

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Since the coronavirus disease 2019 (COVID-19) was first reported in December 2019, the number of COVID-19 patients has rapidly increased worldwide. Consequently, the World Health Organization declared COVID-19 a global pandemic in March 2020. In Korea, the first patient with COVID-19 was reported on January 20, 2020, and the number of patients proliferated, reaching up to more than 5,000 cases within six weeks from the first case. Despite the activation of infectious disease alerts and obligatory social distancing guidelines from the Korean government, the number of newly confirmed cases remained steady, with more than 1,000 COVID-19 cases per day. However, an increasing weekly COVID-19 occurrence was observed as of November 2021. Subsequently, the cumulative number of confirmed cases reached 457,612, with 3,705 deaths due to easing the strict social distancing guidelines.1
Under the situation of the COVID-19 pandemic, significant concerns for healthcare utilization in cancer treatment were suggested. Since the pandemic is an ongoing global issue, there is a possibility of persistent shortages of medical professionals and healthcare facilities that should be provided to patients with cancer. Therefore, the COVID-19-specific guidelines for cancer treatment were developed.23 The guidelines include the strategy for minimizing infection risk and an individualized approach considering the risks and benefits of active treatment. Nonetheless, the most undesirable consequences from the change of cancer care utilization are later stage diagnosis or shift of cancer stage, as Carlos et al.4 previously suggested. Furthermore, patients with cancer should decide whether to engage in cancer treatment plans despite the fear of infection, which, in turn, precipitated high rates of psychological distress such as depression and anxiety among them.5 Additionally, functional impairment arising from the deterioration of patients’ mental health was associated with disturbances in healthcare utilization and anxiety about the pandemic.5
The rate of psychological distress of patients with cancer was reportedly very high due to the COVID-19 pandemic outbreak.6 In particular, fear of progression (FoP) was directly associated with the level of anxiety regarding the COVID-19, which was elevated in patients with cancer.7 Additionally, FoP was indirectly related to the COVID-19 pandemic; that is, patients were anxious about their disease because cancer treatment plans changed due to the COVID-19 situation.8 During the COVID-19 outbreak, the quality of life of patients with cancer deteriorated with the dilemma of staying at home in minimizing the risk for infection and visiting the hospital for cancer management.9 Depressive symptoms, including fatigue, insomnia, and loss of appetite, were more frequently observed during the COVID-19 pandemic than unaffected periods.10 Notably, FoP was associated with depression11 and anxiety.12
Resilience is the ability of an individual to overcome hardship or stressful trauma and maintain normal physical and psychological functions. Resilience is considered multifactorial: Genetic, developmental, neurobiological, and psychosocial factors are associated with resilience.1314 Although most people are exposed to significant stressors during their lifetime, not all individuals develop psychiatric disorders. The difference in the level of resilience between individuals could explain the vulnerability and maladaptive stress response observed in patients with psychiatric disorders such as depressive disorder and posttraumatic stress disorder. Therefore, understanding the role of resilience in mental health problems helps clinicians evaluate their patients better and predict the development of psychiatric illnesses.
Several patients with cancer experience significant psychological distress—from initial cancer diagnosis through cancer treatment.15 As cancer is a life-threatening disease, it can inflict psychological trauma on an individual. Further, cancer-related distress is associated with a high level of anxiety.16 Although there is a heterogeneity of resilience pathways; including individual differences, appraisal processes, psychosocial support and resources, and coping strategies; appraisal processes and social support were suggested as two common mechanisms.17 More recently, to improve patients’ psychological well-being, interventions that enhance their resilience in cancer treatment have drawn attention. For example, resilience was positively associated with hope and perceived social support among patients with advanced cancer, while it was negatively related to hopelessness, distress, and depression.18
Cancer-related dysfunctional beliefs about sleep (C-DBS) mean unrealistic expectations or perceptual and attention bias, which can play an essential role in perpetuating insomnia.1920 In clinical practice, C-DBS is the primary component to be addressed while conducting cognitive-behavioral treatment for insomnia (CBT-I).21 Dysfunctional beliefs on sleep concepts were associated with anxiety, depression, and sleep disorders in general population as well as patients with cancer during the COVID-19 pandemic.22 Those who have more C-DBS are considered to believe that their sleep disturbance significantly impacts on their immune function or affects disease progression. However, a causal relationship between insomnia and immune functioning in cancer patients should be further investigated with limited evidence.23 Because cognitive restructuring in CBT-I aims to alter common beliefs, worry about undesirable consequences of missed sleep, that is, immune dysfunction or disease progression in cancer patients should be focused on. In this context, we previously observed that viral anxiety was associated with C-DBS in cancer patients during July or August of 2020, when the viral transmission was at its peak.5 Cancer patients still felt anxious about viral infection in 2021, even as the meaning of viral infection faded away. As a result of their impaired immune function, they were concerned about the risk of viral infection, and they felt concerned about the harmful effects of viral infection on their prognosis. It is still important to address their fear of progression in relation to viral anxiety.
This study aimed to explore the clinical symptoms of cancer patients—depression, anxiety, insomnia, pain, or fatigue—that mainly affect their FoP during the COVID-19 pandemic. Additionally, we examined the effect of C-DBS on the association between clinical symptoms and FoP during this pandemic. In this study, we hypothesized that 1) cancer patients’ depression will be positively related to fear of disease progression, 2) their viral anxiety will be positively associated with fear of disease progression, and 3) resilience will at least partially mediate the influence of depression/viral anxiety on cancer patients’ fear of disease progression, and 4) cancer-related dysfunctional beliefs about sleep will at least partially mediate the influence of depression/viral anxiety on cancer patients’ fear of disease progression.
Go to : 
METHODS
Participants and procedure
This study was a retrospective medical records review. Participants included patients with cancer who visited the stress management clinic for cancer patients in ASAN Medical Center for the first time. At the first visit, patients were routinely evaluated for psychiatric history or diagnosis established by clinical interviews with psychiatrists (S.C. and H.K.) who were trained to manage patients with cancer’s psychological problems. Their symptoms were measured using rating scales.
Medical records of patients who visited the clinic between July 1, 2021, and November 31, 2021, were reviewed retrospectively. Furthermore, we selected 231 patients who met the following criteria: 1) self-report questionnaire scores completely available in medical records, and 2) never diagnosed with organic brain disorders or brain metastasis. Additionally, information regarding their age, sex, types of cancer, staging, current treatment modalities, or history of surgical procedures were collected, and rating scales scores were gathered.
Measures
Fear of Progression Questionnaire-Short Form (FoP-Q-SF)
The original version of the FoP-Q was used to measure the FoP in chronically-ill patients24 and applied to cancer patients with recurrence12 and patients with multiple sclerosis.25 While the FoP-Q consists of 43 items with five subscales, the shortened version (FoP-Q-SF), which was developed later, includes 12 items.26 It was previously validated in a group of patients with breast cancer with adequate reliability (Cronbach’s α = 0.87), thereby verifying its validity as an instrument for clinical research. We used the Korean version of the FoP-Q-SF in our study.12
Patient Health Questionnaire-9 items (PHQ-9)
The PHQ-9 is a self-rating scale developed to measure the severity of depression.27 It consists of 9 items rated on a 4-point Likert scale ranging from 0 (not at all) to 3 (nearly every day). A total score of PHQ-9 ranges from 0 to 27, and a high score of PHQ-9 reflects severe levels of depression. We applied the Korean version of PHQ-928 in this study.
Stress and Anxiety to Viral Epidemics-6 items (SAVE-6)
The SAVE-6 scale is a self-report rating scale developed for measuring one’s viral anxiety.29 It consists of 6 items, and each item can be rated on a 5-point Likert scale ranging from 0 (never) to 4 (always). The total score of the SAVE-6 can range from 0–24, and a high score on the SAVE-6 reflects a high level of viral anxiety. We applied the original Korean version of the SAVE-6 scale in this study.
Insomnia Severity Scale (ISI)
The ISI is a self-rating scale for measuring the severity of insomnia.30 It consists of seven questions that assess the severity of insomnia, satisfaction with the current sleep pattern, interference with one’s daily functioning, noticeability of impairment, and the degree of distress or concern. Each item can be rated on a 0–4 Likert scale, and a high level of the total score reflects a severe degree of insomnia. We applied the Korean version of the ISI.31
Connor Davidson Resilience Scale-2 items (CD-RISC2)
The CD-RISC2 is a self-rating scale measuring one’s resilience.34 It was shortened from the original full 25-item CD-RISC. It consists of two items, and each item can be rated on a Likert scale ranging from 0 (not true at all) to 4 (true nearly all of the time). This study applied the Korean version of the CD-RISC2 after receiving permission from the original developer, Dr. Jonathan R. T. Davidson.
C-DBS scale
This is a self-report rating scale developed to measure C-DBS.35 It consists of 2 items regarding dysfunctional beliefs about sleep that patients with cancer may have. For example, “Q1. Immune – My immune system will have serious problems if I do not go to sleep at a certain time” and “Q2. Recurrence – If I do not sleep well at night, my cancer may recur or metastasize.” Two items are rated on a 0–10 scale, and a higher total score reflects a severe degree of dysfunctional beliefs about sleep. This study applied the original C-DBS initially developed in the Korean language.
Statistical analysis
Demographic characteristics and rating scales scores are shown as mean ± standard deviation. The significance level for the analyses was defined as two-tailed at P < 0.05. Pearson’s correlation coefficients were examined among clinical variables. A linear regression analysis with entering methods was conducted to explore variables that predict patients’ FoP. To analyze clinical variables’ mediation effect, whether C-DBS mediates the influence of clinical symptoms on FoP, the bootstrap method with 2,000 resamples was implemented. We used SPSS Windows software version 21.0, AMOS version 27 for Windows (IBM Corp., Armonk, NY, USA), and Jamovi version 1.6.18.0 to perform the statistical analysis.
Ethics statement
The protocol of this study was approved by the Asan Medical Center Institutional Review Board (2021-1754), which waived obtaining informed consent from participants.
Go to :
RESULTS
A total of 231 patients were included in the analysis. The mean age of patients was 54.2 ± 12.8 years, of whom 74.5% (n = 172) were women. Most patients (n = 216, 93.5%) were diagnosed with at least one psychiatric disorder, which included sleep-wake disorders (n = 97, 44.9%), depressive disorders (n = 59, 27.3%), anxiety disorders (n= 23, 10.6%), and others as presented in Table 1. As for the cancer-related variables, 18 patients (n = 7.8%) had a hematologic malignancy, and 24.4% of solid tumors were stage IV. A total of 60 patients (26.0%) had undergone cancer surgery within three months and were currently on either chemotherapy, radiation therapy, hormonal therapy, or target therapy (n = 146, 63.2%). The mean scores of the self-report questionnaires were as follows: the ISI (15.5 ± 6.9), PHQ-9 (11.4 ± 6.6), STAI (40.1 ± 7.1), FoP-Q-SF (36.5 ± 12.2), C-DBS (11.7 ± 6.0), pain (3.6 ± 3.0), fatigue (5.9 ± 2.5), CD-RISC2 (4.7 ± 1.7), and SAVE-6 (11.4 ± 5.6).
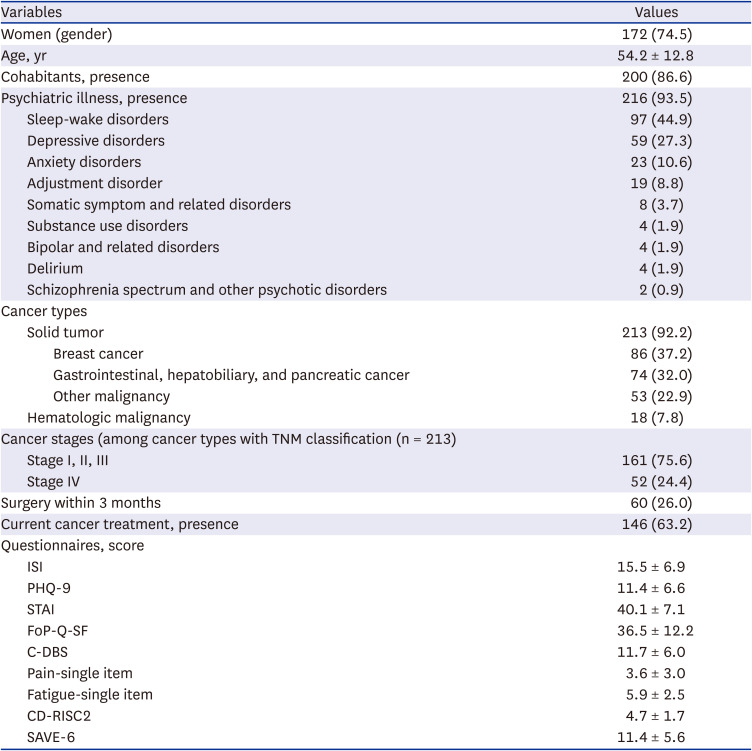
Table 1
Demographic and clinical characteristics of the study subjects (N = 231)
Values are presented as mean ± standard deviation or number (%).
FoP = fear of progression, PHQ-9 = Patient Health Questionnaire-9 items, SAVE-6 = Stress and Anxiety to Viral Epidemics-6 items, ISI = Insomnia Severity Index, CD-RISC2 = Connor Davidson Resilience Scale-2 items, C-DBS = cancer-related dysfunctional beliefs about sleep.
![]()
Table 2 shows Pearson’s correlation analysis results. The FoP score was significantly correlated with PHQ-9 (r = 0.61, P < 0.01), SAVE-6 (r = 0.54, P < 0.01), ISI (r = 0.31, P < 0.01), pain (r = 0.29, P < 0.01), fatigue (r = 0.41, P < 0.01), CD-RISC2 (r = −0.30, P < 0.01), and C-DBS (r = 0.40, P < 0.01). Linear regression analysis, conducted with enter methods, was done to explore the variables which can predict patients’ FoP; it showed that FoP was predicted by age (β = −0.14, P = 0.003), PHQ-9 (β = 0.48, P < 0.001), SAVE-6 (β = 0.34, P < 0.001), and C-DBS (β = 0.15, P = 0.005) (adjusted R2 = 0.55, F = 36.3, P < 0.001; Table 3).


Table 2
Correlation coefficients of each variable in all participants (N = 231)
FoP = fear of progression, PHQ-9 = Patient Health Questionnaire-9 items, SAVE-6 = Stress and Anxiety to Viral Epidemics-6 items, ISI = Insomnia Severity Index, CD-RISC2 = Connor Davidson Resilience Scale-2 items, C-DBS = cancer-related dysfunctional beliefs about sleep.
*P < 0.05, **P < 0.01.
![]()
Table 3
Linear regression analysis to explore the predicting symptoms for fear of disease progression of cancer patients during the COVID-19 pandemic (N =231)
COVID-19 = coronavirus disease 2019, PHQ-9 = Patient Health Questionnaire-9 items, SAVE-6 = Stress and Anxiety to Viral Epidemics-6 items, ISI = Insomnia Severity Index, CD-RISC2 = Connor Davidson Resilience Scale-2 items, C-DBS = cancer-related dysfunctional beliefs about sleep.
![]()
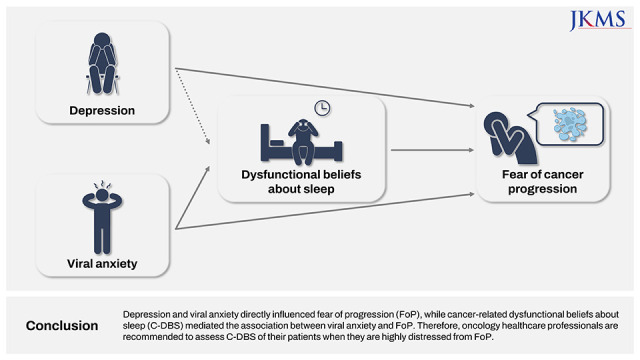
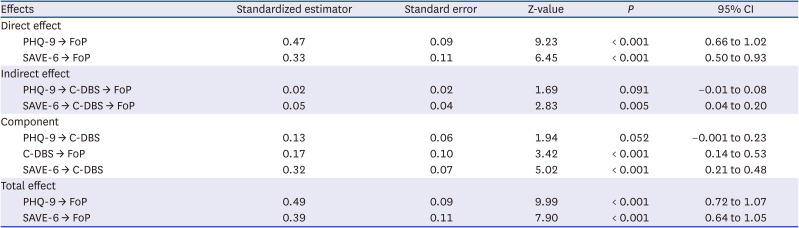
A mediation analysis showed that the viral anxiety of cancer patients directly influenced their FoP, and cancer-related dysfunctional beliefs about sleep mediated this association (Table 4, Fig. 1). Depression directly influenced patients with cancer’s FoP, but dysfunctional beliefs about sleep did not mediate this association.
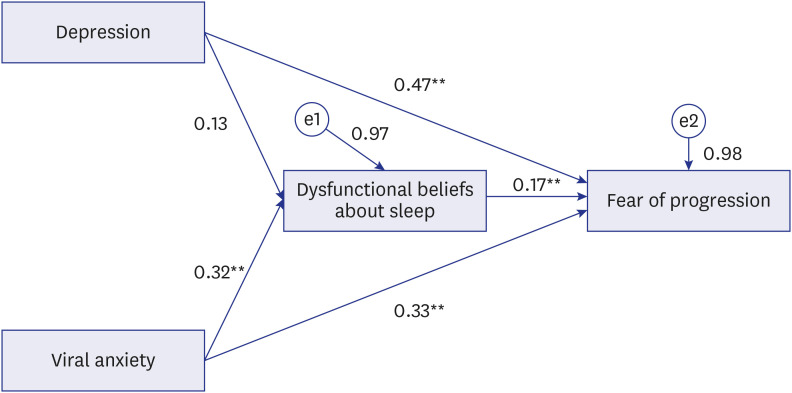 | Fig. 1Mediation model showing the pathway from the effect of depression or viral anxiety (independent variables) on the fear of disease progression (outcome) through resilience or cancer-related dysfunctional beliefs about sleep (mediator).
|
Table 4
The results of direct, indirect, and total effects on mediation analysis
CI = confidence interval, PHQ-9 = Patient Health Questionnaire-9 items, SAVE-6 = Stress and Anxiety to Viral Epidemics-6 items, C-DBS = cancer-related dysfunctional beliefs about sleep.
![]()
Go to :
DISCUSSION
The regression model observed that the FoP of patients with cancer during the COVID-19 pandemic was associated with age, depression, viral anxiety, and C-DBS. The viral anxiety of cancer patients directly influenced their FoP, and C-DBS mediated this association. Depression directly influenced cancer patients’ FoP, but dysfunctional beliefs about sleep did not mediate this association. Clinicians involved in cancer treatment should focus on FoP because it is closely related to physical or psychological distress and the patient’s quality of life. FoP in patients with cancer is one of the most commonly reported yet most neglected psychological distress.36 In recent years, the term “fear of cancer recurrence,” covering both recurred and metastatic cancer, has obtained its popularity and relevant clinical attention in the same context.36 FoP with clinical significance includes specific characteristics, such as a high level of distress, maladaptive adjustment, and marked impairment in daily function and future planning.37
As mentioned above, the COVID-19 pandemic impacts cancer patients negatively. As expected, socio-demographic, physical, and psychological factors were associated with FoP in the COVID-19 pandemic according to the most recent review of clinical research.38 Furthermore, those with a higher level of FoP were more frequently observed during the COVID-19 period than pre-COVID-19. Specifically, cancer patients are even more vulnerable to distress during the pandemic, thus requiring more delicate psycho-oncological care.
Preceding research found socio-demographic, physical, and psychological risk factors associated with the FoP in cancer patients. Therefore, our study included a wide range of those risk factors in the correlational analysis. As for the socio-demographic variables, younger age was significantly associated with FoP, per previous studies.39 As for the physical risk factors, pain and fatigue were positively related to the level of FoP, which were also in line with previous results.4041 Conversely, depression,4243 anxiety,43 and sleep disturbance44 were consistently associated with FoP in other studies, which were relevant to our results. Moreover, as suggested before, resilience was negatively associated with FoP.45
This study observed that viral anxiety directly influenced cancer patients’ FoP, and C-DBS mediated this association. Patients with cancer experiencing sleep disturbance may fear disease progression or recurrence of cancer.40 Previously, we reported that patients’ C-DBS were associated with their psychological distress. Patients’ worry about the harmful effects of sleep disturbance on their immune system was significantly correlated with insomnia severity and FoP. We also reported that C-DBS mediate the influence of FoP on their insomnia.46 Sleep deprivation—reportedly—disrupts immune function and promotes the progression of cancer.45 Based on medical knowledge, patients worry that their sleep problems might be linked with disease progression. Therefore, these beliefs are “dysfunctional,” causing anxiety in patients with cancer and resultantly stimulating sleep problems.47
During the COVID-19 pandemic, patients with cancer easily get viral anxiety (i.e., fear of being infected with coronavirus). As a high-risk group, they have high levels of anxiety about being infected.48 Their fears may be related to their awareness that impaired immune systems of cancer patients are weak in preventing viral infection; a dilemma is thus created: the necessity of life-saving cancer treatments versus exposing oneself to the risk of infection. Contrastingly, the viral anxiety of patients with cancer may help reduce the risk of being infected by others by adhering to a safety behavior.7 However, excessive viral anxiety exaggerates protective attitudes leading to delayed cancer treatment and poor compliance.49 Their viral anxiety was related to their insomnia severity and C-DBS. The COVID-19 pandemic affected individuals’ sleep problems and even cancer patients’.50 Patients with cancer with sleep problems related to viral anxiety might fear cancer progression and thus aggravate their sleep problem, perpetuating a vicious cycle. They were concerned about the risk of viral infection due to their impaired immune function, and about the harmful effects of viral infection on their prognosis. In this pandemic era, the fear of progression in relation to viral anxiety still needs to be addressed when examining psychological distress in cancer patients.
Results showed no mediation effect of C-DBS on the association between depression and FoP. However, the statistical significance was marginal (P = 0.052), and further clinical research is required to investigate the mediation effect of dysfunctional sleep beliefs. In a previous study, we explored the association between depression, FoP, and C-DBS, suggesting that C-DBS were significantly correlated with depression and FoP.51
Although we hypothesized that resilience would mediate the association between FoP and depression or viral anxiety, we could not observe significant mediating effect of resilience of patients with cancer. This finding is concordant with a previous study in that even in highly distressed cancer patients, resilience level was not significantly different when compared to those without cancer.52 On the other hand, breast cancer survivors experienced less FoP when they had a higher level of resilience, despite limited access to healthcare system during the COVID-19 pandemic.53 This discrepancy could occur because of the heterogeneity of clinical samples as well as difference in methodology for evaluating psychological resilience. Because the CD-RISC2 is a brief version originated from the full CD-RISC, our results would be different when the full version or other measurement tools were applied. Of note, more complex version of the CD-RISC showed more favorable psychometric properties in another study.54
The strength of our study is that we applied the SAVE-6 scale to patients with cancer, a viral anxiety-specific rating scale,29 rather than other scales for measuring general anxiety symptoms. Additionally, it was previously validated in patients with cancer55 and is therefore an appropriate tool for our study. Thus, during the COVID-19 pandemic, the viral anxiety of patients with cancer must be adequately assessed because viral anxiety—as indicated by our results—is associated with their psychological distress.
Several limitations should be considered. First, study participants were recruited from a clinically heterogeneous sample who visited the psycho-oncology clinic at a tertiary hospital. Almost all patients had at least one psychiatric disorder, of which sleep-wake disorders and depressive disorders accounted for most. Therefore, there is a possibility of selection bias, limiting the generalizability of our results. Second, clinical and psychological evaluations were based on self-report scales. However, clinical information was thoroughly reviewed, and two qualified psycho-oncologists made psychiatric diagnoses to overcome the limitations of the scales. Third, some risk factors associated with FoP were not included in the analysis. For example, socioeconomic status,56 spiritual well-being,53 quality of life,44 or other coping strategies57 were not covered. Nonetheless, a variety of risk factors, including socio-demographic, physical, and psychological variables, were investigated in our study.
During the COVID-19 pandemic, the FoP of patients with cancer was associated with younger age, depression, viral anxiety, and C-DBS. Depression and viral anxiety directly influenced FoP, while C-DBS mediated the association between viral anxiety and FoP. Therefore, oncology healthcare professionals are recommended to assess C-DBS of their patients when they are highly distressed from FoP.
Go to :
 XML Download
XML Download