

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Respiratory syncytial virus (RSV) and influenza virus (IFV) are two major respiratory viruses, particularly prevalent in late fall and winter in temperate countries.12 These globally widespread viruses are robust endemic viruses with high transmissibility through respiratory droplets and environmental contagiousness.3 High-risk populations such as infants, young children, and older people are at high risk of severe disease from these viral infections.14
Surprisingly, public health measures, namely nonpharmacological interventions (NPIs), implemented in many countries to mitigate the coronavirus disease 2019 (COVID-19) pandemic have resulted in drastic reductions in the prevalence of diseases caused by respiratory viruses during the 2020–2021 season in the Northern and Southern hemispheres.567 According to the national surveillance data from 14 countries/regions including European countries, the USA, Canada, Mexico, Costa Rica, Israel, Taiwan, and South Korea, the RSV (0.02%) and IFV (0.3%) positivity rates in September 2021–January 2022 were extremely lower than the rates in the pre-NPI period, at 15.1% and 6.4% of the pre-NPI period, respectively.8 These phenomena have had positive collateral effects in reducing the number of people with respiratory symptoms requiring COVID-19 screening, emergency room visits, and medical resources.910 Meanwhile, as the COVID-19 pandemic prolongs and with universal vaccination against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) introduced in many countries since December 2020, the intensity of the NPIs has been gradually reducing. As a consequence, there have been reports of re-emergence of RSV infections in several countries, especially in conjunction with the reopening of schools and daycare facilities.1112 However, in the case of influenza, as of February 2022, there have been few reports on re-emergence, and the reason behind the difference in the infection rates of RSV and IFV is unclear.13
In South Korea, the 2020–2021 winter was the first season in which the influenza season advisory was not issued since the 2000–2001 season, when the Korea Disease Control and Prevention Agency had issued the advisory for the first time in South Korea, and it was the first season when there was no endemic transmission of the RSV since the national respiratory virus surveillance was started in 2010.8 As of January 2022, South Korea was one of countries to ease the intensity of the domestic NPIs but still requiring the quarantining of overseas travelers/immigrants for 1–2 weeks or monitoring of their symptoms.14 This circumstance provides a good opportunity to observe the occurrence rates of RSV and IFV when domestic NPIs are alleviated while foreign inflow of these viruses is still blocked.
The primary purpose of this study was to examine whether the occurrence rates of RSV and IFV continued to decline in the 2021–2022 season, which was the second year of NPI implementation, compared to those in the pre-NPI period in South Korea. We also investigated the epidemics of other respiratory viral infections in the region and explored RSV and IFV occurrence rates in other countries since the COVID-19 pandemic.
METHODS
Data sources in South Korea
We used the Korean Influenza and Respiratory Virus Monitoring System (KINRESS) database, described in previous studies.78 Clinical surveillance data of inpatients with acute respiratory illness (ARI) from 192 participating institutions and specimen-based surveillance data of outpatients from 52 participating outpatient clinics were collected. The weekly numbers of tested samples and the number of positive samples for eight respiratory viruses (RSV, IFV, adenovirus, bocavirus, parainfluenza virus, rhinovirus, metapneumovirus, and coronavirus), confirmed by polymerase chain reaction (PCR), were collected. In case of clinical surveillance, the data of patients diagnosed by rapid antigen test (RSV and IFV only) were also included. These data and data on confirmed cases of COVID-19 in South Korea are available on the KDCA website (http://www.kdca.go.kr/npt/). To trace the intensity of domestic NPI measures, mobility trend data from February 15, 2020, to January 31, 2022, were obtained from Google’s Community Mobility Reports (https://www.google.com/covid19/mobility/). We also collected country-level (South Korea) information on the percentage change in visits to or time spent in transit stations and retail and recreational places and compared these data with baseline data for the corresponding day of the week, during the 5-week period of January 3–February 6, 2020.
Study design
This retrospective comparative study examined whether the number and positivity rates (%) of respiratory viral infections, including RSV and IFV infections, were still low in the KINRESS database in the second year of NPI implementation. The period from January 2016 to January 2020 was set as the pre-NPI period (pre-NPI period) and the period from February 2020 to January 2022, as the NPI period (NPI period). The autoregressive integrated moving average (ARIMA) model was used to predict the incidence in the NPI period using the incidence trends in the pre-NPI period. Additionally, we compared the observed incidence during the NPI period with the annual mean incidence during the same months (February–January) in the pre-NPI period. We also analyzed the data on other respiratory viruses contained in the KINRESS.
Data sources from other countries/regions
The surveillance data on RSV and IFV were collected from a total of 14 countries; the data of 13 countries were collected from the literature, and data of Slovenia were collected from a different source.8 The data were also collected from the regional offices of international organizations or infectious disease agencies of national health departments. The weekly positivity rates (%) for RSV and IFV from the specimens of patients with ARIs allowed for a comparative evaluation of time-series data of 40 weeks in 2019 and 5 weeks in 2022.
Statistical analysis
Seasonal ARIMA models were constructed to estimate the incidence during the NPI period. Optimal ARIMA models were determined in terms of the autocorrelation function, partial autocorrelation function, the Akaike information criterion, and residuals. Since sentinel surveillance is not based on population-based data, the parameters for incidence rates could not be estimated, so positive cases or positivity rates were used instead. The parameters were determined by comparing multiple candidate models in terms of residuals, autocorrelation coefficients, and Akaike information criterion. Mean absolute percentage error was calculated to examine the predictive accuracy of the ARIMA models. The relative risk was calculated using the Poisson regression model. All tests were two-tailed, and P value < 0.05 was considered statistically significant. Statistical analyses were performed using R v.4.0.3 (R Foundation for Statistical Computing, Vienna, Austria) and SAS v.9.4 (SAS Institute Inc., Cary, NC, USA).
Ethics statement
This research was ethically conducted in conformance with the guidelines of the World Medical Association and the Declaration of Helsinki. The Institutional Review Board in the Severance Hospital (No. 4-2021-1642) approved the study. Informed consent was waived due to the retrospective nature of the study.
RESULTS
Status of COVID-19 confirmed cases and personal mobility in South Korea
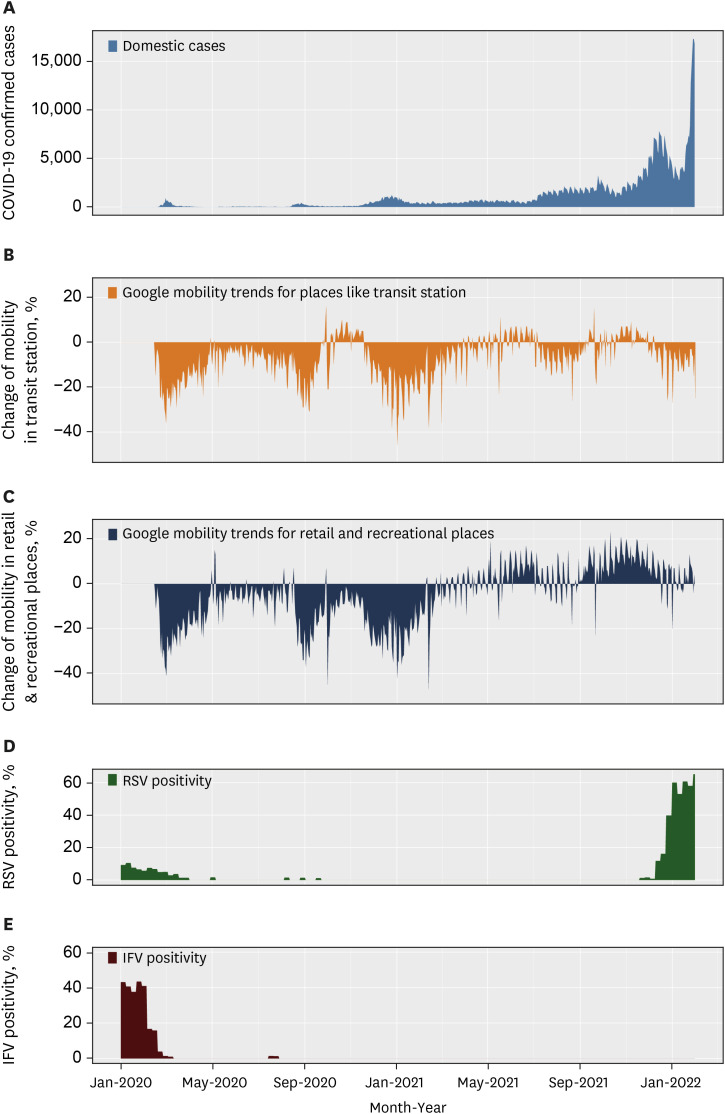
As of January 31, 2022, the cumulative number of confirmed domestic cases in South Korea was about 820,000 (Fig. 1). In February, August, and November of 2020, each epidemic wave had a daily maximum number of 1,000 confirmed cases, and the change in mobility decreased by more than 20% for each wave. Since June 2021, after the delta-variant coronavirus began to spread, the number of confirmed cases increased to thousands of cases per day, on average, but the change in mobility decreased compared to that in the previous epidemic wave or even exceeded the baseline value. In 2022, there were more than 10,000 confirmed cases per day as the omicron-variant coronavirus spread, but the mobility trends were similar to those during the delta-variant coronavirus dominant period.
Fig. 1
Trend of COVID-19 and individual mobility in South Korea. (A) Daily number of confirmed cases of COVID-19, (B, C) monthly individual movement estimation through mobile phones, (D) respiratory syncytial virus-positivity rate in the specimen-based surveillance, and (E) influenza virus-positivity rate in the specimen-based surveillance, January 2020–January 2022.
COVID-19 = coronavirus disease 2019, RSV = respiratory syncytial virus, IFV = influenza virus.
The baseline was the median value, for the corresponding day of the week, during the 5-week period from January 3, 2020, to February 6, 2020.
Characteristics of surveillance data in South Korea
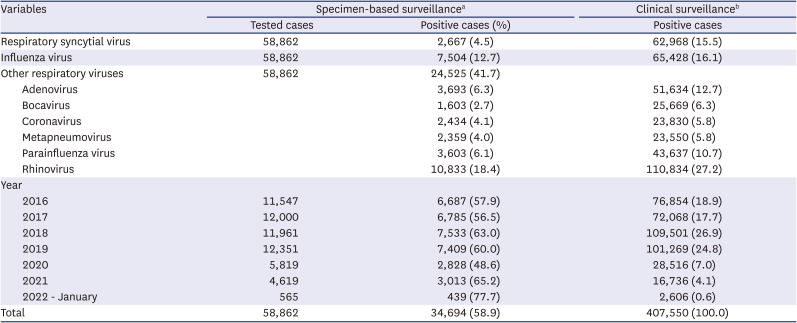
A total of 58,682 samples from outpatients under specimen-based surveillance and 407,550 samples from inpatients under clinical surveillance were collected. In the former dataset, the weekly mean numbers of collected samples were 230.6 (standard deviation [SD] ± 53.2) in the pre-NPI period, 90.1 (± 39.2) in the 2020–2021 season, and 94.7 (± 33.3) in the 2021–2022 season, respectively. The weekly mean numbers of hospitalized patients in the latter dataset were 1755.4 (± 843.5) in the pre-NPI period, 254.5 (± 282.0) in the 2020–2021 season, and 365.9 (± 234.0) in the 2021–2022 season, respectively. Other detailed characteristics are described in Table 1.
Table 1
Respiratory virus infection and positivity rates (%) from the Korean Influenza and Respiratory Virus Monitoring System, January 2016–January 2022
PCR = polymerase chain reaction.
aSpecimen-based surveillance data of outpatients from 52 participating outpatient clinics using PCR method; bClinical surveillance data of inpatients with acute respiratory illness from 192 participating institutions using PCR and rapid antigen test (respiratory syncytial virus and influenza virus only).
RSV and influenza epidemics in South Korea
From April 2020, when the broad NPIs for COVID-19 were implemented from February 2020 to early November 2021, there were no outbreaks of either RSV or IFV, with the exception of sporadic cases of RSV (Fig. 2). The RSV outbreak began to occur from the end of November 2021 and peaked in the third week of January 2022, with a weekly positivity rate of 61% under specimen-based surveillance (Fig. 2A). The overall weekly positivity rate of RSV in the 2021–2022 season (5.7%) was 1.5 times higher than that in the pre-NPI period (4.2%), at 1.8 times the predicted value (3.8%). Meanwhile, the rates of hospitalization for RSV infection in the 2021–2022 season were 16.7% (95% confidence interval [CI], 1.0–39.3%) of the pre-NPI period, at 17.6% (95% CI, 2.6–∞%) of the predicted value, but 35–48% higher than the rate in the 2020–2021 season, without statistical significance (Table 2).
Fig. 2
Weekly respiratory syncytial virus and influenza virus trends from Korean influenza and respiratory virus monitoring system, January 2016–January 2022. The solid lines denote the observed or predicted value. Light blue color denotes 95% confidence intervals of the predicted value and the dark blue, 80% confidence intervals of the predicted value. (A) RSV-positivity rates in the specimen-based surveillance, (B) RSV-related hospitalization cases in the clinical surveillance, (C) IFV-positivity rates in the specimen-based surveillance, and (D) IFV-related hospitalization cases in the clinical surveillance.
RSV = respiratory syncytial virus, IFV = influenza virus.
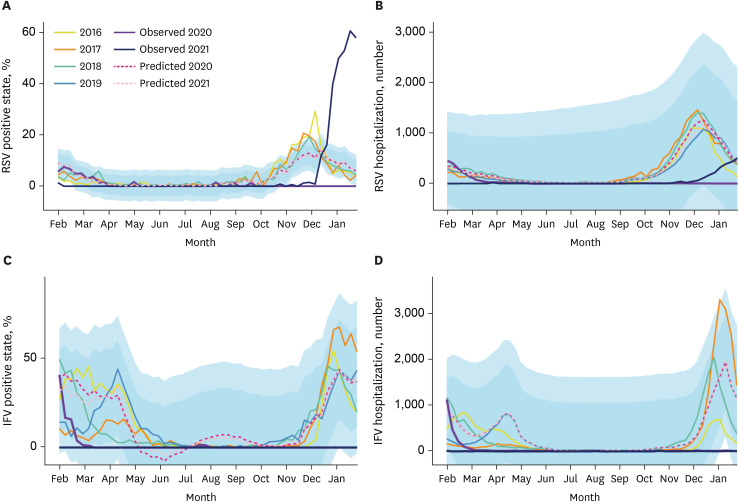
Table 2
Respiratory virus infections and positivity test rates (%) in the Korean Influenza and Respiratory Virus Monitoring System, January 2016–January 2022
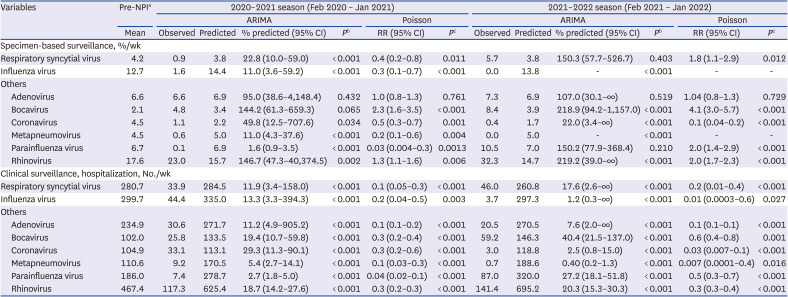
Weekly positivity rates or hospitalizations of respiratory infections from February 2016 to January 2022.
The positivity rates and hospitalizations were predicted by the ARIMA model and compared with mean values of the past 4 years (2016–2019).
NPI = nonpharmaceutical intervention, ARIMA = autoregressive integrated moving average, CI = confidence interval, RR = relative risk.
aIndicates the period from January 2016 to January 2020; bIndicates the statistical difference between the predicted mean and the observed mean; cIndicates the statistical difference between the NPI period and the pre-NPI period.
The weekly positive rates and number of hospitalizations for IFV infection were significantly lower in the NPI period than in the pre-NPI period for two consecutive seasons (i.e., 2020–2021 and 2021–2022) (Fig. 2C and D). In the 2021–2022 season, there was no positive cases of IFV among the 4,902 specimens under the specimen-based surveillance. In addition, the hospitalization rate for IFV under the clinical surveillance was extremely low at 1.3% (95% CI, 0.03–60.8%) of the pre-NPI period and 1.2% (95% CI, 0.3–∞%) of the predicted value (Table 2).
Other respiratory viral epidemics in South Korea
The data on six respiratory viruses (adenovirus, bocavirus, coronavirus, metapneumovirus parainfluenza virus, rhinovirus) were examined. The hospitalization rates for these viruses were statistically and significantly lower in the two consecutive seasons of 2020–2021 and 2021–2022 than in the pre-NPI period (Table 2). Moreover, in the specimen-based surveillance data, the weekly positivity rates for parainfluenza virus, metapneumovirus, and coronavirus were significantly lower in the NPI period than in the pre-NPI period and lower than the predicted value. However, the positivity rates for rhinovirus and bocavirus in the NPI period had significantly increased to 1.3–4.1 times those in the pre-NPI period and the positivity rate for parainfluenza virus in the 2021–2022 season was 2.0 times higher than that in the pre-NPI period (P < 0.001). Other data are described in Table 2.
Surveillance of RSV and IFV infections in other countries/regions
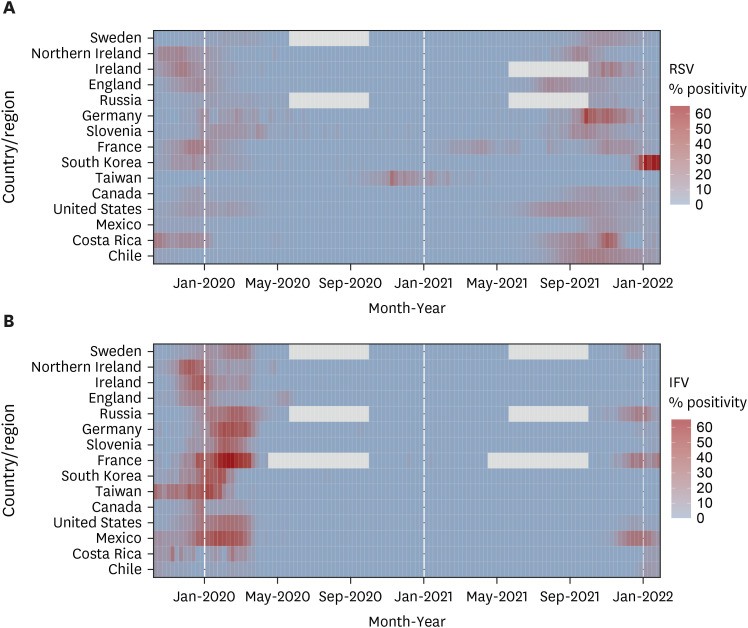
In the Northern hemisphere, endemic transmission of the RSV was observed in 13 countries, excluding Taiwan, during the 2019–2020 winter season (Fig. 3). Furthermore, a distinct influenza epidemic was observed in all countries, including Chile, in the Southern hemisphere. During the 2020–2021 winter season, the influenza epidemic was not observed in any of the countries, but endemic transmission of the RSV was reported in Taiwan (peak positive rate: 17.4%) and France (peak positive rate: 10.6%). In all countries except Taiwan, delayed endemic transmission of the RSV has been observed since the fall season of 2021; the peak positivity rates in Germany and South Korea were 48.0% and 61.0%, respectively, in the fall of 2021 and winter of 2022. Meanwhile, influenza (positivity ≥ 10% in at least 1 week) was reported in four countries (Sweden, Russia, France, and Mexico) in the 2021–2022 winter season.
Fig. 3
Heatmap of positivity rates in the national sentinel surveillance of 14 countries/regions. (A) Respiratory syncytial virus and (B) influenza virus.
RSV = respiratory syncytial virus, IFV = influenza virus.
Gray indicates absence of data: some countries did not operate surveillance systems during non-epidemic periods.
DISCUSSION
In this nationwide ecologic study, we found that there was no influenza outbreak in South Korea during the 2021–2022 season, the second winter season of the COVID-19 era. Meanwhile, endemic transmission of the RSV, delayed by 1–2 months, had emerged in the 2021–2022 season at half the magnitude of that reported in the pre-NPI period. This phenomenon suggests that in South Korea, the resurgence of RSV infections is possible as the domestic NPIs are eased. This also implies that overseas transmission of the IFV can be an important starting point for the annual seasonal influenza outbreak. Similarly, an RSV outbreak without influenza was observed in nine of the other 14 countries during the 2021–2022 season, whereas there were no outbreaks of RSV infection and influenza in all 15 countries with the exception of small-scale occurrences of RSV infection in Taiwan and France in the 2020–2021 season.
The disappearance of influenza outbreaks in South Korea for two consecutive seasons despite the gradual easing of the domestic NPIs means that the origin of annual seasonal influenza outbreaks in South Korea is not related to the extent of domestic NPIs, but to the quarantining of overseas travelers/immigrants. Unlike other respiratory viruses such as RSV, bocavirus and adenovirus, whose sporadic cases have been reported since COVID-19 pandemic, it is noteworthy that the number of influenza cases in the national sentinel surveillance was almost zero for 2 years in the COVID-19 era. Excluding clinical surveillance data containing rapid antigen test-confirmed cases with a risk of false-positive cases, only 2 out of 8,076 outpatients with ARI (30 weeks and 31 weeks in 2020, one case each) since April 2020 were IFV positive, as per PCR results. It is unlikely that the universal influenza vaccination for the general population had a significant effect on its disappearance because the effectiveness of the seasonal influenza vaccine is usually around 40–70%, and the vaccination rate of the general population is less than 50% in South Korea.15 Rather, considering that the RSV (basal reproduction number, R0 = 1.2–7.1) and IFV (R0 = 1.3–1.7) have similar modes of transmissibility, it is possible that the virus inflow from overseas during the seasonal influenza outbreak period in South Korea was blocked due to international travel restrictions.316 The incubation period (1–4 days) and the duration of viral shedding (5–10 days) of the IFV are relatively shorter than those of the SARS-CoV-2; therefore, IFV influx from other countries was theoretically interrupted due to the 1–2 weeks of self-quarantine and symptom monitoring of overseas travelers.17 Moreover, according to a report by International Air Transport Association, international air travel in 2021 was only 22% of the 2019 frequency, with the highest reduction in the Asia-Pacific region including South Korea (https://www.iata.org/en/pressroom/). Therefore, it is possible that the influx number of overseas travelers with influenza itself had decreased markedly. Monitoring how seasonal influenza occurs and spreads around the world as international travel restrictions are eased in the future may provide intriguing findings.1318
The rates of RSV infection in the 2021–2022 season suggest that the seasonal outbreak of RSV infection in South Korea may have started from an endemic source, and the exact origin is still unknown. Similarly, Taiwan and Australia also reported the occurrence of RSV infection without an influenza outbreak when the domestic NPIs were relaxed and overseas entry was strictly restricted.819 However, the scale of the endemic transmission of the RSV was about half of that in the pre-NPI period under the clinical surveillance system, and this scale was smaller than the simulated estimates reported in previous studies. In their epidemiological modeling study conducted in the United States, Baker et al.20 reported that the longer the NPI period, the greater the accumulation of infants and young children susceptible to RSV, so the endemic transmission of the RSV after the NPI period may be greater than that in previous seasons. In addition, according to a modeling study recently published by Zheng et al.,21 the hospitalization rates of infants and young children due to endemic transmission of the RSV could increase to about two times the existing rates. However, according to real-world data on the resurgence of RSV infection, including our study, the magnitude of RSV prevalence after NPI remission varied mostly between 0.5 and 1.5 times that in the pre-NPI period, which is lower than the modeling estimates (Supplementary Table 1). These data suggest that eased but remaining NPI measures such as wearing a mask, self-quarantine of symptomatic persons, telecommuting/online classes, and social awareness of personal hygiene and cough etiquette, etc., still play a role in preventing the spread of these infections. Therefore, it is necessary to continuously monitor how the scale of endemic transmission of the RSV changes as the NPIs are further relaxed or completely lifted in the future.22 In addition, it is important to continuously monitor the epidemiologic and genetic trend of RSV strains in each country, especially for the evaluation of current and targeted therapeutics and vaccines.23
It is interesting that the positivity rates of some respiratory viruses such as RSV, adenovirus, bocavirus, and rhinovirus in specimen-based surveillance were similar to or increased compared to those in the pre-NPI period although the number of hospitalizations due to all respiratory viruses decreased during the NPI period after February 2020 in the clinical surveillance. This may be because the index of specimen-based surveillance was the positivity rate (%), which refers to the number of cases in which the virus was detected among all samples collected, not the number of hospitalizations (as in clinical surveillance system). This means that if the total number of samples collected decreases and there is no minimal reduction in a given respiratory virus, the positivity rate for that virus may increase (Tables 1 and 2). Choe24 suggested that the transmissibility according to NPI measures such as hand hygiene and disinfection may vary depending on the intrinsic factors of each respiratory virus. For example, non-enveloped viruses such as rhinovirus and bocavirus can be more resistant to disinfection than other enveloped respiratory viruses.25 However, there is a limit to explaining the increase in the positivity rate, especially the increased positivity rates in the 2021–2022 season, of enveloped viruses such as the RSV and parainfluenza virus. Therefore, further studies are needed to identify additional specific intrinsic factors of respiratory viruses that influence their transmissibility.3
Our study has some limitations. First, this sentinel surveillance-based study did not aggregate the total number of RSV and IFV cases in South Korea. Therefore, our results do not represent the real incidence rates or trends of RSV and IFV infection epidemics. To offset this, we showed the consistency of data trends by analyzing both outpatient-based specimen surveillance and inpatient-based clinical surveillance data. Second, the specimen acquisition activity of national sentinel surveillance system could have been influenced by the COVID-19 pandemic. However, the positivity rate of some viruses, such as rhinovirus, parainfluenza virus, and bocavirus, were shown to be notably increased in line with to their prevalent season, suggesting that the surveillance system was well activated even during the NPI period. Third, other factors indirectly related to NPIs, such as healthcare-seeking behaviors, may have led to bias. Fourth, only countries that disclosed data on monitoring of both RSV- and influenza-positive rates during the COVID-19 pandemic period were included in the study. Therefore, countries that did not operate or update their national sentinel surveillance system during the COVID-19 pandemic were excluded from this study, so the results of this study do not represent the global trends in RSV and IFV infection epidemics. Finally, information on overseas quarantine regulations and domestic NPI levels by time period of the foreign countries included in the study were not collected.
Nevertheless, this study is of significance as, to our knowledge, this is the first nationwide study to report that IFV infection did not occur, but RSV infection was prevalent in the 2021–2022 winter in northern hemisphere in the COVID-19 era. Observing these epidemic patterns according to NPI intensity and international travel restrictions status can provide valuable information to prepare for the next pandemic and help public health authorities set priorities for prevention and proper quarantine.
 XML Download
XML Download