

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Pulmonary valve replacement (PVR) is the most common operation performed in adults with congenital heart disease.1) Pulmonary regurgitation is the main indication for surgery in patients who have undergone previous right ventricular outflow tract (RVOT) reconstruction.1) A competent pulmonary valve has shown to relieve symptoms and preserve cardiac performance.1)2)
However, controversy still remains with regard to the best bioprosthesis in pulmonary position.1)2)3) The most commonly used xenografts are the porcine and bovine pericardial valves. There is evidence that bovine pericardial valves have a longer durability in aortic position, but this difference has not been showed in pulmonary position.3)
In this study we aim to compare the hemodynamic and clinical performance of Mosaic (Medtronic™; Medtronic Inc., Minneapolis, MN, USA) a porcine bioprosthesis against Carpentier Perimount Magna Ease (Edwards™; Edwards Lifesciences, Irvine, CA, USA) a bovine pericardial bioprosthesis in pulmonary position in patients with congenital heart disease.
METHODS
Ethical statement
Current guidelines of the Institution Ethics and Review Board for data protection were followed (IRB approval HULP: PI-5211), due to retrospective nature of the study informed consent was not warranted. All data collected arose from standard of care assessments.
Sample
This was a retrospective review of the medical records of all patients who underwent PVR from 1st January 1999 till 31st December 2019 at 2 congenital cardiac surgery reference centres. Study patients had either a Mosaic (Medtronic™; Medtronic Inc.) or a Carpentier Perimount Magna Ease (Edwards™; Edwards Lifesciences) bioprosthesis implanted in pulmonary position. Indications of PVR as well as preoperative image studies; such as echocardiography, cardiac magnetic resonance imagings and cath-lab data, were reviewed.
End points
Valve performance was evaluated using previously published criteria with a focus on echocardiographic follow-up to monitor hemodynamic valve function.4) The primary endpoints were freedom from reintervention (surgical or catheter based) and structural valve degeneration (SVD) with a peak transpulmonary gradient of >50 mm Hg and/or more than moderate pulmonary regurgitation.
Hospital mortality is defined as death in hospital or within 30 days of discharge. All other mortality is considered late.
Patients, families, cardiologists and primary care physicians were contacted when necessary to acquire current follow-up information.
Operative technique
Mosaic bioprosthesis were implanted in Hospital Universitario La Paz (Madrid, Spain), while Carpentier were the prosthesis of choice in Hospital Universitario Ramón y Cajal (Madrid, Spain). The same team of surgeons operated in both hospitals. Due to administrative reasons only one brand of bioprosthesis was available in each institution. Both institutions are tertiary level referral hospitals that give coverage to different geographic areas of the Spanish national territory.
PVR with or without tricuspid repair were performed with beating heart using bicaval cannulation and mild hypothermia (32–34ºC). Aortic cross-clamp was necessary for the repair of septal defects or left side valve surgery. Myocardial protection was done by cold single shot Celsior cardioplegia.
Either a failed right ventricle to pulmonary artery conduit, transannular patch or infundibular chamber was opened and residual patch material with native valve tissue was resected.5) The posterior one third of the stented valve annulus was sewn to native pulmonary valve annulus with continuous polypropylene suture or interrupted mattress sutures. Anteriorly, a diamond-shaped patch of Contegra™ (formerly Venpro, Medtronic Inc.) or bovine pericardium was used to roof the RVOT over the prosthesis.
Statistical analysis
A descriptive analysis of all the variables was performed. Quantitative variables with normal distribution are expressed as means±SD. Non-normally distributed variables are expressed as medians and interquartile range (IQR). Qualitative variables are reported as absolute values and percentages. Comparison of means was done either with t-student or U Mann-Whitney depending on the Kolmogorov-Smirnov test. Comparison of qualitative variables was done with Fisher’s test. Kaplan-Meier (KM) and Log-rank test were used to perform survival analysis. A proportional Cox hazard model was used to evaluate the relation between variables and events in follow-up. Statistical significance was considered when p<0.05.
Due to notable imbalances in baseline covariates between the study groups a propensity score (PS) matching system was used, with a nearest neighbour greedy algorithm.6)7) PS were calculated for each group using multivariate logistic regression according to the following clinical covariates: age, body surface area (BSA), size of the prosthesis, sex, base diagnosis, year of procedure and the presence of concomitant procedures.8)9)10) Common support was subjectively assessed by graphical examination of PS across both groups. Balance of PS across both groups was evaluated in quintiles. If it was not equivalent one or more quintiles were split into smaller blocks. Balance of covariates across both groups were evaluated within blocks of the PS. Balance of covariates after matching was checked comparing standardized differences. The KM curves, stratified log-rank tests and adjusted Cox regression analyses were all then run on the PS matched sample.
Matched subjects have a similar value of PS, thus have a similar distribution of observed baseline covariates. Because baseline covariates are related to outcome, matched subjects are likely to display a greater similarity in outcome compared with 2 randomly selected subjects. When outcomes are time-to-event in nature, KM survival curves can be estimated for treated and untreated subjects in the PS matched sample.7) The KM curve calculates the survival rate each time the event of interest occurs rather than at preset follow-up intervals as in actuarial life tables. KM analysis is thus event dependent and not duration dependent.11)
All analysis and graphical representations were done with STATA version 14.2 (Satacorp LP, College Station, TX, USA).
RESULTS
Overall sample
The study included a total of 319 patients with 337 PVR by a bioprosthesis. One hundred and ninty-nine prosthesis were porcine Mosaic (Medtronic™; Medtronic Inc.) and 138 were bovine Carpentier Perimount Magna Ease (Edwards™; Edwards Lifesciences). Due to difficulty for homograft procurement in Spain,12) this treatment option was seldom used with few anecdotal cases which are not considered for this study. Baseline information on diagnosis and concomitant procedures are given in Table 1. The evolution of PVR and case mix is given in Supplementary Table 1 and Supplementary Figure 1. Median follow-up duration was 3.27 years (IQR, 0.96–6.64) for porcine prosthesis and 5.92 years (IQR, 2.7–8.87) for the bovine group (rank-sum p<0.01). The median age in the porcine group was 33.2 years whereas in the bovine group it was 26.7 years (p<0.01). The median weight in the porcine group was 63.5 kg compared to 64.0 kg in the bovine group. Fifty-five patients (39.9%) were males in the porcine group and 99 (49.7%) in the bovine group. The median prosthesis size was 27.1 mm (SD, 1.81) for the porcine group and 26.8mm (SD, 1.99) for the bovine group (p=0.079).
Table 1
Covariate distribution by prosthesis type
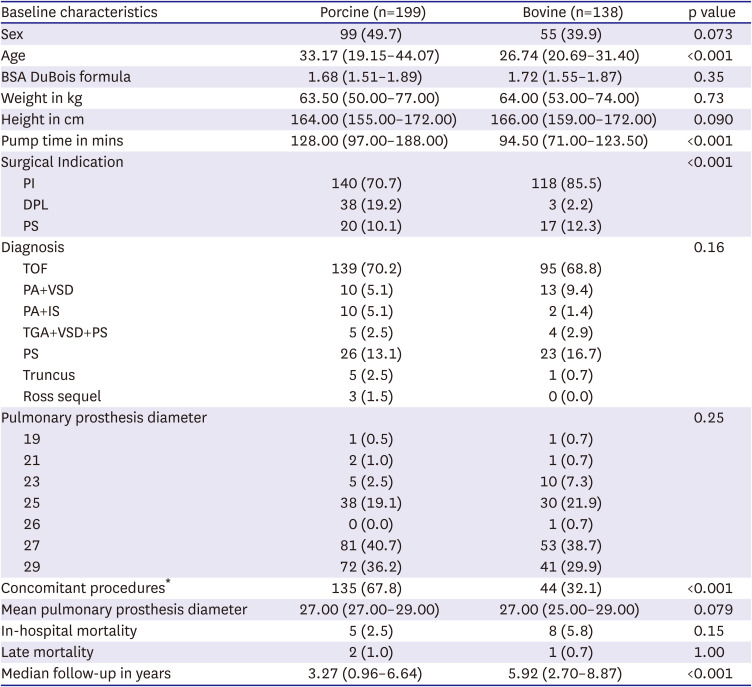
Data are shown as mean±SD or number (%).
BSA = body surface area; DPL = double pulmonary lesion; PA+IS = pulmonary atresia with intact septum; PA+VSD = pulmonary atresia with ventricular septal defect; PS = pulmonary stenosis; PI = pulmonary insufficiency; TOF = tetralogy of fallot; TGA+VSD+PS = transposition of great arteries with ventricular septal defect and pulmonary stenosis; Truncus = truncus arteriosus.
*A detailed description of the concomitant procedures is available in the Supplementary Table 2.
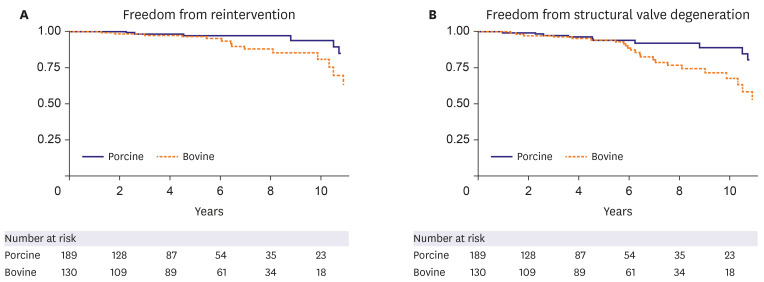
In hospital mortality of the global cohort was of 2.5% (n=5) in the porcine group and 5.8%(n=8) in the bovine group, no statistical significance. Five patients in the porcine group were lost to follow-up because they had moved abroad, none in the bovine group. Late mortality was of 3 patients, 2 in the porcine group and one in the bovine group. Freedom from reintervention for patients who received a porcine bioprosthesis (n=189) was 98.3%, 96.1%, and 93.6% at 3, 5, and 10 years and for patients who received a bovine bioprosthesis (n=130) was 98.3%, 96.1%, and 80.9% at 3, 5, and 10 years, retrospectively (χ2=5.48; Log-rank p=0.02). Freedom from SVD for patients with a porcine bioprosthesis was 97.6%, 94.1%, and 89.1% at 3, 5, and 10 years and for patients with bovine bioprosthesis was 97.5%, 94.3%, and 68% at 3, 5, and 10 years, respectively (χ2=9.74; Log-rank p<0.01).
Figure 1A and B show the KM curves for reintervention and SVD for the full sample. For both outcomes, worse performance was noted in the bovine group, which was confirmed by log-rank test (reintervention p=0.02; SVD p=0.002). However, the KM curves indicate a similar performance among both groups until 5 years of follow-up postimplantation. This was confirmed by converging slopes of the residuals for both outcomes, despite the fact that proportional hazards assumption was not violated. We therefore included a time interaction in the Cox regression. Time was split into 2 periods (t ≤5 years and t >5 years) with separate hazard ratio (HR) estimation in each duration. The interactions were significant for both outcomes (reintervention p=0.019; SVD p=0.005). This indicated that in the first 5 years there was no statistical difference in outcomes (HR, 2.11 [0.47–9.50]; p=0.33 and SVD HR, 1.61 [0.52–5.05]; p=0.41). Whereas, after 5 years recipients of bovine bioprosthesis were at higher risk of both outcomes (reintervention HR, 4.68 [1.29–17.0]; p=0.019 and SVD HR, 6.48 [2.17–19.33]; p=0.01). After accounting for time interaction, we found no evidence of non-proportional hazards.
Propensity-matched analysis
PS matching resulted in a total of 79 pairs of patients (79 porcine and 79 bovine bioprosthesis, n=158). Table 2 shows the covariate imbalance by bioprosthesis among 79 matched patients. Some imbalance was detected in age and year of procedure as the standardized differences exceeded 0.10.
Table 2
Covariate imbalance by prosthesis type

In hospital mortality of the PS cohort was of 3% (n=2) in the porcine group and 6% (n=5) in the bovine group, no statistical significance. Freedom from reintervention for patients who received a porcine bioprosthesis (n=79) was 98.3%, 96.1%, and 91.9% at 3, 5, and 10 years and for patients who received a bovine bioprosthesis (n=79) was and 100%, 98%, and 90.8% at 3, 5, and 10 years, retrospectively (χ2=0.02; Log-rank p=0.88). Freedom from SVD for patients with a porcine bioprosthesis was 96.9%, 92.8%, and 88.7% at 3, 5, and 10 years and for patients with bovine bioprosthesis was 100%, 98%, and 79.1% at 3, 5, and 10 years, respectively (χ2=0.77; Log-rank p=0.38). Figure 2A and B show the KM curves for reintervention and SVD for the PS sample, no difference was found for both outcomes.
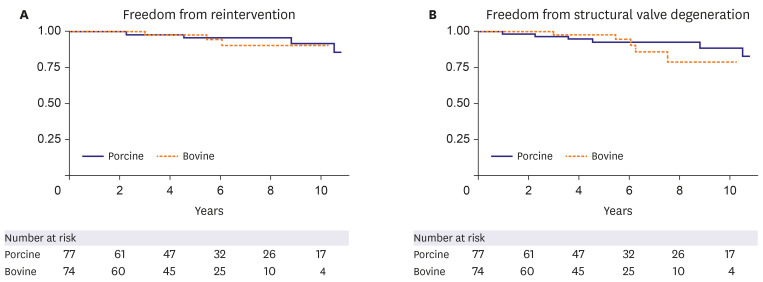
Bovine prosthesis was associated with a reintervention HR, 1.12; 95% confidence intervals, (0.24–5.26); p=0.89 and SVD HR, 1.69 (0.52–5.58); p=0.38. Time was split in 2 periods (t ≤5 years and t >5 years) with separate HR estimation in each duration. During the first 5 years there was no difference in outcomes (reintervention HR, 0.52 [0.05–5.75]; p=0.59 and SVD HR, 0.27 [0.03–2.41]; p=0.24). Whereas after 5 years recipients of bovine bioprosthesis remained at higher risk of SVD but not reintervention (reintervention HR, 2.08 [0.27–16.0]; p=0.49 and SVD HR, 6.99 [1.23–39.8]; p=0.03). After accounting for time interaction, we found no evidence of non-proportional hazards.
DISCUSSION
There is enough accumulated evidence to accept the superiority of bovine pericardial valves in aortic position.13)14) In vitro studies show different performance of bovine valves under left and right sided pressures. Hence left sided hemodynamic performance of these valves can not be extrapolated to the right side, low pressure, chambers.8)15) It is this change in performance which casts doubts of the superior nature of the bovine bioprosthesis in pulmonary position.
Bioprosthesis in pulmonary position is an off-label indication and thus a different scenario. Here the long term data is scarce, with limited reports of over 10 year follow-up.16)17) Comparisons between bioprosthesis is further hindered by confounding factors.18) Studies include different timings or “eras” of operation,18) different ages19) and different valve sizes.20) Some factors are difficult to account for such as immunological factors21) and operative complexity.22) In order, to make more robust comparisons we used a PS adjusting for age, BSA, size of the prosthesis, sex, base diagnosis, year of procedure and presence of concomitant procedures.
As calculated by Pragt et al.,17) overall our results fared better than the median freedom from reintervetion reported in the literature: 95.2±15.98% (range, 50–98.2%) for 5 year follow-up and 81.2% (66.4–84.7%) for 10 year follow-up. One has to take into account that these studies have a younger age cohort which itself is a risk factor for valve failure. Nomoto et al.,23) who included a slightly older population (median, 17.5 years) describe better results of freedom of reintervention of 96.7% at 5 and 10 years of follow-up.
Neither the definition nor the echocardiographic follow-up has been uniform between studies. The choice to include moderate regurgitation and/or moderate stenosis as definition for valve failure is arbitrary.16) There is much debate regarding the best timing for reintervention of malfunctioning pulmonary valve as these are well tolerated.1)3)16)18) Hence, indication for valve reintervention is not solely indicated by the severity of valve malfunction. Our results show a low rate of valve failure: at 10 years of follow-up, 10.9% for porcine and 32% for bovine bioprosthesis. Comparisons with other studies is complicated due to age and valve failure definition confounders.
Although in our study none of the explanted valves were histologically examined, there are reports which identify deterioration patterns of bovine and porcine bioprosthesis.17) Bovine bioprosthesis have a tendency to cusp stiffening with calcium deposits, whereas, porcine bioprosthesis have a tendency to cusp tearing. These findings have been described when the bioprosthesis are implanted in left side positions. In the right side, pulmonary pressure is lower than systemic pressures even in patients with pulmonary atresia and major aortopulmonary collateral arteries.15)16)24) This rarely has been the cause of acute deterioration of the bioprosthetic valve structure, which could explain the better performance of porcine bioprosthesis.
Our study included a number of limitations due to its retrospective nature. To improve the internal validity of our analysis a robust PS was used to compare both prosthesis. There may be other potential confounders not accounted for in the PS. Our study population was from 2 different centres with echocardiographic evaluations performed by 2 different teams of cardiologists using different machines, this could have introduced bias. Finally, our data included small number of patients beyond 5 years of follow-up especially in the porcine group, thus comparisons of survival beyond this point should be interpreted with caution.
In conclusions, bovine and porcine bioprosthesis have similar outcomes up to 5 years after implantation in pulmonary position. After 5 years, there was no difference in the rate of reintervention, however, porcine bioprosthesis seem to to have less SVD.
 XML Download
XML Download