

 PDF
PDF Citation
Citation Print
Print



A 52-year-old female with acute severe chest pain radiation to upper back who had history of cardiac surgery for acute type A aortic dissection presented with recurrent type A aortic dissection around distal edge of previous surgical graft involving the ostium of the right innominate artery (IA) and left common carotid artery (LCCA) with multiple fenestrations. Based on the information from computerized tomography (CT) and invasive angiography, particular hole size of IA and LCCA and their vectors, directions, and accurate locations (Figure 1A) were decided, and the final customized stent-graft was generated (Figure 1B). 5F Pigtail catheter was inserted from left radial artery for angiography guided main body deployment. Main body Stent-graft 32×150 mm (IA hole 14 mm, LCCA hole 12 mm) was positioned with the guide of angiogram with pigtail catheter. (Figure 2A and B). Parallel wire into elbow and snaring was done into left radial artery (Figure 2B and C). After final deployment of main body, there was minimal angiographic endo-leak. CT angiography one week after stent graft implantation showed partial resolution of false lumen, thus we decided active sealing using customized branch graft (Figure 2D). One week after, via right femoral access with 18F sheath, customized IA branch graft 18×35 mm was deployed. After IA stent-graft implantation, final and 6-month CT angiography (Figure 3) showed dramatic sealing of previous endo-leak and patient’s symptom was completely disappeared. This is the first experience of customized 2 fenestrated stent-graft to preserve supra-aortic branches showing the feasibility of this technique to achieve endovascular total arch replacement in selective inoperable or high surgical risk patients.
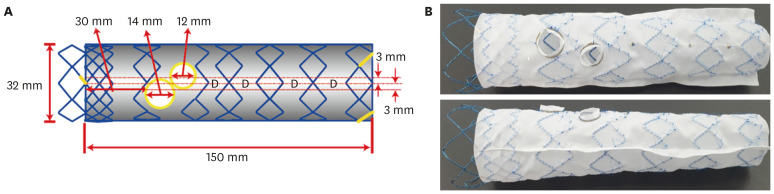 | Figure 1Design and real customized stent graft. (A) Schematic design according to 3D CT and invasive angiography. (B) Real stent-graft product model production.3D = 3-dimensional; CT = computerized tomography.
|
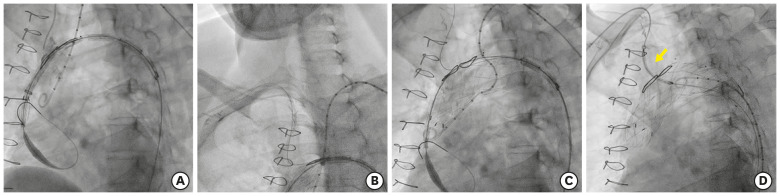 | Figure 2Main stent graft implantation procedure. (A) Sealing of aortic dissection by thoracic stent-graft 32×150 (Seal; S&G Inc., Yongin, Korea). (B) Innominate artery to right subclavian artery for snaring fenestrations (innominate artery & left common carotid artery). Five French MP-1 from right radial, 5 French Pigtail from left radial artery. (C) Main body deployment. (D) Innominate artery stentgraft implantation (yellow arrow).
|
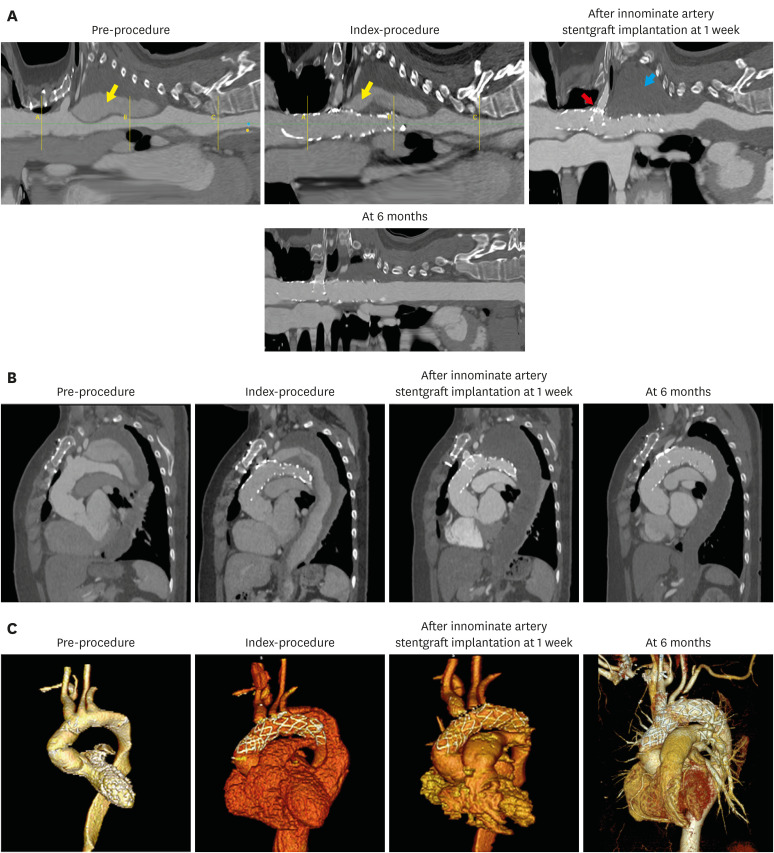 | Figure 3Serial follow-up CT showed resolution of endo-leak after stent-graft implantation. (A) Cross-sectional image. Yellow arrow: Contrast filling in false lumen, Blue arrow: Complete thrombus formation in false lumen, Red arrow: Branch stent-graft in fenestrated TEVAR. (B) Sagittal view. (C) 3D view image. Pre-procedure: Ascending aortic arch replacement status. Index-procedure: Fenestrated TEVAR with 2 fenestrae. After innominate artery stentgraft implantation at 1 week: Fenestrated TEVAR with innominate artery stent-graft.3D = 3-dimensional; CT = computerized tomography; TEVAR = thoracic endovascular aortic replacement.
|
We obtained written informed consent from the patient.
 XML Download
XML Download