

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Vascular access in hemato-oncologic patients is crucial and challenging, particularly in the pediatric population. Owing to advances in technology, several options are available for vascular access, especially central venous access.1 In pediatric patients who require long-term intermittent vascular access, implantable venous access devices are being widely used. Totally implantable venous access devices (TIVADs) are surgically placed entirely in the subcutaneous tissue at a site that is not apparent externally, even in small infants.23 TIVADs have a number of benefits compared with externally visible access modalities, including the lack of need for local care, infrequent flushes, and lack of restriction of the activity of the child. One other advantage may be the preservation of body image, which is very important in young children and adolescents.1
Complications of TIVAD, including infection, malfunctioning, thrombosis, and mechanical breakage, have been reported in the pediatric population.4 Although a lower rate of TIVAD infection has been reported compared with that of Hickmann catheters, infection is still the most frequent complication of TIVAD.5 Analysis of TIVAD infection rates and risk factors is important in children with cancer because the increased risk of infection due to chemotherapy-induced immunodeficiency and the underlying disease may lead to discontinuation of chemotherapy. Previous studies have reported widespread infection rates according to the definition of catheter-associated infection, ranging from 0.09–2.8 per 1,000 catheter-days or 0.8–7.5% of incidence in various settings.6789 Several risk factors have been described in a few studies, including low leukocyte and platelet counts at the time of insertion, reimplantation, TIVAD insertion prior to chemotherapy, and overweight.91011
As there are limited studies on TIVAD infection, in this study, we investigated the infection rate of TIVADs and evaluated the risk factors, bacterial pathogens, treatment modalities, and outcomes in pediatric patients with cancer at a single center.
Go to : 
METHODS
Patients
This retrospective study included pediatric patients with cancer who were treated at the Department of Pediatrics, Chungbuk National University Hospital, and underwent TIVAD insertion between January 2001 and December 2021. TIVAD insertions were performed by experienced pediatric surgeons in an operating room under strict aseptic conditions.
Data collection
Data were collected from the patients’ electronic medical records. The collection included basic demographics of the patient including sex and age, detailed underlying diagnosis, complete blood cell count (CBC) at the time of insertion, and dates of device insertion and removal. For patients with infection, data on clinical manifestations and CBC at the time of infection, treatment modality, identified pathogen, and the outcomes of infection were collected. Event-free days for the indwelling device were estimated from the day of insertion to the day of the infection event or the day of removal, as appropriate.
Definition and treatment of TIVAD infection
Blood stream infection (BSI) was defined as any clinical symptom with at least one recognized pathogen from obtained blood culture. Soft tissue infection was defined as definite inflammation of the insertion site, regardless of positive blood or aspirated fluid cultures. TIVAD infections were treated with removal surgery, and antibiotic lock therapy or intravenous antibiotics for salvage treatment were administered.
Statistical analysis
Statistical analyses were performed using SPSS for Windows version 25.0 (IBM Corp., Armonk, NY, USA). Variables are presented as frequency, mean, or median with range as appropriate. The incidence rate of infection was estimated by number of infections per year/person. Infection-free TIVAD survival was estimated by Kaplan-Meier analysis. Univariate and multivariate risk factor analysis were performed using Cox regression analysis. P values < 0.05 was considered statistically significant.
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Chungbuk National University Hospital (IRB No. 2019-08-016-001). The need for informed consent was waived by the board.
Go to :
RESULTS
Patients
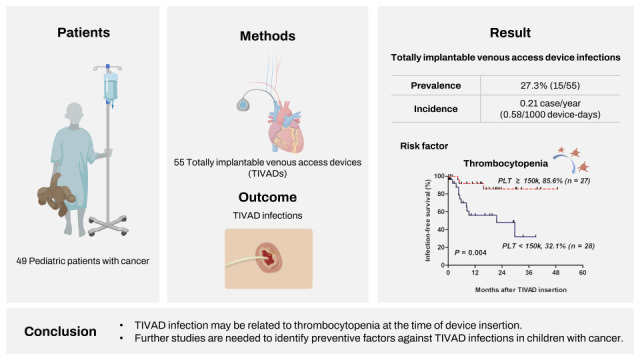
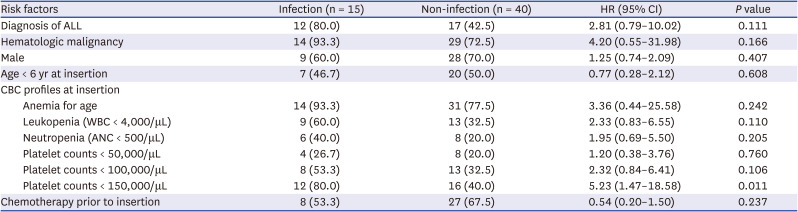
During the study period, 55 TIVADs were performed in 49 patients. Majority of the patients were male (n = 37, 75.6%) and the median age at device insertion was 6.3 (range, 0.3–18.0) years. The median duration of TIVAD use was 386 (range, 6–1,463) days, and the analysis covered a total of 25,954 device days. Among 55 TIVADs, acute lymphoblastic leukemia (ALL) was the most common underlying disease (n = 29, 52.7%) followed by acute myeloid leukemia (n = 8, 14.5%) and lymphoma (n = 5, 9.1%). The 55 cases of TIVAD were divided into two groups according to TIVAD infection status (Table 1). Diagnosis of ALL was more common among the TIVAD infection group compared to the non-infection group (80.0% vs. 42.5%, P = 0.017); other characteristics were comparable between the two groups.
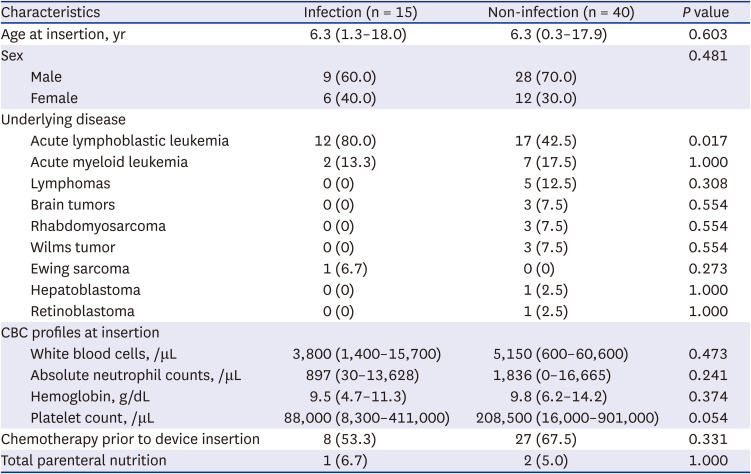
Table 1
Comparisons of demographics according to totally implantable venous access device infection
![]()
Incidence, management, and outcome of TIVAD infection
Table 2 shows the characteristics and treatments among patients with TIVAD infection. Fifteen device infections (27.3%) were observed in 14 patients, which represented an infection rate of 0.21 infections case per TIVAD year (0.58 cases/1,000 device-days). The median duration of TIVAD infection from the time of insertion was 5 months (range, 8 days–30 months). Most infections (12 of 15, 80.0%) occurred within 9 months from TIVAD insertion (Fig. 1). Except for a single case of soft tissue infection, 14 (93.3%) of the 15 infections cases were BSIs with single or multiple identifiable pathogens. Clinical manifestation of the infection presented as fever in all the BSIs, while soft tissue infection presented as granulomatous lesion of the insertion site without clinically evident fever. Coagulase-negative staphylococci were the most common pathogens identified from the BSIs (8 of 15, 53.3%). Other pathogens included Escherichia coli (n = 3, 20.0%), Streptococcus mitis (n = 2, 13.3%), Streptococcus pneumoniae (n = 1, 6.7%) and Enterococcus gallinarum (n = 1, 6.7%). The coagulase negative staphylococci and E. coli were methicillin resistant and positive for extended spectrum beta-lactamase (ESBL), respectively. Device removal was the mainstay of treatment (11 of 15, 73.3%). Of the remaining four cases with salvage management, antibiotic lock therapy was administered in two cases. All the infection cases recovered without permanent sequelae. There were no deaths due to TIVAD infection.
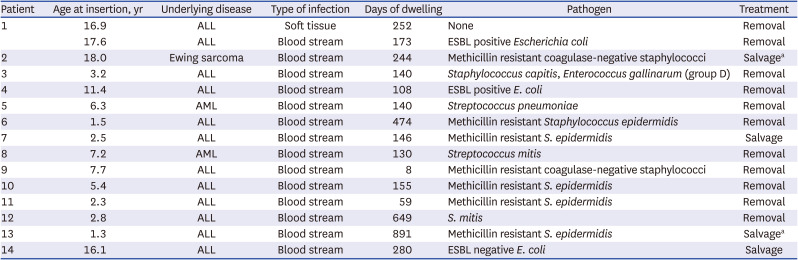
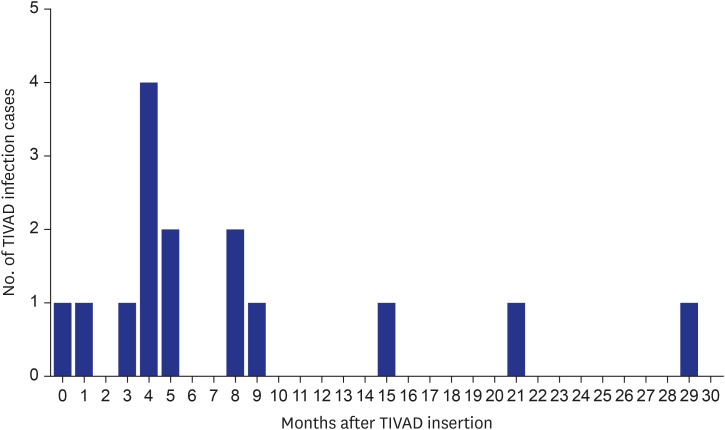
Table 2
Totally implantable venous access device infection characteristics and treatments
ALL = acute lymphoblastic leukemia, ESBL = extended spectrum beta-lactamases, AML = acute myeloid leukemia.
aAntibiotic lock therapy.
![]()
Risk factor analysis for TIVAD infection
In the Kaplan–Meier analysis, infection-free TIVAD survival was higher in the group with normal platelet count at insertion (platelet counts ≥ 150,000/μL) than in the group with thrombocytopenia at insertion (platelet counts < 150,000/μL) (81.3% vs. 32.1%, P = 0.004; Fig. 2). On univariate analysis using Cox regression analysis, platelet counts < 150,000/μL at insertion was statistically associated with TIVAD infection (Table 3). No significant associations with TIVAD infection were found with other factors, including diagnosis of ALL and hematologic malignancy (ALL, acute myeloid leukemia, and lymphomas), sex, age, white blood cell counts, anemia, and chemotherapy prior to insertion. On multivariate analysis, platelet count < 150,000/μL at the time of TIVAD insertion was independently associated with TIVAD infection (hazard ratio, 5.23; 95% confidence interval [CI], 1.47–18.58; P = 0.011).
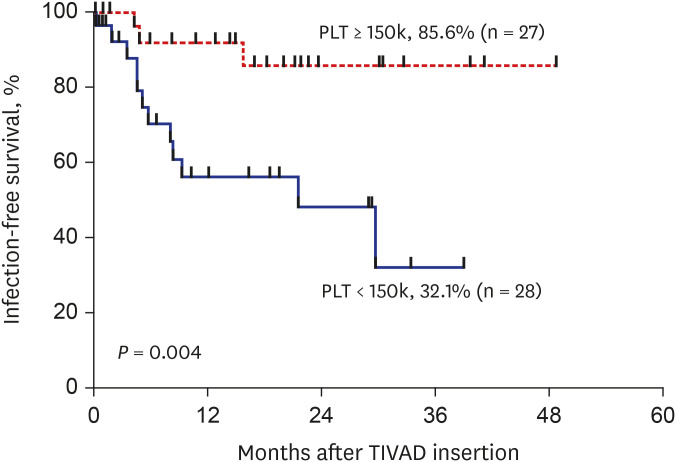 | Fig. 2Kaplan-Meier curves of TIVAD infection according to the presence of thrombocytopenia at the time of insertion.TIVAD = totally implantable venous access device, PLT = platelet count.
|
Table 3
Risk factors analysis for totally implantable venous access device infection
Values are presented as number (%).
HR = hazard ratio, CI = confidence interval, ALL = acute lymphoblastic leukemia, CBC = complete blood cell count, WBC = white blood cell count, ANC = absolute neutrophil count.
![]()
Go to :
DISCUSSION
There were two major findings of this study: 1) the infection rate of TIVAD was 0.21 cases per device-year (0.58 cases/1,000 device-days), and 2) TIVAD infection was associated with thrombocytopenia at the time of device insertion. The majority of infections occurred within 9 months after TIVAD insertion and methicillin-resistant coagulase-negative staphylococci were the most common pathogens causing BSI.
TIVAD has been used since the 1980s for multiple vascular access in long-term medical treatment.12 TIVAD offers multiple benefits not only for patients with cancer, but also for patients with chronic diseases, such as cystic fibrosis and metabolic diseases; however, it appears to be most beneficial for pediatric patients with cancer exhibiting difficult vascular access.1314 Notably, despite the benefits of TIVAD over peripheral access, inherent complications persist. A study that analyzed 209 TIVADs in 200 patients with cancer aged < 15 years reported that 21 TIVADs were removed because TIVAD-related complications, with infection being the most common complication (0.66/1,000 catheter-days, 11.9%), followed by mechanical problems and venous thrombosis.6 Another study that included 128 pediatric oncology patients with TIVADs demonstrated that BSI was the most prevalent complication (0.17/1,000 catheter-days), followed by thrombosis, dislodgement, and occlusions.15 Even with a reduction in the risk of microbial contamination due to total implantation under the skin, 3–10% of TIVAD carriers experience a related infection, which is the most common indication for device removal.1617
The infection rates vary among studies because of differences in underlying disease, immunodeficiency level, and definition of device infection.17 Our study showed an expected infection rate of 0.58, which was similar to previous studies that reported 0.09–2.8 infections per 1,000 device-days.6 However, infection occurred in 27.3% of all patients with TIVADs in our study, and most of the infections (12/15, 80.0%) occurred in the first 9 months after insertion. This may explain the reason behind long-term infection-free survival when the device is stored without problems for a period of time after insertion. Further research should be conducted to reduce the initial infection rate after TIVAD insertion.
Our study revealed that thrombocytopenia was a major risk factor for TIVAD infection. Previous studies have investigated the association between TIVAD infection and the conditions at the time of TIVAD insertion.1011 A study of 188 pediatric oncology patients with 77,541 catheter-days, revealed that a white blood cell count < 1,000/μL on the day of implantation was a risk factor for TIVAD infection (risk ratio, 1.64; 95% CI, 1.22–2.26; P = 0.003).11 Another study that included 238 devices implanted in 225 hemato-oncology pediatric patients found that risk factors for infection were an absolute neutrophil count of < 500/μL and platelet count of < 50,000/μL.10 As neutropenia and thrombocytopenia derive from bone marrow suppression that is caused by hematologic malignancies and requires intensive chemotherapy with multiple handling of the device, they could be surrogate markers of the patient’s general immunocompetence. Compared to previous studies, low platelet count, but not neutrophil count, was associated with TIVAD infection in our study. However, it is difficult to conclude that thrombocytopenia is a risk factor for TIVAD infection from these results alone because of the small number of patients in our study and the possible presence of various confounding variables. Furthermore, the degree of association between thrombocytopenia and TIVAD infection should be considered. In the current study, mild thrombocytopenia (just below the reference value) was a major risk factor for TIVAD infection, which is distinct from the findings of a previous study which concluded that severe thrombocytopenia was associated with TIVAD infection.10 We assume that this may highlight the importance of normal reference values for CBC parameters. However, further studies are needed, as studies on this particular subject are lacking.
The most common pathogens identified in this study were coagulase-negative staphylococci, which is consistent with previous studies.1118 The proportion of Gram-positive and Gram-negative species varies among studies; however, our study reported a relatively low proportion of Gram-negative species. Possible reasons for this may include a relatively low level of immunodeficiency among the patients in this study; however further investigations are needed. All staphylococci were methicillin resistant, and majority of E. coli harbored the ESBL gene, indicating that the pathogens are highly resistant to major antibiotics. These findings reconfirm the necessity of broad-spectrum antibiotics for the empirical management in patients with possible central line infections.19
The outcomes of patients with TIVAD infections were favorable, with no cases of mortality in this study. The major strategy against infection was removal of the device, which might have contributed to this result. Four patients were managed for device salvage, with two cases of antibiotic locking therapy. As there are ongoing controversies regarding the benefits of trying to retain the device using antibiotic lock therapy, conservative managements with salvage therapy in select patients might be the best approach.1920
This study had several limitations. Most importantly, the number of patients and corresponding device days were limited. To thoroughly analyze the risk factors for device infections, a much greater number of inserted devices seems needed. Further, in our study, we could not analyze the relationship between prophylactic antibiotics for device implantation and TIVAD infection. Although new strategies have been proposed in an attempt to reduce the risk of central-line associated BSIs, knowledge of prophylactic antibiotics prior to insertion of TIVADs is limited, especially in the pediatric population. Further studies are needed to validate our findings and identify preventive factors, such as prophylactic antibiotic therapy against TIVAD infections in children with cancer. Despite these limitations, we believe our study adds knowledge to the field of TIVAD infections and may guide physicians to improve the management of TIVAD and related infections.
This study identified infection as one of the major drawbacks of TIVAD, despite the benefits of improved vascular access. Our study showed that thrombocytopenia at insertion may be associated with TIVAD infection and platelet count can be used as a prognostic predicting factor of clinal outcome in patients who have had TIVAD insertions. TIVADs are important means for pediatric patients with cancer; therefore, it is necessary to reduce the complications of infection, especially the initial complications that occur after insertion. Further studies are needed to validate our findings and identify preventive factors against TIVAD infections in children with cancer.
Go to :
 XML Download
XML Download