

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Coronavirus disease 2019 (COVID-19) is an infectious disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).1 First identified in the city of Wuhan, Hubei, China in late December 2019, the World Health Organization (WHO) declared a pandemic on March 11, 2020.2 Globally, as of October 7, 2021, there have been 236,132,02 confirmed cases of COVID-19, including 4,822,272 deaths, reported to the WHO.3 As of October 7, 2021, there have been 325,804 confirmed cases and 2,544 deaths in Korea.4
The prevalence of COVID-19 in children and adolescents is low, and most of them only have mild symptoms or are asymptomatic.56 However, secondary problems caused by COVID-19 may appear, and several recent studies on mental health have been published. A study reported 11.78% with depression, 18.92% with anxiety, and 6.56% with depression and anxiety in 1,036 quarantined adolescents in China.7 Zhou et al.8 evaluated adolescents in China ages 12–18 years old, of which 37.4% and 43.7% of cases had anxiety and depression symptoms, respectively, in a cross-sectional study using an online survey. Children and adolescents experienced significantly lower HRQoL (40.2% vs. 15.3%), more mental health problems (17.8% vs. 9.9%) and higher anxiety levels (24.1% vs. 14.9%) than before the COVID-19 pandemic in Germany.9 And students in Daegu, Republic of Korea also experienced lots of mental difficulties since the COVID-19 pandemic.10
The COVID-19 recession that began in February 2020 was the worst global financial crisis since the Great Depression.11 Korea did not implement any lockdowns but implemented a social distancing policy, according to the quarantine stage, as employment and economic status declined.12 Recession has significantly increased the frequency of mental health problems in Spain, the US, and South Korea.131415 Family socioeconomic status is known to cause mental health problems in adolescence.1617
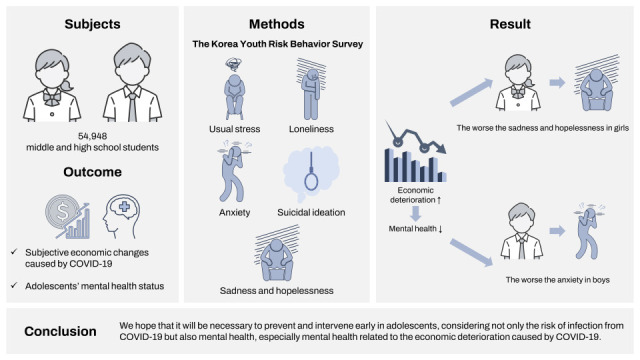
Therefore, we would like to evaluate the subjective economic changes caused by COVID-19 in Korea and adolescents’ mental health status.
Go to : 
METHODS
Source of data
These data are from the Korea Youth Risk Behavior Survey published by the Korea Center for Disease Control and Prevention in South Korea, which is a cross-sectional national representative survey of middle and high school students every year.18 The survey was a stratified, clustered, multistage probability sampling conducted from August 3, 2020, to November 13, 2020. The survey is conducted annually through an anonymous, self-administered web-based online survey targeting 400 middle and high schools nationwide, which includes about 60,000 middle and high school students. In each school sampled, one class was sampled for each grade, and an online survey was conducted in the school computer room for all classes. In the 2020 survey that we used, 54,948 out of 57,925 subjects participated, showing a participation rate of 94.9%.
Variables
We used five factors to assess mental health in adolescents. Usual stress is based on a five-point Likert-scale response to the questionnaire, “How much stress do you usually feel?,” with response options “do not feel any,” “not much,” “some,” “high,” and “very high.” When performing an odds ratio analysis with a logistic regression analysis, the first three were normal and the other two were stressful. Loneliness is based on the survey question, “How often have you felt lonely in the past 12 months?” with responses being “never,” “hardly ever,” “sometimes,” “often,” and “always.” When performing an odds ratio analysis with a logistic regression analysis, the first three were normal and the other two were loneliness. Anxiety uses generalized anxiety 7.19 It was divided into seven questions on a scale of 0–3 points, and four groups were divided into normal, mild, moderate, and severe. When performing an odds ratio analysis with a logistic regression analysis, the normal and mild were classified as normal, and moderate and severe were classified as having anxiety. Sadness and hopelessness are based on a yes/no response to the survey question, “In the past 12 months, have you felt so sad or hopeless that you stopped your daily activities for two weeks?” Suicidal ideation is a dichotomous measure according to the question, “Have you seriously considered committing suicide in the past 12 months?” with yes or no response.
Subjective economic deterioration caused by COVID-19 is based on the questionnaire, “Do you think the economic status of student families has become more difficult than before due to COVID-19?” with possible responses being “Very much,” “Some,” “Not much,” and “Not at all.” Three additional variables were used as covariates in regression analysis. Participants were middle and high school students and usually between the ages of 13 and 18. Academic performance and economic status were divided into five levels, “high,” “upper-middle,” “middle,” “lower-middle,” and “low.”
Data analysis
Statistical analyses were performed with consideration of the complex sampling design using SPSS Statistic 26.0 (IBM Corp., Armonk, NY, USA), with P < 0.05 as the level of statistical significance. The χ2 test was used to compare the general characteristics and mental health factors between men and women. In addition, to analyze the mental health factors according to changes in economic conditions caused by COVID-19, the χ2 test was used. Logistic regression analysis was used to analyze the odds ratio of mental health factors due to economic changes caused by COVID-19. Since the statistical analysis was converted to a composite sample, the number of analysis subjects, fraction, and sampling error were expressed.
Go to :
RESULTS
The demographic information for the 54,948 participants (26,595 girls and 28,353 boys) is shown in Table 1. The subjects’ grades were surveyed almost equally from the 1st to 3rd grades in middle and high school. Regarding economic status, the proportion of male students who answered “high” and “upper middle” was higher. (high 12.7% vs 9.3%, upper-middle 29.3% vs 27.9%). Most of the residential areas were large cities and small cities, with a small fraction in rural areas.
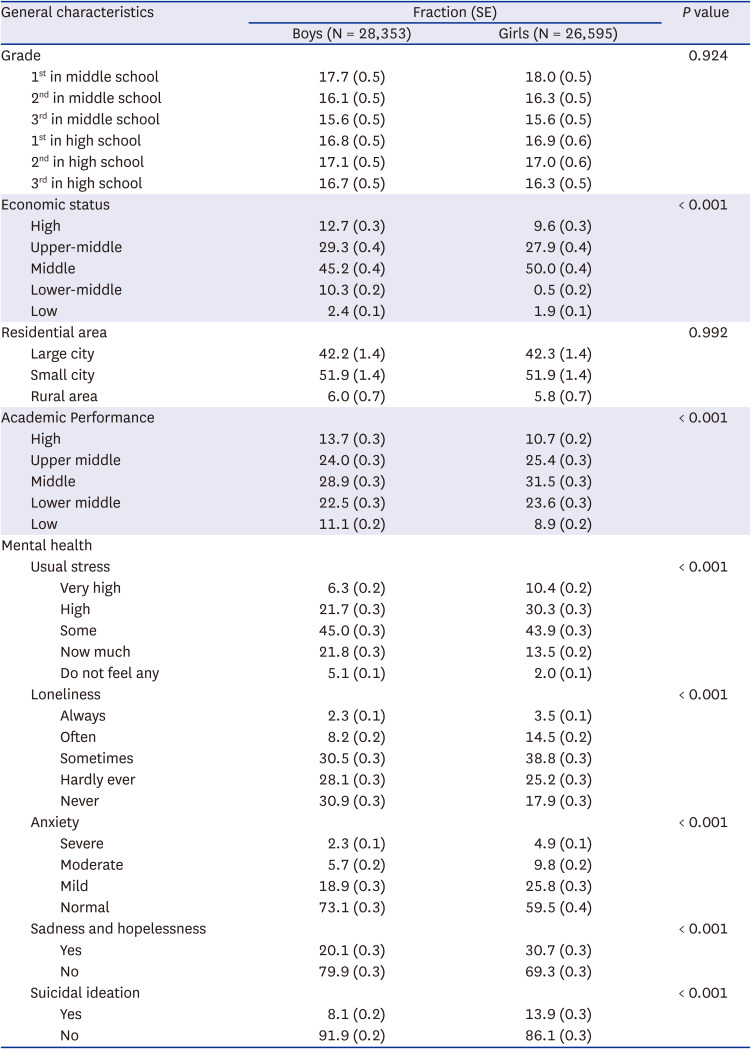
Table 1
Demographic characteristics and mental health factors of the participants (N = 54,948)
![]()
The usual stress rate was higher among girls than boys among the mental health factors. The loneliness experience was also higher in the girls, and conversely, there were many fractions in which boys did not have any (30.9% vs. 17.9%). The rate of “severe” anxiety among girls was more than twice that of boys (2.3% vs. 4.9%). Sadness and hopelessness were higher in female students (20.1% vs. 30.7%), and suicidal ideation was also higher in female students (8.1% vs. 13.9%) (Table 1).
This study aimed to determine the relationship between subjective economic changes caused by COVID-19 and adolescent mental health in boys and girls. The analysis revealed a correlation between subjective economic change caused by COVID-19 and adolescent mental health (usual stress, loneliness, anxiety, sadness and hopelessness, and suicidal ideation). In male students, very high usual stress was 5.8% in not at all economic changes caused by COVID-19 but 15.6% in many economic changes caused by COVID-19. The answer that loneliness is always present was 2.0% in not at all economic changes caused by COVID-19 but 7.0% in many economic changes caused by COVID-19. Severe anxiety was 2.3% in not at all economic changes caused by COVID-19 but 5.8% in many economic changes caused by COVID-19. The proportion of those who answered that they were sad and hopeless was 20.1% in not at all economic changes caused by COVID-19 but 30.7% in many economic changes caused by COVID-19. Suicidal ideation was 8.1% in not at all economic changes caused by COVID-19 but 13.9% in many economic changes caused by COVID-19. In female students, very high usual stress was 9.1% in not at all economic changes caused by COVID-19 but 21.7% in many economic changes caused by COVID-19. The answer that loneliness is always present was 2.7% in not at all economic changes caused by COVID-19 but 9.6% in many economic changes caused by COVID-19. Severe anxiety was 4.2% in not at all economic changes caused by COVID-19 but 11.6% in many economic changes caused by COVID-19. The proportion of those who answered that they had sadness and hopelessness was 25.5% in not at all economic changes caused by COVID-19 but 47.6% in many economic changes caused by COVID-19. Suicidal ideation was 10.8% in not at all economic changes caused by COVID-19 but 26.2% in many economic changes caused by COVID-19 (Table 2).
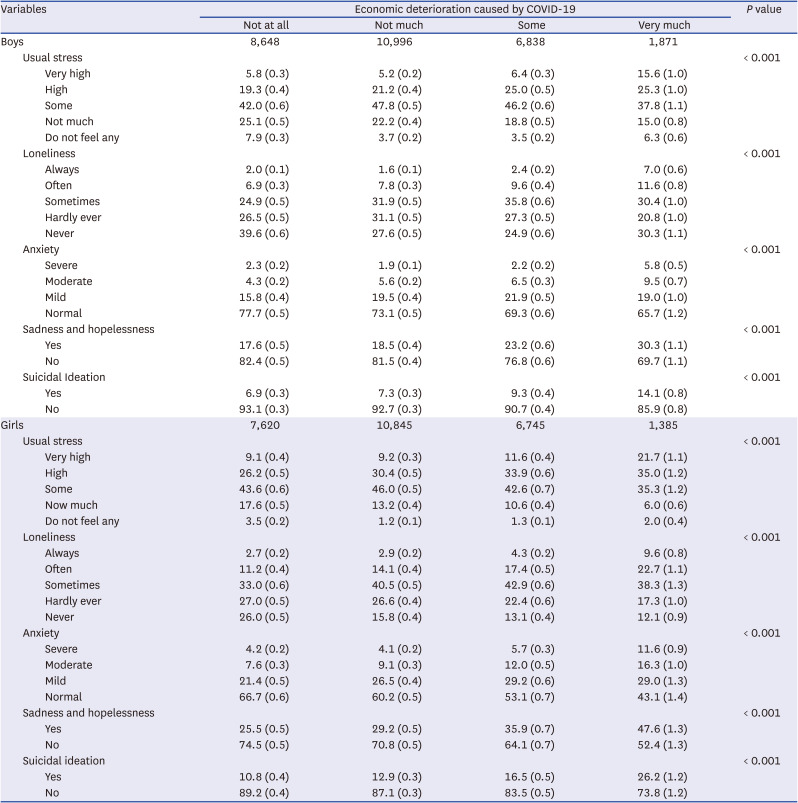
Table 2
Adolescent mental health factors in response to subjective economic changes caused by COVID-19
![]()
A logistic regression analysis was performed to determine the relationship between economic changes due to COVID-19 and adolescent mental health and analyzed after adjusting for grade, academic performance, and economic status. In boys, as the economic changes due to COVID-19 increase, the usual stress odds ratio increases to 1.393, 1.680, and 1.735. The loneliness odds ratios are 0.918, 1.134, and 1.508, respectively. The anxiety odds ratio increased to 1.705, 1.909, and 2.175. Sadness and hopelessness odds ratios changed to 1.309, 1.655, and 1.743, respectively. The suicidal ideation odds ratio increased to 1.409, 1.697, and 1.765. In girls, as the economic changes due to COVID-19 increased, the usual stress odds ratio increased to 1.379, 1.638, and 1.851. The loneliness odds ratio increased to 1.137, 1.424, and 2.058. The anxiety odds ratio increased to 1.527, 1.995, and 2.179, respectively. Sad and hopeless odds ratios changed to 1.457, 1.902, and 1.244, respectively. The suicidal ideation odds ratios increased to 1.503, 1.865, and 2.193 (Table 3).
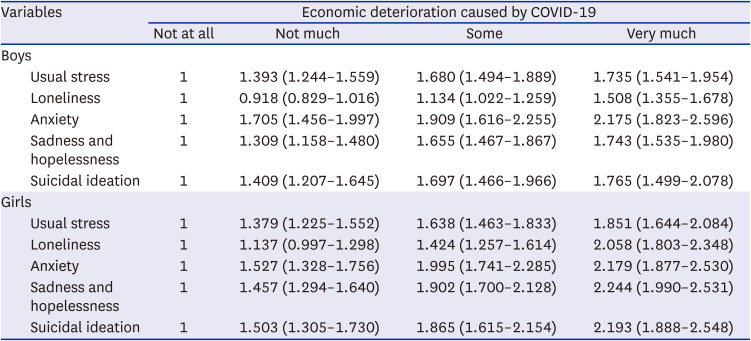
Table 3
Relationship between adolescent mental health and subjective economic deterioration caused by COVID-19
Values are presented as odds ratio (95% confidence interval).
Adjusted by grade, academic performance, and economic status.
COVID-19 = coronavirus disease 2019.
![]()
Go to :
DISCUSSION
Through this study, we investigated the correlation between the subjective economic changes caused by COVID-19 and adolescents’ mental health. The results of this study are based on a large nationally representative sample of South Korean adolescents. To the best of our knowledge, this is the first study to determine the relationship between adolescents’ mental health and the economic deterioration caused by COVID-19. There were more mental health problems in the group with large economic changes caused by COVID-19. Overall, it was found that the mental health factors were worse in female students than in male students. The more severe the economic deterioration caused by COVID-19, the worse the mental health. Anxiety factors due to economic deterioration were the largest among male students, and sadness and hopelessness were the largest among female students.
In this survey, the rate of economic deterioration of households subjectively answered by adolescents was “very much” 5.8%, “somewhat” 24.2%, and in total 30%, respectively. Although the subjective answer lacks objectivity, the rate of economic deterioration caused by COVID-19 seems to be somewhat consistent, with 32.2% in a survey of adults in South Korea.20 Adolescents and adults have similar rates of feeling the deterioration of the household economy.
Several factors resulting from COVID-19 affect adolescents’ mental health. Social isolation on quarantines and lockdowns affects depression and anxiety in adolescents’ mental health.21 Separation from friends, inability to access peer support groups, and face-to-face services have been cancelled worsens their conditions with previous mental health difficulties.2223 Adolescents receive considerable information through traditional media and social media for COVID-19.24 Excessive exposure to COVID-19 media has been associated with increased anxiety levels and stress.25 Adolescents with a history of depression, attention deficit hyperactivity disorder (ADHD), autism, eating disorders, and obsessive-compulsive disorders have more difficulty adjusting to COVID-19 and have potential negative impacts. 2627282930
Many studies have shown that economic deterioration adversely affects the mental health of adults.31323334 However, few studies have examined the economic deterioration and mental health of children and adolescents. Gassman-Pines et al.35 used data from the Youth Risk Behavior Survey and the Bureau of Labor Statistics, and they showed that statewide job loss increases adolescent girls’ suicidal ideation and suicide plans and non-Hispanic blacks’ suicidal ideation, suicide plans, and suicide attempts. Children’s mental health outcomes worsen as the economy weakens.3637 Mihashi et al.38 reported that income reduction was the highest predictive factor of psychological disorder development during recovery following the 2003 SARS outbreak in China. Greek financial crisis has incurred adverse effects on the mental health of the adolescents.39 In 1997, Asia-Pacific countries, such as South Korea had undergone a major financial crisis, which resulted in increase in unemployment rate and income gap between the rich and poor. Consequently, delinquency and suicide increased during this period.40 In addition to these studies, we found that the economic deterioration caused by COVID-19 and deterioration of adolescent mental health correlated with each other. It was also confirmed that the more severe the economic deterioration, the worse the mental health.
This study has some limitations. Since it is based on a self-reporting survey, it may not always be aligned with objective assessments by mental health professionals. Some factors that possibly affect adolescents’ mental health could not be adjusted because the data are secondary, designed by the national agency. There were multicultural families and parents’ educational backgrounds, which could affect adolescents’ mental health in the survey, but it was difficult to include them. It is estimated that about 6.5% of school-age children and adolescents do not attend school in South Korea.41 They may have more mental health problems; however, they were not included in the study.
In conclusion, this research found that the more severe the subjective economic change caused by COVID-19, the greater the impact on adolescent mental health. However, health authorities and government should treat this as a public health issue and investment in well-designed research is needed to evaluate the mental health of children and adolescents and the long impact of COVID-19. We hope that this study will assist with the distribution of disaster subsidies, making policies due to COVID-19, and long-term mitigation will be taken.
Go to :
 XML Download
XML Download