCDAI or PUCAI < 10) and accurately reporting mucosal healing (SES-CD:0 or below 3). However, for the first time, the latest data was collected from as many PIBD centers as possible in Korea. In this study, large centers in Seoul were excluded, and there is a limitation in that the largest number of PIBD patients data were omitted, however, we think this is a problem that the domestic registry can address through follow-up studies. In addition, this study is meaningful because it examines the domestic PIBD trends before and after COVID-19, however, it is believed that it shows the current status of rapidly changing PIBD regardless of COVID-19, and for this reason, continuous follow-up research is needed. This study will serve as the basis for a large-scale multicenter follow-up study, and it is hoped that it can help stablish the PIBD registry in Korea.
In conclusion, this study confirmed that the incidence of PIBD in Korea is steadily increasing despite a rapid decline in the birth rate. The initial management of PIBD continues to change, and it is reasonable to see that this is due to the characteristics of chronic diseases that are repeated by the heterogenicity of PIBD rather than the influence of the COVID-19 era. Especially in children, growth periods should be considered, and if not handled appropriately, they can lead to growth failure. In Korea, early diagnosis and optimal guidelines are essential for children with PIBD.
 XML Download
XML Download