

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
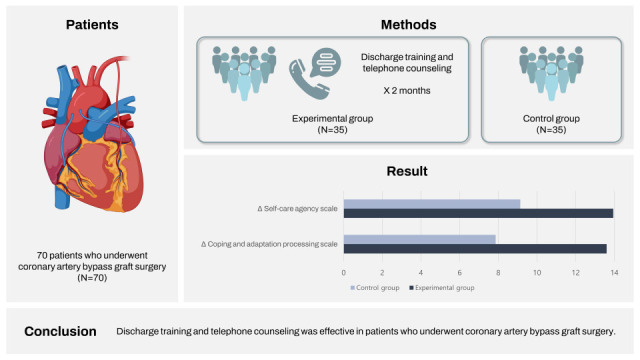
Coronary artery bypass graft (CABG) surgery is the process of creating a bridge (grafting) to narrowed or clogged coronary arteries using artery and/or vein grafts. Although the success rates of CABG surgeries have increased, patients may encounter problems and/or complications in the hospital before discharge or at home after discharge.123 These problems and complications even increase with inadequate discharge planning and training.45 Discharge planning ensures the determination of home care needs, continuity of care, and improvement of the quality of care.678
Self-care, coping, and adaptation remain important in promoting health. Self-care is defined as the decisions and practices made by individuals, who face health concerns, to cope with these concerns, improve their health, and enhance their adaptation. With these improved decisions and practice skills, patients can protect their health more actively.910 Today, with the increase in the technology use, patient counseling by telephone can be provided for patient follow-up at home, monitoring drug side effects, counseling, sudden situations, appointment reminders, evaluation of the effectiveness of discharge training, determining training needs, performance evaluation, providing communication between hospital and home, increasing participation in training, improving self-care, increasing quality of life, and ensuring coping and adaptation.11
This study was conducted to determine the effect of discharge training planned according to Self-Care Deficit Theory and telephone counseling on self-care agency and coping and adaptation process in patients undergoing CABG surgery.
Go to : 
METHODS
Population
The population of the research consisted of patients who were hospitalized in the cardiovascular surgery unit of a state hospital in Cyprus and underwent CABG surgery and the sample consisted of patients who underwent CABG surgery between September 2020 and May 2021. The sample size was determined by G*power analysis. The statistical power of the study was planned to be 80% and it was calculated that there should be at least 35 (experimental group = 35, control group = 35) individuals in both groups with a confidence interval (CI) of 95% and a xlink:type two error of 5%.
In the study, the groups were distributed through block randomization. The website, randomizer.org, was used for the randomization process. Primarily, combinations were created. The number of participants (70) was divided by the number of combinations and the combinations were sorted by group (18 groups in total). Group A and group B were determined as the experimental (B) and control (A) groups by drawing lots.
Local
The study was carried out in a state hospital and in a cardiovascular clinic, located in Nicosia city of the country of Cyprus.
Selection criteria
Selection criteria were: having undergone CABG surgery, being able to speak, ability to read and write in Turkish, not having a visual, hearing, physical, or mentally disability, and being over age 18.
Data collection
Patient descriptive characteristics form
The form consists of 44 questions and two parts. The first part includes 20 questions about the sociodemographic characteristics of the patients (age, gender, marital status, number of children, education level, employment status, smoking-alcohol use, social security, income status, caregivers, need for help/care). The second part consists of 24 questions about the medical condition/CABG surgery of the patient (presence of chronic disease, having a heart attack, surgery xlink:type, number of vessels changed, status of receiving training, information sources, sufficiency of information, anxiety, ongoing or finished problems, medical topics to want to know).
Exercise of Self-Care Agency Scale (ESCA)
The scale was developed by Kearney and Fleicher in 1979 and is originally a 43-item English form. Its Turkish validity and reliability study was conducted by Nahcivan in 1993 and the form was modified to 35 items. The five-point Likert-type questionnaire aims to determine the ability of individuals to care for themselves and their self-care agency. The scale consists of statements scored from 0 to 4. It consists of a scale of ‘very uncharacteristic of me’ (0), ‘somewhat uncharacteristic of me’ (1), ‘uncertain’ (2), ‘somewhat characteristic of me’ (3), and ‘very characteristic of me’ (4) in each statement. Eight negative statements on the scale (3, 6, 9, 13, 19, 22, 26, and 31) are scored reversely. The lowest score obtainable from the scale is 35 and the highest score is 140. A score of 24–64 points on the scale indicates ‘poor’ self-care agency; a score of 65–100 indicates ‘moderate’ self-care agency; a score of 101–112 indicates ‘good’ self-care agency and a score of 113–140 indicates ‘very good’ self-care agency. The scale has no cut-off value. It is the most used scale for the concept of self-care, can be applied in a short time like 8–10 minutes, and is understandable.12
Coping and Adaptation Processing Scale (CAPS)
The scale was developed by Callista Roy in 2004. Its Turkish validity and reliability study was performed by Çatal in 2015. It is theoretically based on the Roy Adaptation Model and concepts related to its cognitive process. The scale consists of subscales such as troubleshooting and focusing, physical and conclusion, attention process, systematizing process, learning and establishing relationship. The number of items in the subdimensions is as follows: ‘troubleshooting and focusing’ involves 10 items; ‘physical and conclusion’ involves 14 items: ‘attention process’ involves 9 items; ‘systematizing process’ involves 6 items; ‘learning and establishing relationship’ involves 8 items. Items are scored on a Likert-type scale: ‘never,’ ‘rarely,’ ‘sometimes,’ and ‘always.’ ‘Never’ is scored 1 point; ‘rarely’ is scored 2; ‘sometimes’ is scored 3 and ‘always’ is scored 4. A minimum of 47 and a maximum of 188 points can be obtained from the 47-item scale. In the original scale, the Cronbach alpha reliability coefficient is 0.94 for the total scale and ranges between 0.78–0.86 for the subscales. The coefficient for the Turkish validity and reliability study is 0.82. Reverse scoring is obtained by summing the numerical answers of each subscale. Items of the physical and conclusion subdimension are reversed, re-scored, and calculated. Reverse scored items are the items 5, 8, 13, 15, 20, 23, 24, 29, 33, 35, 39, 43, 45, and 47. Reverse scoring is as 1 = 4, 2 = 3 or 3 = 2, 4 = 1.13
Data analysis/treatment
The sealed envelope method was applied with combinations determined according to block randomization and the patients were included in the experimental or control group on the day of the intervention (Fig. 1).
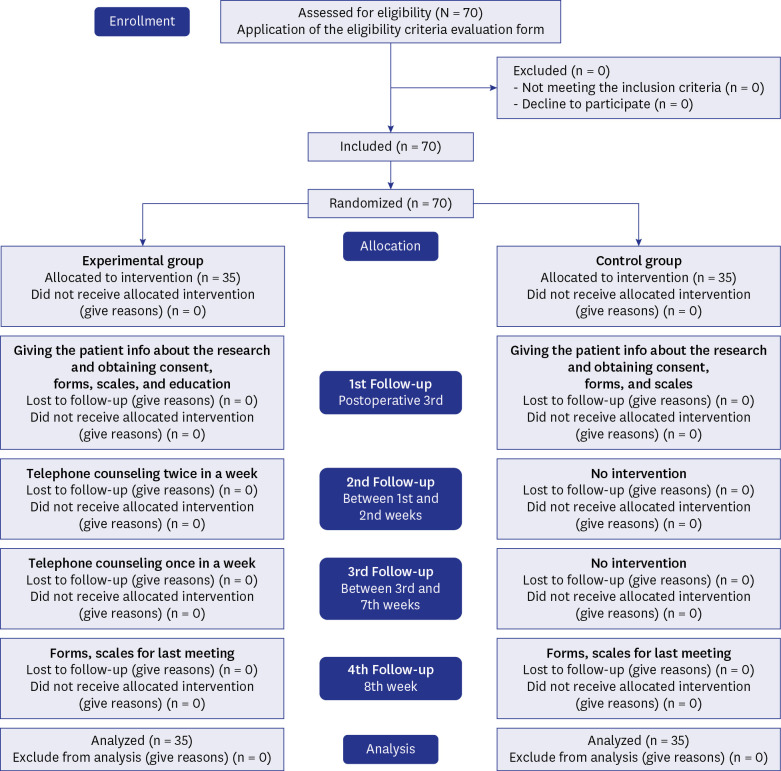
In the first interview, the patients in the experimental and control groups were met at the first interview and informed about the research. The Patient Descriptive Characteristics Form, ESCA, and CAPS were applied to the patients who voluntarily agreed to participate in the study (including both groups). The researcher provided discharge training to the patients in the experimental group in the clinic with the illustrated discharge training guideline prepared according to Orem’s Self-Care Deficit Theory. The training took 25–30 minutes on average. During the training, patients were allowed to ask questions to better understand the subject and these questions were answered by the researcher. After the training, a copy of the discharge training guideline was given to the patients in the experimental group.
The patients included in the experimental group were called twice a week for the first two weeks after discharge and counseling was provided. The problems experienced by the patients during telephone counseling and the suggestions for these problems were recorded in the ‘Telephone Counseling Patient Follow-up Form.’ The control group received no intervention for the first two weeks.
The patients in the experimental group were called once a week by telephone between the third and eighth weeks and counseling was provided. During these weeks, the problems experienced by the patients and the suggestions for these problems were recorded in the ‘Telephone Counseling Patient Follow-up Form.’ The control group received no intervention within the specified weeks.
Face-to-face interviews were conducted with the experimental and control groups at the hospital at the end of two months. In this interview, ESCA and CAPS were applied for the last time. Afterward, a copy of the discharge training guideline was given to the patients in the control group.
The Statistical Package for Social Sciences (SPSS) program (SPSS, Chicago, IL, USA) was used for statistical analysis. Percentages and frequencies were determined for the analysis of descriptive statistics. The χ2 test was applied to determine the variables in the categories. The Kolmogorov-Smirnov test was used to test the normal distribution of the data. The Mann-Whitney U test was used for bivariate data without normal distribution and the Kruskal-Wallis H test was used for the data with three or more variables. The independent samples t-test was utilized for normally distributed bivariate data. Independent sample t-test and Mann-Whitney U test were used for intergroup comparisons. The data were evaluated at a CI of 95% and a P value of P < 0.05.
Ethics statement
For the study, permissions were obtained from the Ethics Committee of Dr. Burhan Nalbantoğlu State Hospital for this research (YTK.1.01 [EK015/20]). Additionally, patients who were included in the study provided written permission and the researchers verified the validity and reliability of the scales used in the research.
Go to :
RESULTS
Table 1 shows the introductory characteristics of the patients. In the experimental group, 60–69 years old (37.1%), male (68.6%), married (85.7%), having two children (51.4%) and high school graduate degree (60.0%) patients made up the majority. In the control group, those aged between 50–59 and 60–69 (both of them 28.6%), male (60.0%), married (91.4%), having three or more children (45.7%) and high school graduates (65.7%) made up the majority.
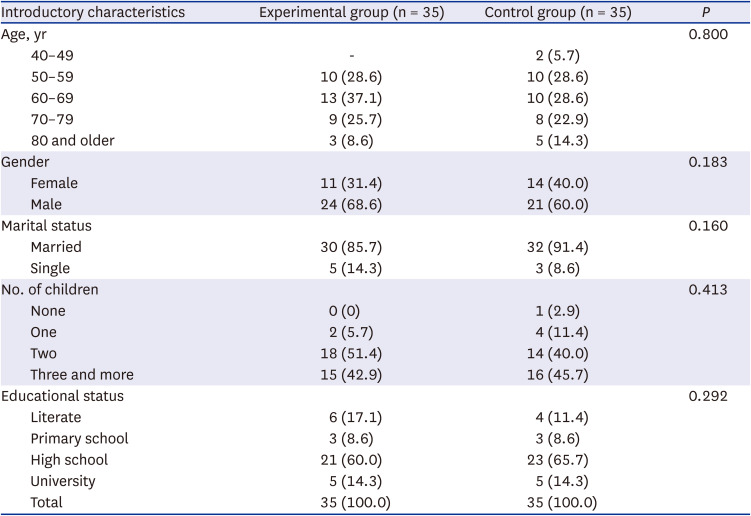
Table 1
Introductory characteristics of the patients
![]()
Table 2 shows the descriptive characteristics of the patients and their average scores from the coping and adaptation process scale. In the experimental group, patients aged 70–79 (difference 17.6), male (difference 13.9), married (difference 14.4), having three or more children (difference 15.7), having literate educational degree (difference 15) groups’ average score increased more. In the control group, patients aged 50–59 (difference 10.4), male (difference 8.53), married (difference 8.16), having one and three or more children (difference 7.75), primary school educational degree (difference 11.6) groups’ average score increased more. When compared to the experimental group, it is seen that the scores of the control group increased less. Statistical significance was determined between the mean score after training and counseling in the experimental group and gender (P = 0.001), marital status (P = 0.004), number of children (P = 0.045). Statistical significance was determined between the mean score after training and counseling in the experimental group and marital status (P = 0.038).
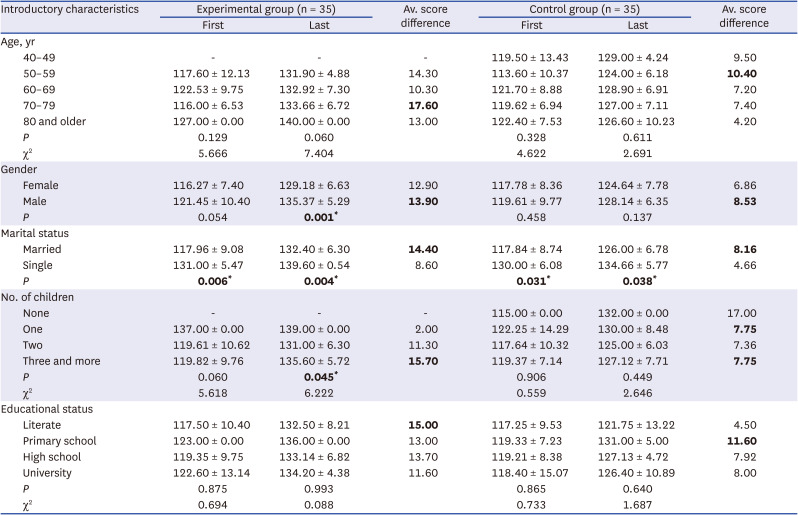
Table 2
Comparison of patients’ Coping and Adaptation Processing Scale mean scores with introductory characteristics
Values are presented as Av. ± SD. χ2 used Kruskal-Wallis H test.
Av. = average, SD = standard deviation.
*P < 0.05.
The values given as 'bold' (av. score difference) are the group in which the difference is seen the most between before and after training-counselling. ‘Bold’ values with * indicate the P significance value.
![]()
Table 3 shows the descriptive characteristics of the patients and their average scores from the self-care power scale. In the experimental group, patients aged 70–79 (difference 17.67), female (difference 14.73), single (difference 15.4), having three or more children (difference 16.6), having primary school educational degree (difference 19) groups’ average score increased more. In the control group, patients aged 50–59 (difference 10.5), male (difference 9.9), single (difference 11), not having and having one child (difference 14), having university educational degree (difference 15.8) groups’ average score increased more. When compared to the experimental group, it is seen that the scores of the control group increased less. Statistical significance was determined between the mean score after training and counseling in the experimental group and gender (P = 0.010). Statistical significance was determined between the mean score after training and counseling in the experimental group and gender (P = 0.041).
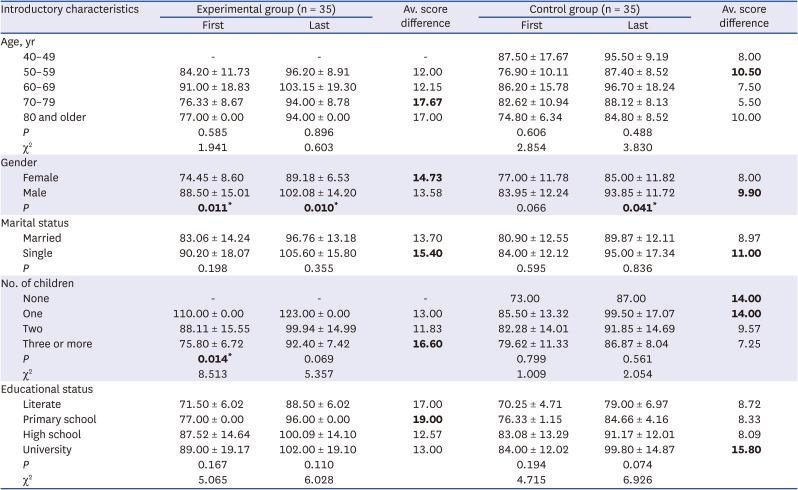
Table 3
Comparison of the self-care power scale mean scores of the patients with the introductory characteristics
Values are presented as Av. ± SD. χ2 used Kruskal-Wallis H test.
Av. = average, SD = standard deviation.
*P < 0.05.
The values given as 'bold' (av. score difference) are the group in which the difference is seen the most between before and after training-counselling. ‘Bold’ values with * indicate the P significance value.
![]()
Table 4 shows the CAPS and ESCA scores of the patients before and after the discharge training and telephone counseling services. The mean CAPS score of the patients in the experimental group was 119.82 ± 9.76 before the training and counseling services and 133.42 ± 6.35 after the services. The score of the patients in the experimental group increased by 13.6. The initial mean score of the patients in the control group was 118.88 ± 9.15 and the final mean score was 126.74 ± 7.06. The score of the patients in the control group increased by 7.86 points. During the coping and adaptation process, the scores of the experimental and control groups were significant and the difference found in the intergroup comparison was statistically significant (pre- and post-period, P = 0.010, 0.001, respectively). In the comparison of ESCA, before and after training/counseling, statistical significance was determined in both groups (P = 0.019, 0.001, respectively).
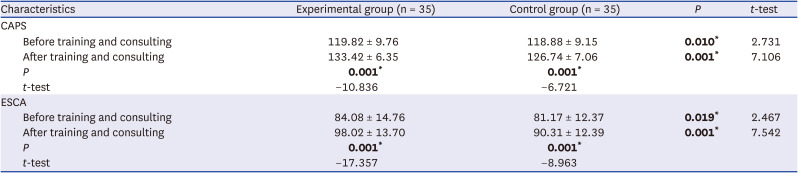
Table 4
CAPS and ESCA score distribution
Values are presented as average ± standard deviation.
CAPS = Coping and Adaptation Processing Scale, ESCA = Exercise of Self-Care Agency Scale.
*P < 0.05.
‘Bold’ values with * indicate the P significance value.
![]()
Table 4 also presents the ESCA scores of the patients. The mean score of the patients in the experimental group was 84.08 ± 14.76 before training and counseling and 98.02 ± 13.70 after training and counseling; the score increased by 13.94. The mean score of the patients in the control group was 81.17 ± 12.37 at the first interview and 90.31 ± 12.39 at the final interview.
The score of the control group increased by 9.14. Table 5 shows the statistical significance determined between both scales and the experimental and control groups (P = 0.001).

Table 5
Effect size of CAPS and ESCA after training and counseling
| Characteristics | Experimental group | Control group | Effect size | Z | P |
|---|---|---|---|---|---|
| CAPS | 13.6 | 7.86 | 5.74 | −5.055 | 0.001* |
| ESCA | 13.94 | 9.14 | 4.80 | −5.220 | 0.001* |
CAPS = Coping and Adaptation Processing Scale, ESCA = Exercise of Self-Care Agency Scale.
*P < 0.05.
‘Bold’ values with * indicate the P significance value.
![]()
Go to :
DISCUSSION
Discharge training is a process that starts from the moment the patient is hospitalized and prepares the patient to continue self-care at home in better quality. With training, recovery processes are accelerated, self-care skills are improved, and coping and adaptation processes progress positively.814 Especially after major surgeries such as CABG, patients and their relatives may need training on the quality of life, problems that may occur at home, and care. Because it is known that without patient training and counseling services, the rate of problems that can develop at home increases.5
After the patients are discharged, patients may develop anxiety on issues such as care and quality of life. In our study, it was determined that the problems that the patients experienced at home more were pain, inactivity, use of compression socks, sore throat, and a sense of itchiness. Telephone counseling is recommended to better pursue the process that starts after discharge.4
In our study, discharge training and telephone counseling services were provided to the patients. The mean ESCA and CAPS scores of the patients in the experimental group increased more compared to the control group. Many studies examining the effect of training and patient counseling services given to patients undergoing CABG surgery are available in the literature.
In one of the studies, telephone counseling was provided to patients who had undergone CABG surgery to assess their quality of life. As a result of the study, it was determined that the quality of life of the experimental group who received telephone counseling service was statistically higher than that of the control group.4 The study that provided discharge training and counseling services to patients who had undergone CABG surgery found that the quality of life of the patients included in the experimental group was higher than that of the control group.1
With good and accurate training given to the patients, the medical condition can be understood more easily; disease management can be better performed; information can be provided about the problems that may develop and the interventions that can be applied. As a result, the duration of hospital stays will be shortened; patient satisfaction will increase; and health expenditures will be reduced.151617 In the study that provided training to patients after myocardial infarction, the effect of training on self-care agency was evaluated. According to this, the self-care agency of the patients included in the experimental group increased by 40 points after the training whereas the patients in the control group remained at a moderate level before and after the training.18 In one study, researchers provided training to evaluate the quality of life of patients and found that the quality of life of the patients in the experimental group was higher than that of the control group at the end of the one-month period.19
Self-care can be defined as the decisions and actions made by the patient, who is alone with his/her health problems, in order to cope with these concerns, adapt, and recover.92021 A patient with a high self-care agency and a comfortable coping and adaptation process will be able to better control his/her health. It is necessary to guide the patient, who will do his/her part more comfortably about his/her health, provide discharge training and telephone counseling as a nurse, ensure his/her recovery, and support.10
It is known that the profession of nursing is a scientific and artistic health discipline. It helps everyone, regardless of whether they are sick or healthy. Orem, who developed the self-care model, and Roy, the first name that comes to mind regarding the Adaptation Model, recommend helping people and using scientific knowledge in integrity while helping.13
Orem’s theory is used in patient education and counseling because it focuses on individuality and provides a systematic nursing guide to assess the patient's needs, limitations, health perception, capacity, and care behaviors. After CABG surgeries, it is of great importance to increase the self-care of people through education and counseling, to reduce and eliminate the difficulties they experience, to complete or correct the missing or wrong ones, to develop and reinforce existing positive behaviors and practice.2223
It is important for patients who have undergone CABG surgery to strengthen their self-care, coping, and adaptation in order to solve the problems related to the surgery and to control the symptoms. In order to strengthen self-care and increase coping and adaptation, the patient should initiate and maintain activities by themselves. However, all these activities that are initiated depend on the strength and abilities of the patients. For this reason, the use of ESCA and CAPS scales can be considered to determine these strengths and abilities. Thanks to the use of these scales in the clinical setting, active participation of patients in their own treatment and care can be ensured, and coping and adaptation processes with their self-care powers can be determined easily. In fact, it can even be corrected by focusing on the issues that patients lack knowledge.2425
There are some limitations in our study. This study was conducted as randomized, controlled and experimental. Such a study (discharge training and telephone counseling) for patients who have undergone CABG surgery has been implemented for the first time in the country. We conducted our study in a single center.
In our study, discharge training and telephone counseling were provided to the patients in the experimental group. After the two-month follow-up period, the mean ESCA and CAPS scores of the patients in the experimental group increased more compared to the control group. Discharge training and telephone counseling accelerate the recovery of patients while they are in the hospital and after they are discharged and reduce problems that may develop. It is recommended that providing discharge training and telephone counseling to patients undergoing surgery will be beneficial.
Go to :
 XML Download
XML Download