

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
A cough is a protective reflex of the airway against aspiration and irritation. However, a dysregulated cough reflex has a significant physical, social, and psychological burden on the population.1 Recently, cough hypersensitivity syndrome (CHS) was proposed for chronic cough in adults and endorsed by the European Respiratory Society (ERS) task force.2 Chronic cough is not a disease-related condition but a clinical syndrome characterized by troublesome coughing often triggered by low levels of thermal, mechanical, or chemical exposure.34 Thus, CHS is a unifying paradigm that includes diverse groups of patients with chronic cough and helps clarify unexplained cough. The clinical approach with the CHS paradigm includes the identification of potentially treatable traits, such as eosinophilic inflammation in the lower airways, nasal inflammation, and gastroesophageal reflux, and the use of cough control treatment including pharmacological or non-pharmacological interventions.345 Codeine and levodropropizine have been widely prescribed for cough management in Korea. Codeine is a centrally acting antitussive agent and prodrug of morphine,6 whereas levodropropizine is a peripheral antitussive agent, which may act by inhibiting C-fibers secreting protussive neuropeptides.7 Previous meta-analyses have suggested that codeine and levodropropizine provide better antitussive effects than placebo in adults. However, they had small sample sizes, and relatively few good-quality studies drew conclusions about the relative efficacy of codeine and levodropropizine.789 Moreover, limited data have been provided on the use of codeine and levodropropizine as antitussives in chronic cough, particularly in Asian populations.
We hypothesized that codeine would reduce coughing and promote more positive clinical outcomes in unselected patients with chronic cough than levodropropizine. This study aimed to assess the effectiveness and safety of codeine and levodropropizine in adult patients with chronic cough. The effectiveness of codeine was examined by analyzing the changes in common cough assessment tools, including the cough visual analog scale (VAS), Cough Symptom Score (CSS), and the Leicester Cough Questionnaire (LCQ).
METHODS
Study design and intervention
We conducted an open-label comparative trial with participants with chronic cough. The participants were administered codeine and levodropropizine for 2 weeks at a single tertiary referral center (Gachon University Gil Medical Center in Incheon, Korea).
Patients
Patients with a persistent cough for more than 8 weeks, who visited a specialist cough clinic for the first time at a tertiary hospital, were consecutively screened for eligibility during outpatient visits. The inclusion criteria in this study were chronic cough patients who had not received antitussive treatment before their initial visit to the referral clinics and those with unresolved coughing after smoking cessation for at least 4 weeks or medication for comorbidities within a primary care setting. Participants who had recent respiratory tract infections, underlying lung disorders such as pulmonary tuberculosis, pneumonia, emphysema, bronchiectasis, and lung cancer, or those administered medications that could influence coughing and interact with antitussives were excluded from this study. After enrollment, all participants were assessed according to anatomic diagnostic protocols in the guidelines for chronic cough.10 They underwent investigation for a differential diagnosis, including chest radiography, lung function test, allergy testing through the skin or blood testing for specific immunoglobulin E (IgE) against potential allergens, methacholine bronchial challenges, or fractional exhaled nitric oxide (FeNO). Using a combination of history, physical examination, and laboratory assessments, identifiable conditions presumed to contribute to cough were investigated. Thereafter, a successful response to treatment was considered as confirmation of the diagnosis. For this analysis, chronic cough patients were classified into “Upper airway cough syndrome” (patients with chronic rhinitis or rhinosinusitis), “Asthmatic cough” (patients with airway eosinophilia and good response to corticosteroid therapy), and “Unexplained cough” (patients with an unknown etiology after thorough investigation for common cough-triggering conditions and therapeutic trials) groups. Patients with cough-variant asthma (CVA) and non-asthmatic eosinophilic bronchitis (NAEB) were included in the asthmatic cough group. CVA was defined as chronic cough with bronchial hyperresponsiveness and variable airflow obstruction, and NAEB was defined as chronic cough with an absence of symptoms or objective evidence of variable airflow obstruction, airway hyperresponsiveness, and airway eosinophilic inflammation related to high FeNO levels.1112 Patients were directed to answer a structured questionnaire that obtained information on demographic characteristics, cough severity (100-mm linear VAS and CSS), and cough-related quality of life (LCQ).13141516 Using antitussives with standard treatment of the confirmed cause of chronic cough poses difficulties in ascertaining which treatment improved the symptoms. Therefore, we initiated a clinical trial using antitussives without the standard treatment for chronic cough. The test drugs were administered before the standard treatment of the confirmed cause of chronic cough. After the trial period, all patients were treated with standard therapy, depending on their diagnosis and condition.
Study design
No formal calculation was performed for sample size, given the unavailability of previous data on patients with chronic cough to evaluate the effectiveness of codeine and levodropropizine. For codeine or levodropropizine administration, patients were allocated in equal proportions following simple randomization performed in Excel 2010 (Microsoft Corp., Redmond, WA, USA).
Every 8 hours, the participants were orally administered 20 mg of codeine or 60 mg of levodropropizine. All effectiveness analyses were performed according to VAS, CSS, and LCQ scores. Treatment-emergent adverse events were recorded during the study. The primary outcome was the VAS score changes of patients before and after 2 weeks of treatment. The VAS is widely used for the subjective assessment of cough because it is a simple and brief measure of patient-reported outcomes.1718 Participants were asked to indicate cough severity by marking between 0 (no cough) and 100 (the worst cough severity) on a 100 mm scale. Secondary outcomes included between-group differences in effectiveness regarding CSS and LCQ changes. CSS rates daytime and nighttime cough on a 6-point scale from 0 to 5, where 0 indicates no cough and 5 indicates the most severe cough.1316 The LCQ has 19 cough-specific health status questions divided into three domains (physical, psychological, and social) and a 7-point Likert response scale, with a higher score indicating a better health status.1415
To aid clinical interpretability of the patient-reported outcomes, response rates to antitussives were calculated as the proportions of patients exceeding the minimum clinically important difference (MCID) threshold of VAS and LCQ and achieving a 50% improvement from the baseline of total CSS (CSS 50). As proposed by Raj et al.19 and Martin Nguyen et al.,17 the MCID expressed as the total scores of the cough VAS and LCQ in chronic cough were 30 and 1.3, respectively. The time required for the perceived effect on symptom alleviation was also compared between the two groups. We explored differences in treatment-emergent adverse events, defined as adverse events that appeared or worsened after the first dose of the test drug and within 14 days following the last dose. Adherence and satisfaction with the antitussives were also assessed. Given the current level of effectiveness and side effects, patient satisfaction with antitussives was assessed using an 11-point ordinal scale from 0 to 10, with higher scores representing higher satisfaction. A secondary analysis was conducted to determine the possible difference in the effect of codeine on coughing according to the chronic cough phenotype.
Statistical analysis
All analyses were performed using SPSS version 25.0 (IBM Corporation, Armonk, NY, USA), and GraphPad Prism version 5.0 software (GraphPad Prism Software Inc., San Diego, CA, USA) was used for the data analysis and graph generation. Continuous and categorical variables are expressed as mean ± standard deviation (SD) and percentages, respectively. For qualitative and quantitative variables, the χ2 or Fisher’s exact test and Student’s t-test, respectively, were used to compare groups. The Kaplan-Meier method and log-rank test were used to evaluate the time to resolution of symptoms following antitussive treatment. Differences were considered statistically significant at two-sided P values < 0.05.
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board (IRB) of the Gachon University Gil Medical Center (IRB approval No.: GAIRB2019-266). Informed consent was submitted by all participants after a full explanation of the characteristics of the protocol when they were enrolled.
RESULTS
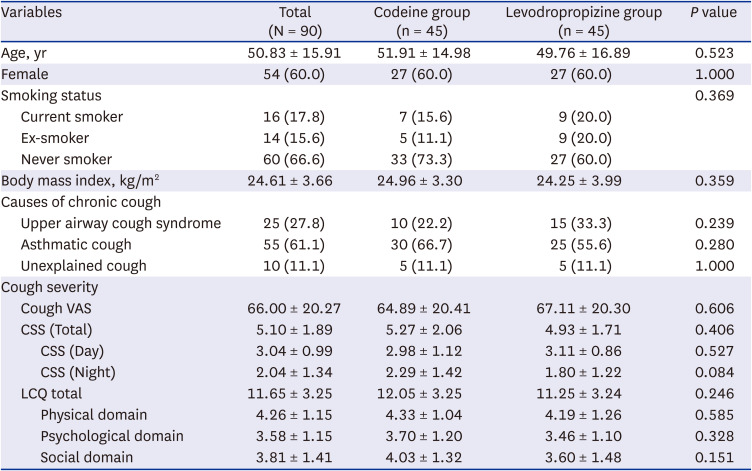
A total of 108 participants were screened; however, 90 participants were enrolled in this study and randomized to either codeine (n = 45) or levodropropizine (n = 45) (Fig. 1). Two participants in the levodropropizine group were lost to follow-up; 88 participants completed the treatment and were included in the analysis. The study participants were aged 50.83 ± 15.91 years and were mostly females (60.0%) and non-smokers (66.6%) (Table 1). The causes of chronic cough included upper airway cough syndrome (n = 25, 27.8%), asthmatic cough (n = 55, 61.1%), and unexplained cough (n = 10, 11.1%). The initial cough severities of VAS, CSS, and LCQ were 66.00 ± 20.27, 5.10 ± 1.89, and 11.65 ± 3.25, respectively. There were no significant differences in demographic characteristics or cough status; therefore, the two groups were comparable.
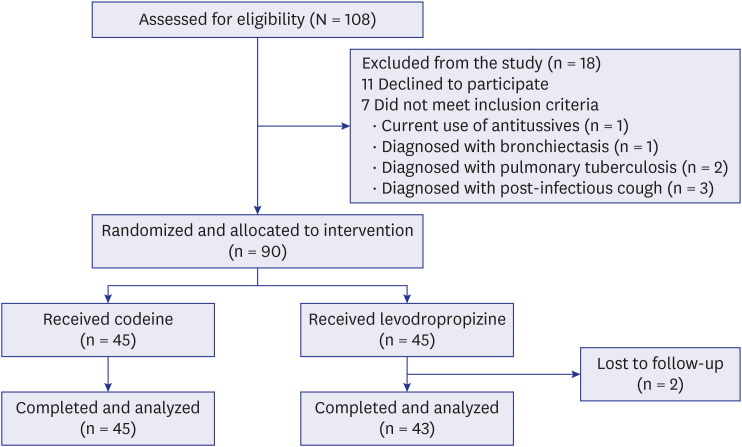
Table 1
Baseline characteristics of the study population in chronic cough
Treatment effectiveness of codeine
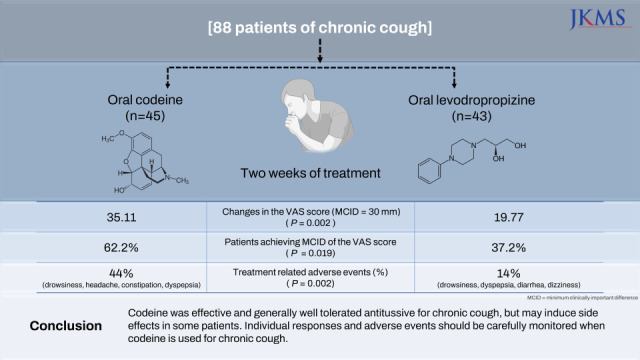
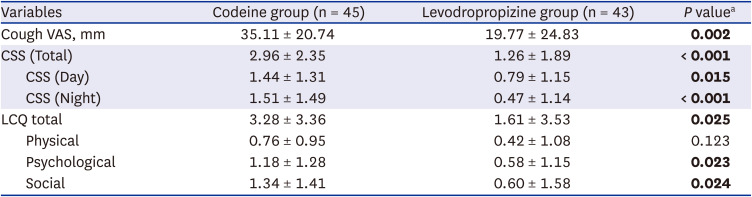
The mean VAS, CSS, and LCQ at baseline in the codeine and levodropropizine groups significantly improved 2 weeks after treatment (Supplementary Table 1). Changes in VAS score were significantly higher in the codeine group than in the levodropropizine group 2 weeks after treatment (35.11 ± 20.74 vs. 19.77 ± 24.83, P = 0.002). Codeine treatment achieved better changes in total CSS (2.96 ± 2.35 vs. 1.26 ± 1.89, P < 0.001), daytime CSS (1.44 ± 1.31 vs. 0.79 ± 1.15, P = 0.015) and nighttime CSS (1.51 ± 1.49 vs. 0.47 ± 1.14, P < 0.001) than levodropropizine treatment. Changes in total LCQ (3.28 ± 3.36 vs. 1.61 ± 3.53, P = 0.025) and domain scores for the psychological and social domain (1.18 ± 1.28 vs. 0.58 ± 1.15, P = 0.023; 1.34 ± 1.41 vs. 0.60 ± 1.58, P = 0.024) were significantly higher in the codeine group than in the levodropropizine group; however, the difference in the physical domain was not significant (Fig. 2, Table 2).
Fig. 2
Effectiveness to chronic cough between codeine and levodropropizine.
The changes in (A) VAS, (B) CSS, and (C) LCQ scores between the two groups are presented as the mean ± standard deviation.
VAS = visual analogue scale, CSS = Cough Symptom Score, LCQ = Leicester Cough Questionnaire.
*P < 0.05 and **P < 0.01.
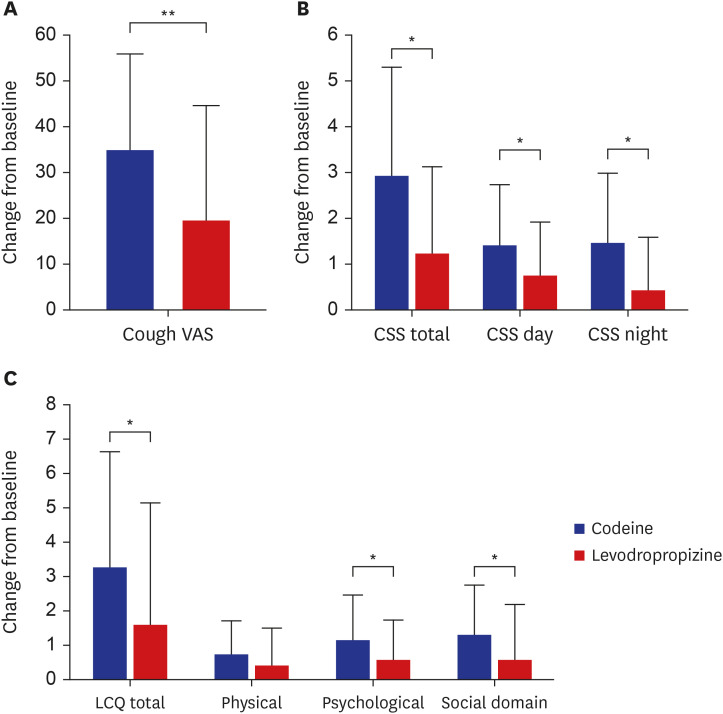
Table 2
Comparison of change in cough severity and quality of life of chronic cough between codeine and levodropropizine
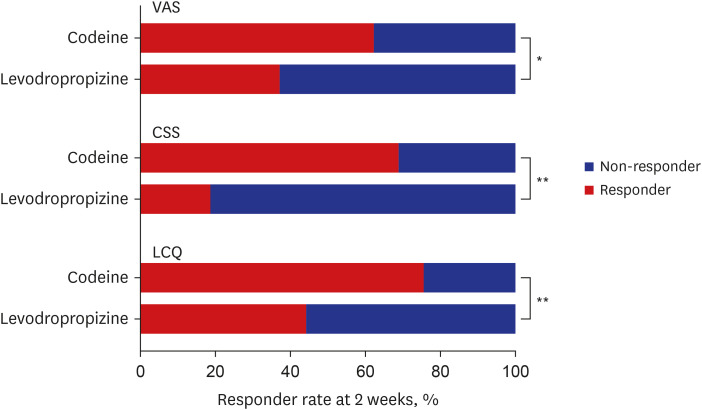
Compared with patients in the levodropropizine group, patients in the codeine group had a significantly higher proportion of responders achieving VAS and LCQ MCID at week 2 (62.2% vs. 37.2%, P = 0.019; 75.6% vs. 44.2%, P = 0.003). Furthermore, 50% CSS improvement was significantly greater in the codeine group than in the levodropropizine group (68.9% vs. 18.6%, P < 0.001) (Fig. 3). Kaplan–Meier curves and log-rank tests showed that, among patients who reached the MCID of VAS, codeine was associated with a significantly shorter time to resolution of chronic cough (Supplementary Fig. 1). The median time to resolution of coughing in the codeine group (median, 3 days, 95% confidence interval [CI], 1.98–4.02 days) was lower than that in the levodropropizine group (median, 7 days; 95% CI, 6.30–7.71 days). The median difference between the two treatment groups was 4 days (P = 0.011, log-rank test). In a subgroup of patients with chronic cough, codeine significantly decreased cough severity and improved the quality of life in patients with upper airway cough syndrome. Patients with asthmatic cough exhibited improved severity and quality of life following codeine administration, although statistical significance was not achieved. In addition, codeine significantly improved changes in the overall LCQ scores and the physical domain of LCQ in patients with unexplained cough (Supplementary Table 2).
Fig. 3
Comparison of response rate to chronic cough between codeine and levodropropizine. Responses rate between the two groups was presented according to the MCID of VAS and LCQ as well as 50% improvement of CSS.
MCID = minimum clinically important difference, VAS = visual analogue scale, CSS = Cough Symptom Score, LCQ = Leicester Cough Questionnaire.
*P < 0.05 and **P < 0.01.
Treatment-emergent adverse events
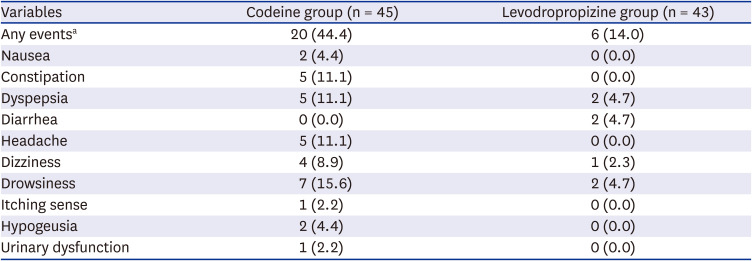
Treatment-emergent adverse events in the codeine group were significantly more frequent than that in the levodropropizine group (44.4% vs. 14.0%, P = 0.002). Of the 20 patients with codeine-related adverse events, 4 discontinued treatment due to adverse events. The most common codeine-related adverse events were drowsiness (15.6%), followed by headache (11.1%), gastrointestinal in nature, specifically constipation (11.1%), and dyspepsia (11.1%) (Table 3).
Table 3
Treatment-related adverse events in patients treated with codeine and levodropropizine
Medication adherence and treatment satisfaction
During the study and at follow-up, 81.8% adhered to the prescribed regimen, and 6.8% used each treatment as needed for cough symptoms. More than 10% of patients discontinued their medication because some (5.5%) recovered from cough symptoms, and others refused their medication due to ineffectiveness (1.1%) or adverse events (4.5%). Additionally, withdrawal due to adverse events was frequent in the codeine group; however, there was no significant difference between the treatment arms. After two weeks of treatment, patients in the codeine group were significantly more satisfied with their treatment than those in the levodropropizine group (Supplementary Table 3).
DISCUSSION
In this study, a 2-week treatment with codeine resulted in a significant improvement in cough severity and cough-related quality of life assessed by the cough VAS, CSS and LCQ, respectively. Codeine treatment also resulted in higher rates of clinically meaningful responses and rapidly reduced cough symptoms compared with levodropropizine. Opiates are cough suppressants that act on the central nervous system; they include morphine and structurally related derivatives, such as codeine.720 Low dose morphine at 5 to 10 mg twice daily was found to significantly suppress chronic refractory cough and was generally well tolerated with limited side effects.21 Furthermore, a trial of low-dose morphine was recommended for adult patients with chronic refractory cough in current ERS guidelines.5 However, given the strict worldwide control and safety risks, including respiratory depression, drowsiness, dependence and abuse, morphine is unfeasibly implemented as an antitussive in Korea and other countries.22 Codeine has been in use since 1834 and widely prescribed in clinical settings for non-productive coughs and pain relief.6 From the first clinical trial of codeine as an antitussive in 1934, early studies have reported success in reducing cough in patients with chronic bronchitis, lung cancer, and pulmonary tuberculosis.69 Furthermore, conversion from codeine to morphine depends on cytochrome P450 family 2 subfamily D member 6 (CYP2D6), which exhibits genetic polymorphism. The CYP2D6 gene polymorphism affects the metabolic behavior of codeine in patients, which may generate inconsistencies in the efficacy of codeine.72023 To date, only one study has compared efficacy and safety between levodropropizine and dihydrocodeine.24 Both antitussives were highly and equally effective in patients with primary or metastatic lung cancer. Side effects were comparable, except for somnolence in the dihydrocodeine group. These results are inconsistent with the findings of this study, and the phenomenon may be explained as follows. Patients with lung parenchymal diseases or structural changes were excluded when the effects of antitussive drugs were compared. We reviewed all treatment-emergent adverse events reported by pharmaceutical companies, while an Italian study assessed the side effects of interest and changes in blood pressure, heart rate, and laboratory tests. The codeine dose used in Korea induced more treatment-emergent adverse events than levodropropizine. Opioid receptors are widely distributed in neuronal and non-neuronal tissues; drowsiness, headache, and digestive problems after administering codeine might be common adverse effects similar to other opiate agonists.25 Although treatment withdrawal due to adverse events was not significantly different between the two groups, adverse events led to the discontinuation of codeine in 20% of patients. However, the discontinuation rate of codeine due to adverse events is still unknown in clinical trials and clinical practice. Our subgroup analyses showed that the benefit of codeine differed according to different patient subgroups. Although the factors, if any, involved in response to antitussives remain unknown, different responses to treatment in patients with specific characteristics require further clarification in larger cohort studies.
Although there are clinical benefits of codeine based on different cough measurement tools, there is an unmet need for novel treatments that favorably impact clinical outcomes in patients who are unresponsive to codeine. Novel antitussives for targeting specific neural pathways in the cough reflex, such as purinergic receptor P2X3 (P2X3), neurokinin-1-receptor (NK1R), and transient receptor potential channels, are being developed and studied in human clinical trials for patients with chronic refractory cough.2627 Promising results of new therapies are expected to benefit the treatment of refractory cough; however, further studies are required to confirm their efficacy in unselected chronic cough, in addition to refractory cough.2628
Patients with chronic cough desperately need effective antitussives that can be used on demand or long-term. Even in patients whose cough is controlled by managing potentially treatable traits, using an antitussive would be useful for breakthrough symptoms. Our study suggests that the timely use of codeine clinically improves cough severity and health-related quality of life without increasing the risk of treatment interruption owing to adverse events. Given the clinical heterogeneity of the chronic cough population, it is critical to perform a thorough initial patient assessment with diagnostic guidelines to accurately identify appropriate patients who will benefit from antitussives.510
This study had certain limitations that must be addressed. First, it relied on subjective self-reported measures and did not evaluate the effectiveness of objective measures of cough, which has contributed to the lack of clarity regarding the nature of antitussive drugs. Second, we could not use intensive objective methods for gastroesophageal reflux disease-related cough, such as 24-hour intraesophageal pH monitoring, manometry, or impedance monitoring, and NAEB, such as induced sputum examination; hence, the cause of chronic cough may be equivocal in such patients. Third, we were unable to obtain placebo pills for codeine or levodropropizine. The placebo effect of codeine has been reported to improve subjective and objective measures, leading some authors to question the efficacy and widespread use of codeine in practice.29 We could not evaluate whether these results encompassed placebo effects or confined effects specific to the purpose or designed intent of the intervention. Fourth, this study addressed the short-term outcomes of codeine. It is unclear whether long-term codeine treatment improves chronic cough with fewer side effects; thus, further study is required. Lastly, data analyses were performed without considering inter-individual variations in cytochrome P450 (CYP) metabolic profiles; confounding factors may have influenced the results. Moreover, evidence for such a dose-response relationship is lacking. Despite these limitations, this study evaluated the effects of codeine on chronic cough, and its results can provide valuable insights into the real-world applications of codeine. Moreover, to ensure a more accurate assessment of the significance of antitussives, we used various criteria, including VAS, CSS, and LCQ measurements, to determine efficacy and performed a collective interpretation.
In conclusion, a 2-week course of codeine was clinically effective in significantly reducing cough severity and improving quality of life. The cough reduction became apparent after 3 days of treatment with codeine. In addition, some patients experienced treatment-related adverse events in the central nervous and gastrointestinal systems. Therefore, patients with chronic cough should be closely monitored for the benefits and adverse effects of codeine.
 XML Download
XML Download