

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has been quickly spreading worldwide.1 The World Health Organization (WHO) declared the COVID-19 outbreak a global pandemic in March 2020. According to previous reports, 80–90% of cases were asymptomatic or showed mild respiratory symptoms or fever, classified as mild pneumonia.23 However, the remainder of the patients had severe pneumonia requiring oxygen therapy, particularly those with comorbidities and impaired immune function developed severe or critical illness. Severe COVID-19 was associated with acute respiratory distress syndrome (ARDS), and affected patients received high-flow oxygen therapy, mechanical ventilation, and extracorporeal membrane oxygenation (ECMO) therapy.4 A recent study reported that among 173 COVID-19 patients with severe disease activity, 38.7% required mechanical ventilation, 2.9% received ECMO therapy, and 8.1% died.5 Fatality rate is higher in elderly, reaching 14% in patients aged 80 or older in Korea.6
Several studies have investigated the long-term impairments in the physical function of affected individuals since the onset of the COVID-19 pandemic. In previous studies of ARDS, most survivors suffered from persistent intensive care unit (ICU)-acquired weakness and could not recover completely, as their functional limitation lasted for years.7 Similarly, impaired exercise capacity was common in survivors of SARS and Middle East respiratory syndrome.8 In COVID-19, some studies have reported that 30–40% of patients had neurologic manifestations, and critical illness polyneuropathy and critical illness myopathy were the main causes of ICU-acquired weakness.910 Post-acute COVID-19 patients are at risk for functional impairment, muscular performance, and fatigue.1112 A recent one-year follow-up study of survivors of COVID-19-associated ARDS reported long-lasting impairments in physical, cognitive, and mental health status.13
There is a consensus that early rehabilitation is crucial to avoid impairments in physical function, cognition, and mental health resulting from prolonged immobility in the ICU, thus preventing critical illness polyneuropathy or critical illness myopathy and improving long-term functional recovery.141516 Also, rehabilitation was shown to reduce the rate of 30-day ICU readmission and revisit to emergency room in ICU survivors.17 Most mild-to-moderate COVID-19 patients fully recover to premorbid functional status and return to normal social life without any disabilities. In contrast, physical and functional recovery in severe COVID-19 patients may be slow, and long-term sequelae are more likely to ensue in severe-to-critical COVID-19 patients, raising the socioeconomic burden.1819
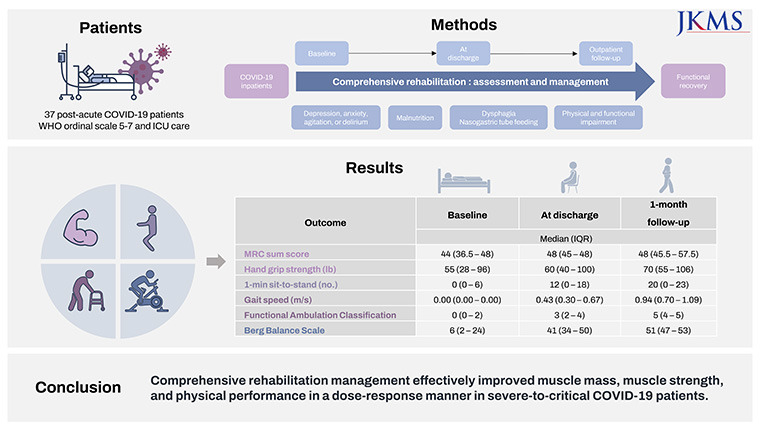
Several studies have explored the feasibility and effect of rehabilitation on physical function in COVID-19 survivors.202122 However, as far as we know, existing studies have not followed up on the effect of rehabilitation on COVID-19 patients after discharge, and the majority have investigated rehabilitation of whole COVID-19 patient cohorts regardless of disease severity. Therefore, this study focused on the rehabilitation of patients with severe COVID-19 in a tertiary university hospital. We performed comprehensive rehabilitation management and evaluated the effect of intervention on physical function in survivors of severe COVID-19 at the time of discharge and at 1 month post-discharge. Additionally, we investigated the effect of the dose of rehabilitation on physical and functional recovery and the correlation between improved functional outcomes and clinical parameters in this group.
Go to : 
METHODS
Study design and participants
This longitudinal, single-center retrospective cohort study was designed according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. The World Health Organization (WHO) suggested an 8-point ordinal scale to describe the illness severity of COVID-19 on February 18, 2020. The ordinal scale is as follows: 0, uninfected (no clinical or virological evidence of infection); 1, ambulatory and no limitation of activities; 2, ambulatory with limitation of activities; 3, hospitalized, no oxygen therapy; 4, hospitalized, oxygen by mask or nasal prongs; 5, hospitalized, non-invasive ventilation or high-flow oxygen; 6, hospitalized, intubation and mechanical ventilation; 7, hospitalized, ventilation with additional organ support (e.g. pressors, renal replacement therapy, extracorporeal membrane oxygenation); 8, death.23 We included COVID-19 inpatients who were admitted to the nationally designated isolation units24 from March 2020 to September 2021 and those who 1) underwent intensive care for at least 2 days, 2) were classified as patients with severe COVID-19 (WHO ordinal scale of 5–7), and 3) participated in the rehabilitation program, and 4) in whom negative conversion was confirmed with two consecutive tests. Participants who had started the rehabilitation program but died (WHO ordinal scale of 8) before discharge were excluded.
COVID-19 was diagnosed according to positive real-time reverse-transcription polymerase chain reaction (RT-PCR) results for SARS-CoV-2 in upper respiratory specimens. The negative conversion of the virus was confirmed by two consecutive RT-PCR tests of upper respiratory specimens. After receving a negative result, patients who still needed mechanical ventilation, high-flow oxygen therapy, or frequent assessments of vital signs were transferred from the isolation ICU to the non-isolation ICU, and the others were transferred to the general ward. When patients tested negative, the critical care physician consulted the rehabilitation physician about rehabilitative evaluation and management. At the time of consultation, the rehabilitation physician evaluated the patients’ medical and physical status and determined whether they could participate in the exercise program in the physiotherapy (PT) room. If patients did not show dyspnea and saturation of percutaneous oxygen (SpO2) at rest was 92% or more when oxygen support of upto 3 L/min is provided, the PT room program was performed. Otherwise, if patients still required more than 3 L/min oxygen at rest and required frequent vital sign assessments, the exercise program was conducted bedside instead; the PT room program was performed once the patient was stable.
Comprehensive rehabilitation management
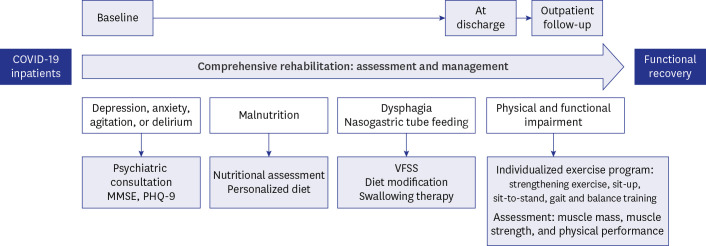
Comprehensive rehabilitation consisted of a multi-component assessment and management strategy (Fig. 1). Participants attended the exercise program in the PT room or at the bedside. The program was offered once daily on weekdays by trained physical therapists. Nevertheless, some patients who were physically confident enough to participate in more exercise sessions received two times of exercise sessions in a day. The individualized exercise program started after baseline assessment. The sessions consisted of a warm-up, conditioning and strengthening exercises, and cool-down in PT room programs. Patients usually received strengthening exercises of the upper and lower extremities, sit-up and sit-to-stand training, sitting and standing balance training, gait training with or without ambulation aids, step-up and step-down training, and aerobic exercise (e.g. cycle ergometry, walking). The total duration of one session took 30 minutes.25 Physical therapists also provided instructions for an exercise program at home after discharge.
Each program was individualized to participants’ current physical function. In bedside programs, patients underwent gentle range-of-motion exercise of all major joints, stretching exercise, strengthening exercises of upper and lower extremities (e.g., quadriceps setting exercise, ankle pump exercise, bridge exercise), and sitting balance training for approximately 10 minutes. Weight-bearing exercises such as sit-to-stand training or standing balance training were not included in bedside programs as the patients were still at risk for oxygen desaturation. Each bedside program was individualized to patients’ current physical function, the same as the PT room program.
During hospitalization, trained dietitians evaluated the patients’ nutritional status. Nutritional assessment was based on the modified version of a standardized set of diagnostic characteristics used to detect adult malnutrition according to the consensus statement of the Academy of Nutrition and Dietetics and the American Society for Parenteral and Enteral Nutrition.26 Subsequently, a personalized diet was recommended to every patient according to their nutritional status. The target daily intake of calories and proteins was individualized based on the patients’ ideal body weight or adjusted body weight (in case of obesity); the daily protein intake ranged from 1.2 to 1.8 g/kg.27
For safe feeding of those who switched from nasogastric tube feeding to direct oral feeding, a videofluoroscopic swallowing study (VFSS) was performed;28 patients with dysphagia were instructed to use compensation techniques and swallowing maneuvers, and they were recommended to engage in swallowing therapy.29
Many participants experienced depressive moods, anxiety, agitation, or delirious characteristics because of the long hospitalization and prolonged stay in the ICU. In these cases, patients were referred for psychiatric consultations and were assessed using the Patient Health Questionnaire-9 (PHQ-9) if needed.30 In supportive interviews, psychiatrists assessed patients’ main symptoms and possible causes of psychological problems. Antidepressants or antipsychotics were prescribed on a case-by-case basis if needed.
Outcome measures and follow-up
We aimed to evaluate the effect of comprehensive rehabilitation management on the physical and functional recovery of severe-to-critical COVID-19 patients, especially on muscle mass, strength, and physical performance. Appendicular skeletal muscle mass index (SMI) was calculated by dividing the total skeletal muscle mass of all four limbs by the square of the height. Body fat mass and muscle mass were measured based on bioelectrical impedance analysis using Inbody S10 (Inbody, Seoul, Korea). Muscle strength was evaluated based on the handgrip strength and Medical Research Council (MRC) sum score. The handgrip strength of both hands was measured using a dynamometer. Handgrip strength is associated independently with poor hospital outcome.31 MRC sum score is the summation of each MRC scale score in six major bilateral muscles (shoulder abductor, elbow flexor, wrist dorsiflexor, hip flexor, knee extensor, and ankle dorsiflexor). MRC sum score below 48 suggests significant weakness, and a score below 36 suggests severe weakness.32 Both handgrip strength and MRC sum score revealed good inter-rater reliability.3334 The number of repetitions in the 1-min sit-to-stand test,3536 gait speed, Berg Balance Scale (BBS) scores,37 and Functional Ambulation Classification (FAC; scored from 0 to 5) scores were also used to assess physical performance.38 Ten-meter walk test was used to measure gait speed.3940 Those tests demonstrated good inter-rater reliability in previous studies.3637383940
In our study, the trained physical therapists who were well-informed of the assessment method evaluated the outcome variables at baseline, discharge, and outpatient follow-up. Although the same assessor did not perform the assessments in many cases, each outcome measure was shown to have good inter-rater reliability in previous studies.33343637383940 Baseline assessment was performed upon initiation of the exercise program in the PT room and included an evaluation of physical status, cognitive function, and psychiatric status. Cognitive function was evaluated using the Mini-Mental Status Examination (MMSE), and self-assessment of mood was conducted using the PHQ-9.30
Comprehensive rehabilitation management started after baseline assessment. Muscle mass, strength, physical performance, cognitive function, and self-reported mood were subsequently assessed at discharge. Routine outpatient follow-up was conducted 1 month after discharge and included a reassessment of muscle mass, strength, and physical performance.
As the dose of rehabilitation is of great importance, its correlation with functional improvements was analyzed. The rehabilitation dose was calculated in two ways: the number of days of rehabilitation and the total time spent on rehabilitation. The latter was calculated by multiplying the time spent on exercise sessions (minutes) and the number of exercise sessions at each site (i.e., 30 × the number of PT room sessions + 10 × the number of bedside sessions). Since the time spent in the PT room program was about three times longer than that in the bedside program, the dose of rehabilitation was calculated in these two ways. The correlation between the dose of rehabilitation and functional improvement was analyzed.
Data collection
Demographic, clinical, laboratory, radiologic, and functional outcome data were extracted from electronic medical records. The contents and doses of rehabilitation were also collected. Demographic data included age, sex, height, weight, body mass index, date of birth, smoking history, and Charlson comorbidity index (CCI). Additionally, the date of confirmation of COVID-19, date of negative conversion, length of ICU stay, the total length of hospital stay, and duration of mechanical ventilation were collected.
All patients underwent intensive care and routine laboratory tests at ICU admission. From the data collected at the time of ICU admission, we calculated the Acute Physiology and Chronic Health Evaluation (APACHE) II scores to estimate the ICU mortality and severity of COVID-19; the APACHE II score is a known effective tool to predict hospital mortality in COVID-19.41 The use of a systemic corticosteroid, antiviral and neuromuscular-blocking agents, and antidepressant and antipsychotic drugs was investigated. Vital signs, laboratory results, nutritional status, and dose of oxygen therapy at the beginning of rehabilitation were collected in addition to functional assessment at baseline, discharge, and 1 month after discharge.
In-hospital and 1-month outpatient department follow-up measurements of SMI and body fat mass were also collected. In-hospital measurements of SMI and body fat mass were conducted several times at different time points, which showed different ratios of extracellular water and total body water. Among them, one in-hospital measurement was selected, as it revealed a closer value of extracellular/total body water than that taken at the 1-month follow-up. All data were extracted using a standardized data collection form.
Statistical analysis
Statistical analysis was performed using R software (version 4.0.5, R Foundation for Statistical Computing, Vienna, Austria) and SPSS software (version 19.0, SPSS Inc., Chicago, IL, USA). Continuous parameters are shown as mean ± standard deviation. Categorical parameters are presented as numbers and percentages. Median and interquartile range (IQR) were calculated for each outcome parameter. Pairwise comparisons of functional assessments between baseline and discharge were analyzed using the Wilcoxon-signed rank test. A P value of < 0.05 was considered significant. Functional assessments at the three time points were analyzed using a non-parametric Friedman test. A value of P < 0.016 was considered to indicate significance after the Bonferroni adjustment. In-hospital and out-of-hospital measurements of the SMI and body fat mass were analyzed using the Wilcoxon-signed rank test. Spearman’s rank correlation test was used to investigate the correlation between functional improvement and dose of rehabilitation. Furthermore, non-parametric partial correlation analysis was used to avoid confounding effects of other demographic and clinical parameters. Age, sex, CCI, and WHO ordinal scale were included as control factors in partial correlation analysis. Spearman’s rank correlation test was also performed to analyze associations between functional improvement and other clinical and demographic parameters. Spearman’s rank correlation coefficient (ρ) and P value are shown in the tables and figures.
Ethics statement
This single-center retrospective cohort study (clinical trial registration number: NCT05104411) was approved by the Institutional Review Board (IRB) of Seoul National University Bundang Hospital (B-2108-705-112), and the IRB approved the waiver for informed consent. This study was conducted according to the Declaration of Helsinki.
Go to :
RESULTS
Baseline characteristics
Thirty-seven patients were enrolled in this cohort study; their baseline characteristics are summarized in Table 1. The mean age of the participants was 64.1 ± 12.7 years. All patients were classified as levels 5–7 on the WHO ordinal scale; 59.5% underwent intubation and mechanical ventilation and 32.4% required ECMO. The mean lengths of stay in the hospital and at the ICU were 63.8 ± 36.5 and 33.6 ± 23.9 days, respectively. The mean quarantine period was 31.0 ± 11.5 days. Pneumonic infiltration of the bilateral lung was observed in all patients.
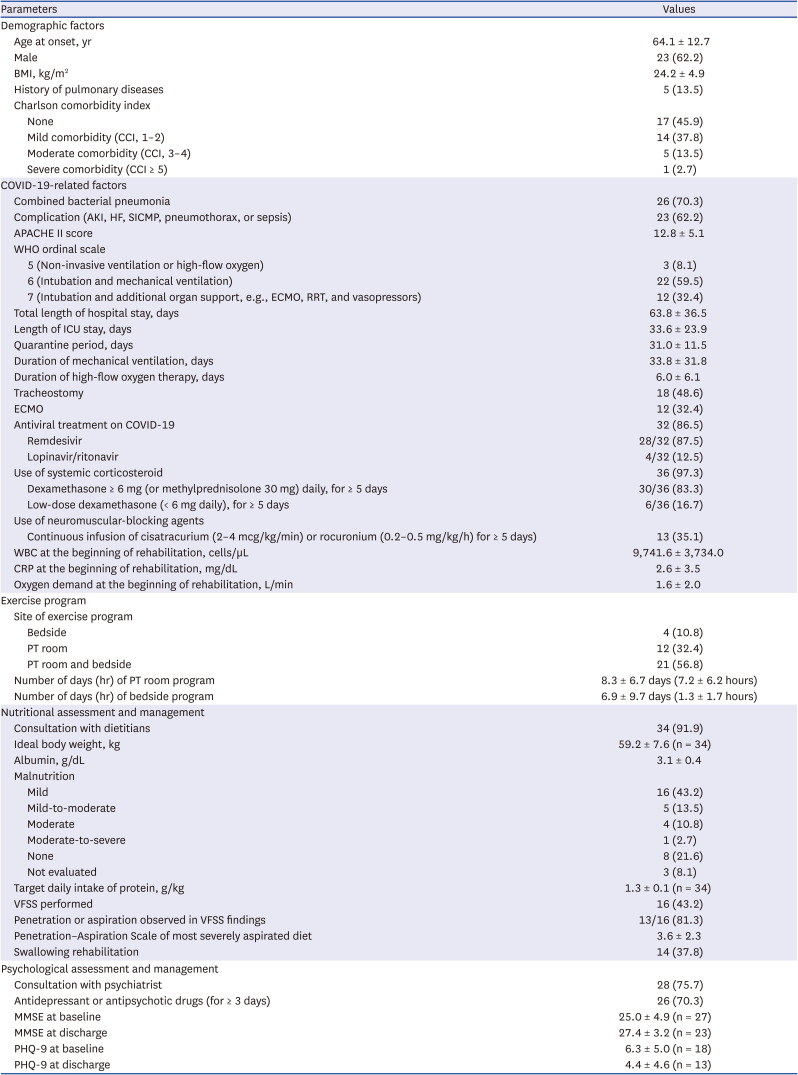
Table 1
Baseline characteristics of the 37 included patients
Continuous parameters are presented as mean ± standard deviation and categorical parameters are presented as numbers (%).
BMI = body mass index, CCI = Charlson comorbidity index, COVID-19 = coronavirus disease 2019, AKI = acute kidney injury, HF = heart failure, SICMP = stress-induced cardiomyopathy, APACHE II = Acute Physiology and Chronic Health Evaluation II, WHO = World Health Organization, ECMO = extracorporeal membrane oxygenation, RRT = renal replacement therapy, ICU = intensive care unit, WBC = white blood cell count, CRP = C-reactive protein, PT = physiotherapy, VFSS = videofluoroscopic swallow study, MMSE = Mini-Mental Status Examination, PHQ-9 = Patient Health Questionnaire-9.
![]()
All patients were independent community ambulators before diagnosis with COVID-19 (FAC: 5). No comorbidity was present in 45.9% of the patients, whereas 37.8% had mild (CCI, 1–2), 13.5% had moderate (CCI, 3–4), and 2.7% had severe comorbidities (CCI ≥ 5). A total of 86.5% of patients received antiviral therapy, and the majority of them received remdesivir intravenously. Systemic corticosteroids were used in 97.3% of the patients, most of whom received dexamethasone 6 mg (or methylprednisolone 30 mg) or more daily for 5 days or longer. Overall, 35.1% of the patients received a continuous infusion of neuromuscular-blocking agents for 5 days or longer. The mean APACHE II score calculated within 24 hours of ICU admission was 12.8 ± 5.1. Tracheostomy was conducted in 48.6% of the patients, as they were expected to have prolonged intubation periods.
Of all patients engaged in the exercise program at the PT room or bedside, 56.8% started the program at the bedside and switched to the PT room as their medical condition stabilized, 32.4% exclusively engaged in the PT room program, and 10.8% in the bedside program. The duration of the exercise program at the PT room and bedside was 8.3 ± 6.7 and 2.3 ± 3.2 hours, respectively. The oxygen demand at the beginning of rehabilitation was 1.6 ± 2.0 L/min.
In total, 91.9% of the patients consulted dietitians and underwent nutritional assessments; 70.2% revealed malnutrition regardless of its severity. Safe oral feeding was performed in 43.2% of the patients after evaluation on swallowing function using VFSS, and all except for two of these patients received swallowing therapy. Among those who received VFSS, only 18.7% did not show aspiration or penetration. Overall, 75.7% of the patients consulted psychiatrists, and 70.3% were prescribed antidepressants or antipsychotics. The mean PHQ-9 and MMSE scores at baseline assessment were 6.3 ± 5.0 and 25.0 ± 4.9, respectively.
Short-term follow-up of functional outcomes following comprehensive rehabilitation management
Baseline functional assessments were conducted on the first day of the exercise program at the rehabilitation unit, followed by reassessments at the time of discharge and 1-month (35.0 ± 16.6 days after discharge) outpatient follow-up. Compared with the values at baseline, significant improvements were noted in the MRC sum score and both handgrip strength at the time of discharge and 1-month outpatient follow-up (median, 44 [IQR, 36.5–48] vs. 48 [45–58] vs. 48 [45.5–57.5]; median, 55 [IQR, 28–96] vs. 60 [40–100] vs. 70 [55–106] lb, respectively) (Table 2). The number of repetitions in the 1-min sit-to-stand test was significantly improved (median, 0 [IQR, 0–6] vs. 12 [0–18] vs. 20 [0–23]). In the evaluation of physical performance, gait speed, FAC, and BBS were significantly improved (median, 0.00 [IQR, 0.00–0.00] vs. 0.43 [0.30–0.67] vs. 0.94 [0.70–1.09] m/s; median, 0 [IQR, 0–2] vs. 3 [2–4] vs. 5 [4–5]; median, 6 [2–24] vs. 41 [34–50] vs. 51 [47–53], respectively). We also observed a significant increase in the SMI between in-hospital and 1-month follow-up measurements, whereas the body fat mass remained unchanged (Table 3).
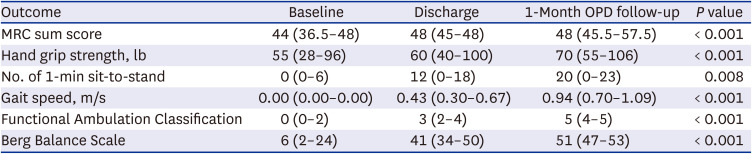

Table 2
Comparison of outcome parameters at baseline, discharge, and 1-month OPD follow-up
Values are presented as median (interquartile range).
OPD = outpatient department, MRC = Medical Research Council.
![]()
Table 3
Skeletal muscle mass index and body fat mass between in-hospital and 1-month follow-up assessment
| Outcome | In-hospital | 1-Month OPD follow-up | P value |
|---|---|---|---|
| Appendicular skeletal muscle mass index (kg/m2) | 5.80 (5.39–7.05) | 6.13 (5.24–7.76) | 0.012 |
| Body fat mass (kg) | 21.8 (15.1–30.7) | 22.2 (17.6–31.2) | 0.394 |
![]()
Association between the dose of rehabilitation and functional improvements
We analyzed associations between the number of days of rehabilitation and the improvements in each outcome measures. Among them, FAC and BBS showed significant positive associations with the number of days of rehabilitation (P = 0.011 for FAC and P = 0.003 for BBS), whereby moderate correlations were identified for FAC (ρ = 0.48) and BBS (ρ = 0.56) in unadjusted Spearman’s rank correlation analysis (Fig. 2, Table 4). Partial correlation analysis (Age-, sex-, CCI- and WHO ordinal scale-adjusted) revealed that the dose of rehabilitation was still moderately correlated with FAC and BBS (ρ = 0.46, P = 0.027; ρ = 0.50, P = 0.019, respectively). In addition, we analyzed associations between the time spent on rehabilitation and the improvements in each outcome measure. BBS showed statistically significant positive associations with time (ρ = 0.39, P = 0.049), while the others showed no statistically significant associations (P > 0.05).

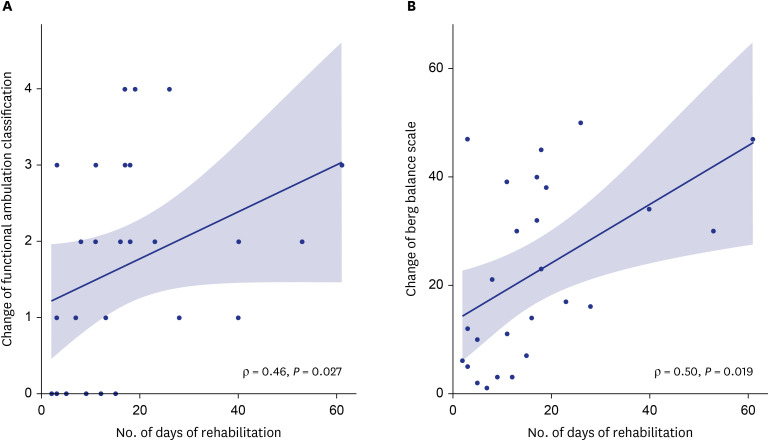 | Fig. 2Adjusted Spearman’s partial correlation between rehabilitation dose and improvement of outcome parameters (age, sex, Charlson comorbidity index, WHO ordinal scale used as control factors). (A) Changes in FAC from baseline to discharge showed positive associations with the number of days of rehabilitation (ρ = 0.46, P = 0.027) and (B) Changes in BBS from baseline to discharge also showed moderate correlation with the number of days of rehabilitation (ρ = 0.50, P = 0.019).WHO = World Health Organization, FAC = Functional Ambulation Classification, BBS = Berg Balance Scale.
|
Table 4
Correlation between rehabilitation dose and improvement of outcome parameters
| Outcome | Unadjusted Spearman’s correlation | Adjusted Spearman’s partial correlation | ||
|---|---|---|---|---|
| ρ | P | ρ | P | |
| Dose of rehabilitation – FAC | 0.48 | 0.011 | 0.46 | 0.027 |
| Dose of rehabilitation – BBS | 0.56 | 0.003 | 0.50 | 0.019 |
ρ: Spearman’s rank correlation coefficients; adjusted Spearman’s partial correlation analysis used age, sex, Charlson comorbidity index, WHO ordinal scale as control factors.
FAC = Functional Ambulation Classification, BBS = Berg Balance Scale, WHO = World Health Organization.
![]()
Association between functional improvements and clinical parameters
A summary of the moderate or strong associations between functional improvementsfifth and other clinical and demographic parameters is provided in Table 5. Between baseline and 1-month follow-up, those with higher PHQ-9 scores at baseline showed minor improvements in the number of repetitions in the 1-min sit-to-stand test and gait speed among various functional outcomes. Older age, longer hospitalization, longer ICU stay, longer duration of mechanical ventilation, and tracheostomy were associated with reduced improvements in gait speed. Patients with higher serum albumin levels demonstrated more significant improvements in gait speed. Besides, patients with higher MMSE scores showed more significant gait speed improvements between baseline and discharge (ρ = 0.40, P = 0.050).

Table 5
Correlation between improvement of functional outcomes and clinical parameters (between baseline and 1-month OPD follow-up)
![]()
Go to :
DISCUSSION
In this longitudinal retrospective cohort study of survivors from severe-to-critical COVID-19, comprehensive rehabilitation management, including exercise training and nutritional and psychological support, improved muscle strength, balance function, and ambulatory function during hospitalization and 1 month after discharge. To the best of our knowledge, this is the first observational cohort study to investigate the lasting beneficial effects of comprehensive rehabilitation management after discharge in severe-to-critical COVID-19 survivors from a tertiary hospital.
A single week of immobilization in an intensive care setting suffices to cause muscle atrophy, that is, a muscle weakness that is further aggravated in patients with a critical illness.42 Long-term complications associated with disuse atrophy, critical illness polyneuropathy, and myopathy lead to long-lasting limitations in physical function.43 Prevalent use of systemic corticosteroid and neuromuscular-blocking agents also contribute to ICU-acquired weakness. One large cohort study on long-term consequences of COVID-19 reported that the severely affected subgroup (requiring high-flow nasal cannula, non-invasive mechanical ventilation, and/or invasive mechanical ventilation) commonly experienced muscle weakness (81%) and decreased walking distance (29%) at 6 months after discharge.19 It was further demonstrated that 79% of patients with COVID-19 who did not require mechanical ventilation exhibited walking distance below their age-adjusted predicted values at a 6-week follow-up.44
Lessons learned from the outbreak of SARS in Hong Kong in 2003 include that exercise training programs effectively enhance the recovery of cardiopulmonary and musculoskeletal function and health-related quality of life in SARS survivors.45 A cohort study conducted at a COVID-19 rehabilitation unit revealed that rehabilitation improved the Barthel index, sit-to-stand frequency, and grip strength of affected individuals at discharge; however, only a relatively small number of severe patients were included (13 intubated patients), and long-term effects of rehabilitation were not investigated.22
Our study exclusively included survivors of severe-to-critical COVID-19 in the tertiary hospital, who were expected to experience functional decline after acute care based on their scores of 5–7 on the WHO ordinal scale. The duration of ICU stay was longer compared with the relatively short durations in other studies (10.22 ± 4.87 days in the study by Piquet et al.,22 19 ± 14 days in the study by Puchner et al.,46 17.98 ± 8.66 days in the study by Curci et al.,47 and 20 ± 13 days in the study by Rodrigues et al.21). Moreover, the APACHE II score was slightly higher in our study than in another retrospective cohort study of COVID-19 survivors (10.87 ± 4.40).41 Judging by the APACHE II score and duration of ICU stay, the severity of participants in our study was more severe than in previous studies.2122414647 Despite the severe-to-critical disease severity in our study, comprehensive rehabilitation management, including exercise training in addition to nutritional and psychological support, led to a significant improvement in muscle strength (MRC sum score and handgrip strength) and physical functional performance (1-min sit-to-stand repetitions, FAC, BBS, and gait speed) at discharge.
ICU survivors commonly experience muscle weakness and fatigue and often become bedridden even after a period of acute intensive care,194849 which becomes a vicious cycle of prolonged deterioration of muscle function and physical performance. Early rehabilitation is crucial to circumvent these ICU-associated issues. Herein, we demonstrated that inpatient rehabilitation was the first step of recovering from deconditioning in survivors of severe-to-critical COVID-19. Similarly, muscle strength and physical functional performance continued to improve in response to rehabilitation during the 1-month follow-up assessment after discharge. These observations highlight the lasting effects of inpatient rehabilitation and education of patients toward a home exercise program. A few studies investigated multi-disciplinary or comprehensive inpatient rehabilitation of post-acute COVID-19 patients.4650 However, follow-up of physical function was not performed after discharge from the rehabilitation unit. Although the follow-up period was relatively short in our study, we investigated the effects of comprehensive inpatient rehabilitation after discharge.
In our study, cumulative time of inpatient rehabilitation, regardless of the site of the exercise program, was 1 hour per day at maximum, for 15.2 ± 14.6 days. Compared to the previous study on inpatient rehabilitation of survivors of severe COVID-19, performed at least 3 hours per day on weekdays for 16.7 ± 7.8 days, our study revealed comparable improvement despite the relatively short time of inpatient rehabilitation (BBS: 22.6 ± 18.5 at baseline, 43.7 ± 14.0 at discharge; gait speed: 0.25 ± 0.25 m/s at baseline, 0.86 ± 0.57 m/s at discharge in the study by Olezene et al.51). The lasting effect of comprehensive inpatient rehabilitation demonstrates the possibility of reducing the length of inpatient rehabilitation and hospital stay. Despite the long, acute care period in patients with severe-to-critical COVID-19, a relatively short period of comprehensive rehabilitation enabled patients to go back to premorbid lives.
COVID-19 survivors are at an increased risk of developing acute forms of sarcopenia, the underlying mechanism of which has been suggested in previous studies.525354 In this study, a comparison of body composition analysis between in-hospital and 1-month follow-up demonstrated a significant increase in the SMI. However, the change in body fat mass was not significant. These results correspond to the recovery from acute forms of sarcopenia in survivors of severe COVID-19.
Considering the effectiveness of intervention and limited healthcare resources, the dose of rehabilitation has been an important issue. However, to the best of our knowledge, no study investigated the dose-response relationship between rehabilitation and functional outcomes. Thus, we explored the dose-response relationship between rehabilitation and functional outcomes. During the period of inpatient rehabilitation, there were moderate correlations between the number of days of rehabilitation with the improvements in FAC and BBS. Although the short period of inpatient rehabilitation could not sufficiently improve muscle strength, a high dose of training did improve physical functional outcomes: it will contribute to a decrease in the length of hospital stay in the tertiary university hospital, eventually saving healthcare resources and costs and reducing the negative effect of prolonged hospital stay on patients.
In the correlation analysis between demographics, clinical information, and the change in outcome parameters, patients with higher cognition tended to show greater improvements in gait speed at discharge. By contrast, those with older age, longer hospitalization, longer ICU stay, longer duration of mechanical ventilation, and poorer nutritional status (represented by serum albumin) showed poorer improvements in gait speed at the 1-month follow-up. Patients with a more depressive mood according to PHQ-9 assessments at baseline exhibited poorer improvements in the number of repetitions in the 1-min sit-to-stand test and gait speed at the 1-month follow-up.
This study has several limitations. First, we did not include a control group, as it was considered unethical not to provide rehabilitation to COVID-19 survivors. Contemporary or historical controls were not available at this moment. Given the absence of a control group, the effects of rehabilitation cannot be strictly differentiated from natural recovery. Second, given our focus on the rehabilitation of patients with severe-to-critical COVID-19, the sample size was relatively small, limiting the generalization of the results. Further study with a larger sample size will provide more statistical power. Third, we could not initiate rehabilitation during the quarantine period (before negative conversion of COVID-19) due to concerns of cross-infection of the medical staff. However, a recent update on the isolation of COVID-19 states that the maximum period of isolation should be less than 20 days after symptom onset.55 Thus, earlier rehabilitation is expected to be provided to severe-to-critical inpatients. Fourth, many participants were lost to follow-up; therefore, all assessments could not be completed. Body composition analysis was not performed in some cases because of the limited mobility of most inpatients. Fifth, the definition of the rehabilitation dose based on the total number of days or total time spent on rehabilitation cannot perfectly reflect the true meaning of dose. It would be desirable to include the exercise intensity and contents of the individualized PT program and the patient’s compliance with rehabilitation, as well as the number of days of rehabilitation, the time spent on rehabilitation in the definition of the rehabilitation dose. Nevertheless, the former two were not included as they cannot be quantified. Finally, the follow-up period of one month was insufficient to predict long-term rehabilitation results; the present study focused on comprehensive rehabilitation management with a short-term outpatient follow-up in COVID-19 survivors, and studies with long-term follow-ups are being conducted. Further studies with long-term follow-up would provide more insights on the impact of rehabilitation in severe-to-critical COVID-19 cases.
This study revealed the effects of comprehensive rehabilitation management on the recovery of muscle strength and physical performance in patients with severe-to-critical COVID-19 in a tertiary hospital. The observed dose-response relationship of rehabilitation emphasizes the importance of intensive post-acute inpatient rehabilitation in COVID-19 survivors and provides insights into the allocation of medical resources in the COVID-19 pandemic. Further studies with multicenter prospective cohorts with the randomized control group, conducted over longer periods, will pave the way to mitigate the functional decline in critical COVID-19 cases.
Go to :
 XML Download
XML Download