

 PDF
PDF Citation
Citation Print
Print



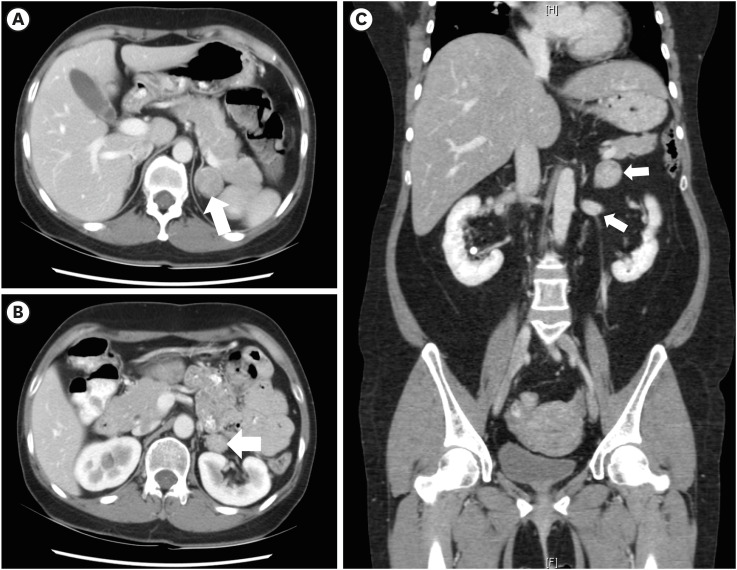
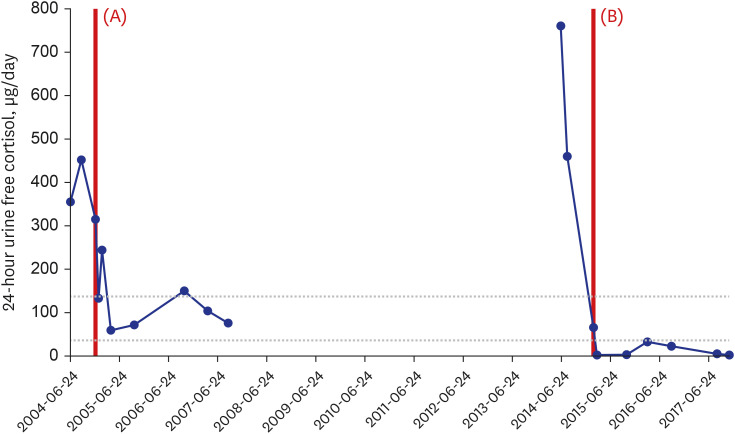
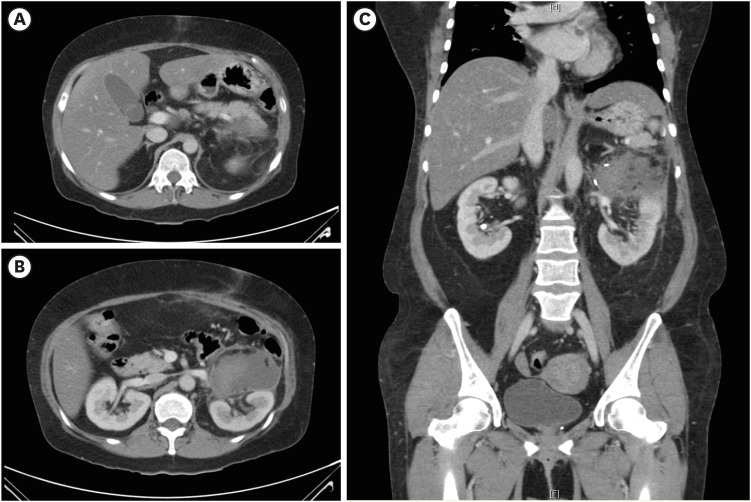
A 42-year-old woman with history of diabetes mellitus (DM), hyperlipidemia and subclinical hypercortisolism with previous left adrenalectomy was admitted for the evaluation of recurrent hypercortisolism due to gain of weight (8 kg over 3 months).1 The woman was on oral diabetic and hypertension medication (metformin, glimepiride, losartan, and amlodipine), without exposure of exogenous glucocorticoid. The woman had no familial history of hypercortisolism. Plasma ACTH levels at 8 A.M. and 4 P.M. were within normal range (16.2 pg/mL and 18.0 pg/mL, respectively), but 24-hour urine free cortisol was elevated (760.5 μg/day). A 3 × 2 cm mass on lower surgical bed level of previously resected left adrenal region was found in abdominal CT and showed increased uptake in 131I-iodocholesterol (NP-59) scan. Suggestive of adrenocortical adenoma, left adrenal mass was resected and pathology was concordant with adrenocortical adenoma. Follow-up abdominal CT 1 week after second left adrenalectomy showed left adrenal gland removed state with hematoma.
In this case, ipsilateral adrenal mass beside primary lesion was noticed in CT (Fig. 1) after the patient developed overt hypercortisolism after 10 years of previous left partial adrenalectomy.2 The 24-hour urine free cortisol was normalized after first adrenalectomy but increased after 10 years as shown in Fig. 2, suggesting that initially undetected adrenal mass changed its nature from subclinical to overt hypercortisolism over 10 years. Clinical presentation of hypercortisolism was resolved after second adrenalectomy (Fig. 3) and postoperative glucocorticoid treatment (hydrocortisone 40mg/day PO) was required.3 The level of 24-hour urine free cortisol decreased to 32.5 μg/day (normal range; 37–136 μg/day) in 1 year after second left adrenalectomy and the level of 8 A.M. plasma ACTH level increased to 52.8 pg/mL (normal range; 7.2–63.3 pg/mL) in 3 years after second left adrenalectomy.
 XML Download
XML Download