

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Atrial fibrillation (AF) is one of the most notable and common cardiac arrhythmias1)2)3) associated with a higher incidence of stroke.3)4) AF shows biological sex-based differences in pathophysiology, epidemiology, presentation, and prognosis.5) For several decades, Vitamin K antagonist (VKA) has been the preferred oral anticoagulants (OACs) for patients with AF, reducing all-cause death (26%) and stroke (64%) risks. Overall, women have an elevated risk of stroke, mortality, and cardiac events than men.6)7) Several studies have reported that females taking VKA are still at higher risk of stroke or systemic embolism (SSE).8)9) One of the possible reasons was that there was a significant biological sex-based difference in the proportion of patients with AF who use anticoagulants. Lower anticoagulation rate of women might be due to a higher concern of increased bleeding risk in women, especially in old age.7)
In multiple major randomized controlled trials, direct oral anticoagulants (DOACs) are safer than VKA, with a low incidence of intracranial hemorrhage.10)11) Moreover, DOACs have several additional advantages over VKA; these include lower frequency of monitoring the routine coagulation status and fewer drug-drug interactions.12) Current guidelines propose that it is preferable to use DOACs in patients with non-valvular atrial fibrillation (NVAF) at risk of stroke or systemic thromboembolism.3)13)14) In contemporary AF cohorts, the use of DOACs is more prevalent than that of VKA.
Patients who have a low risk of stroke are not recommended OACs, whereas patients with a higher stroke risk benefit from antithrombotic therapy.3)13) There is a lack of large contemporary cohort-based data comparing anticoagulant usage patterns and outcomes between both sexes. This study evaluated the relationship between biological sex and adverse clinical events in a contemporary AF patient cohort, those mainly taking DOACs, with intermediate to high risk of stroke (CHA2DS2-VASc score ≥1 for men and ≥2 for women).
METHODS
Ethical statement
Patients provided informed consent before participation, and the study received approval from the ethics committee of each center. This research was registered on ClinicalTrials.gov (NCT02786095) and approved by the Institutional Review Board of the Yonsei University Health System (4-2016-0105).
A previous report has described the research design of the comparison study of drugs for symptom control and complication prevention of atrial fibrillation (CODE-AF).15) The CODE-AF registry is a prospective, multi-center study of patients with AF over 18 years old, conducted at 18 tertiary centers across the Korea.15) Eligible patients were recruited from June 2016 to May 2019.
The primary goal of the CODE-AF registry was to evaluate the outcomes of medical therapy for AF, including anticoagulation and rate or rhythm control.15) The secondary aim was to understand the epidemiology and diagnostic flow of AF as well as clinical management.15) The Korea Heart Rhythm Society organized this CODE-AF registry.15) To minimize inconsistencies or errors, we obtained data from a commonly used electronic database.15)
From June 2016 to May 2021, 12,232 patients with NVAF aged >18 years were enrolled in the registry. The patients were excluded with more than a moderate grade of mitral stenosis and those with a history of valve surgery because VKA is required in such patients. Furthermore, patients with a history of cancer, pulmonary embolism, or deep vein thrombosis were excluded. Patients with missing data on usage of VKA or DOAC (n=47) and those who transitioned from VKA to DOAC or vice versa (n=203) were excluded from the 12,232 enrolled patients. Patients with missing follow-up data were also excluded (n=1,523). After exclusion, 9,476 patients were included. Stroke risk was assessed and the patients were grouped according to the CHA2DS2-VA score (sex-independent thromboembolism risk). Each component of the CHA2DS2-VA score was defined as C = congestive heart failure (1 point); H: hypertension (1 point); A: age ≥75 years (2 points); D: diabetes mellitus (1 point); S: stroke or TIA (2 points); V: vascular disease (1 point); and A: age 65–74 years (1 point). The patients with more than an intermediate risk of stroke (CHA2DS2-VA score ≥1) with taking anticoagulation therapy (n=6,067, mean age 70±9 years, men 59%) were finally analyzed. The patients were stratified based on their biological sex. The data on adverse clinical events, such as SSE, major or minor bleeding, and all-cause death in these patients were obtained. Every 6 months, all patients were scheduled for outpatient clinic interviews or telephone consultations.
The primary endpoint of this study was SSE occurrence during the period of follow-up. The safety endpoint was the incidence of major bleeding. The other clinical endpoints comprised all-cause death and minor bleeding during the period of follow-up. Stroke was defined as a neurological deficit due to a cerebrovascular cause, persisting for over 24 hours, confirmed the diagnosis of ischemic stroke due to thrombosis or embolism with computed tomography or magnetic resonance imaging.16) Systemic embolism (SE) was defined as a acute loss of perfusion of a vessel supplying an extremity or end-organ. It was diagnosed using various imaging modalities, including computed tomography or ultrasonography.16)
All normally distributed continuous variables were expressed in mean ± standard deviation and compared using Student’s t-test. For variables with a skewed distribution, medians with interquartile ranges and the Mann–Whitney U-test was used. Categorical variables were expressed in numbers (percentages) and compared using the χ2 test and Fisher’s exact test. We conducted a multivariable cox regression analysis of the outcome of interest to identify factors associated with sex-based differences. Clinical variables were selected based on previous studies and experiences.10) The results are expressed in hazard ratio (HR) and 95% confidence intervals (CI). All p values were two-sided, and values below 0.05 were considered statistically significant. We performed all statistical analyses using SPSS software (v.25.0; IBM Corp., Armonk, NY, USA).
RESULTS
Sex differences in intermediate to high risk of stroke
Table 1 describes the patients’ baseline characteristics. Compared to men, women were older (71.9±8.5 vs. 68.3±9.7 years, p<0.001). The CHA2DS2-VA score did not differ between women and men. Men had a higher incidence of diabetes, myocardial infarction, and peripheral arterial occlusive disease than women. In women, interventions for control of cardiac rhythms, such as catheter ablation (9.7% vs. 14.5%, p<0.001) and cardioversion (10.7% vs. 17.5%, p<0.001) were less frequently performed than in men. Analysis of antiarrhythmic drugs revealed that amiodarone (8.6% vs. 13.9%, p<0.001) was used significantly in a lower proportion of women than in men.
Table 1
Baseline characteristics of patients according to sex in intermediate-to-high-risk group of stroke
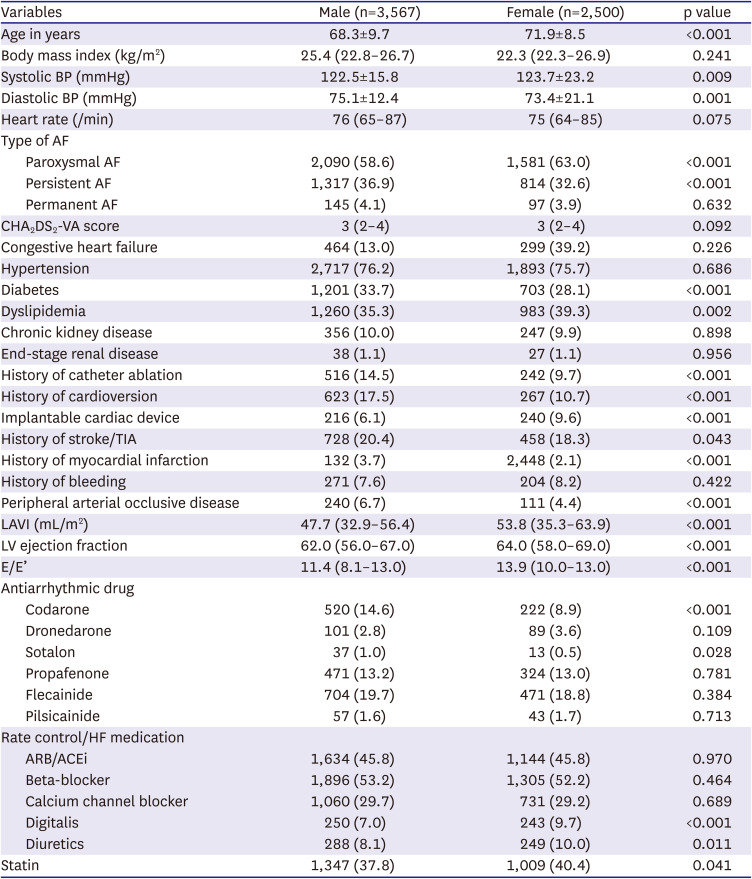
Values are presented as mean ± standard deviation for normally distributed variables, median (IQR) for non-normally distributed variables, or number (%).
ACEi = angiotensin converting enzyme inhibitor; AF = atrial fibrillation; ARB = angiotensin II receptor blocker; BP = bood pressure; HF = heart failure; LAVI = left atrial volume index; LV = left ventricle; TIA = transient ischemic attack.
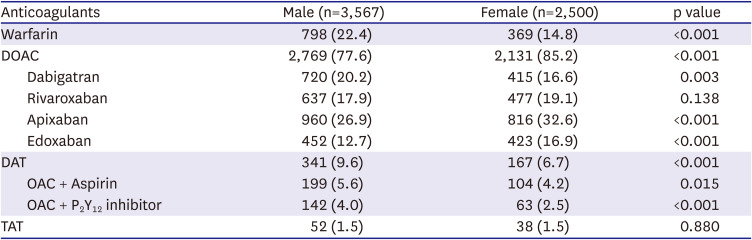
Table 2 describes the usage pattern of OACs. VKA was prescribed to a higher proportion of men than to women (22.4% vs. 14.8%, p<0.001). However, DOACs were more frequently prescribed to women than to men (85.2% vs. 77.6%, p<0.001). In the individual analysis of DOACs, apixaban and edoxaban were prescribed to a higher proportion of women. Dual antithrombotic agents (DAT; OAC + P2Y12 inhibitor or aspirin) was less frequently prescribed to women (6.7% vs. 9.6%, p<0.001); however, the prescription frequency of triple antithrombotic agents (TAT; OAC+ P2Y12 inhibitor + aspirin) did not differ between men and women.
Table 2
Comparison of anticoagulation status between men and women in the intermediate-to-high-risk group of stroke
During a median (25th, 75th percentiles) follow-up of 30 months (24, 38), women and men experienced 41 and 61 SSE events, respectively, with annualized rates of 0.7 and 0.7 per 100 person-years (Table 3). Women and men experienced 7 and 14 major bleeding events, respectively, with annualized rates of 0.1 and 0.2 per 100 person-years (p=0.60). The cumulative incidence rates of SSE (p=0.89, Figure 1A) and major bleeding (p=0.46, Figure 1B) did not differ between the sexes. The adjusted risks of SSE or major bleeding were the same for both sexes (Table 3).
Table 3
Incidence rates and adjusted hazard ratios of all-cause death and other clinical events according to sex in the intermediate-to-high-risk group of stroke
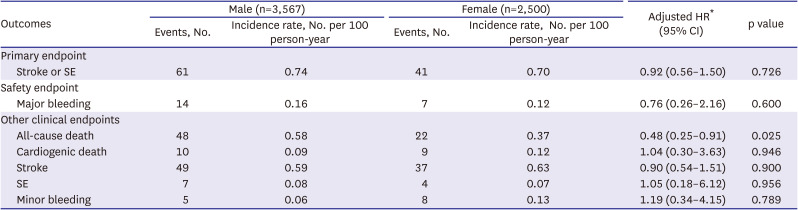
AF = atrial fibrillation; CI = confidence interval; EF = ejection fraction; HF = heart failure; HR = hazard ratio; LAVI = left atrial volume index; PAOD = peripheral artery occlusive disease; SE = systemic embolism.
*Adjusted for age, blood pressure, type of AF, diabetes, dyslipidemia, prior myocardial infarction, PAOD, prior implantable cardiac device, history of catheter ablation, history of cardioversion, statin use, HF medications, antiarrythmic drugs, LAVI, EF, and E/e’.
Figure 1
Cumulative incidence of stroke or systemic embolism (A), major bleeding (B), and all-cause death (C).
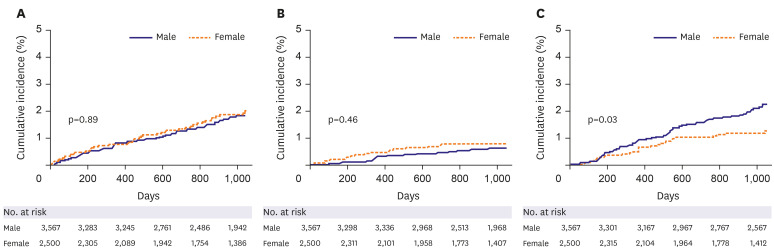
Among individual outcomes, women exhibited a significantly lower incidence rate and risk of all-cause death than men (0.37 vs. 0.58 per 100 person-years, adjusted HR, 0.48; 95% CI, 0.25–0.91; p=0.025) when adjusting for confounding clinical variables. However, cardiovascular death rates did not differ between women and men (Table 3). The cumulative incidence of all-cause death was also lower in women than in men significantly (p=0.03, Figure 1C). The occurrences and risks of stroke, SE, and minor bleeding did not differ across sexes (Table 3).
When analyzed the differences in the occurrence of clinical events between men and women by dividing into DOAC group and the VKA group, women showed lower risk of all-cause death than men (0.29 vs. 0.47 per 100 person years, adjusted HR, 0.43; 95% CI, 0.20–0.94; p=0.045) in DOAC group (Supplementary Table 1). However, in the VKA group, there was no significant difference between men and women in any clinical events including all-cause of death (Supplementary Table 2).
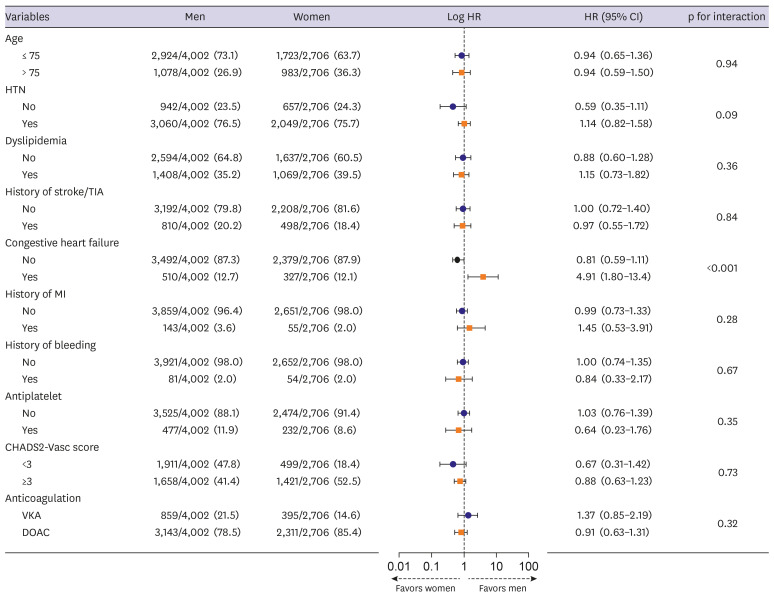
In a subgroup analysis after adjusting the confounding clinical factors for SSE occurrence, patients with a history of previous heart failure exhibited significantly higher HR among women (HR, 4.91; CI, 1.80–13.4; p for interaction: <0.001). In other subgroups, including the type of anticoagulant used, there were not any significant sex-based differences in SSE occurrence (Figure 2).
Figure 2
Forest plot representation of clinical factors including anticoagulation associated with the primary endpoint (stroke or systemic embolism).
CI = confidence interval; DOAC = direct oral anticoagulant; HR = hazard ratio; HTN = hypertension; MI = myocardial infarction; TIA = transient ischemic attack; VKA = vitamin K antagonist.
Sex differences in all patients
Supplementary Tables 3 and 4 provide the baseline characteristics and anticoagulation status of patients in the all patients in CODE-AF registry. Similar to those in the intermediate to high-risk group, the proportion of men who used VKA was higher than that of women (15.0% vs. 12.1%, p<0.001), while the proportion of women who used DOACs was higher than that of men (64.3% vs. 48.8%) in the all patients in CODE-AF registry. Women used all DOACs more frequently than men, except dabigatran. In the analysis of DAT and TAT, the use of DAT was lower in women compared to men (5.0% vs. 5.8%, p<0.001) and TAT did not differ between sexes.
In the all risk of stroke groups, the adjusted risk of SSE was not different between women and men (1.3 vs. 0.7 per 100 person-years, adjusted HR, 0.70; 95% CI, 0.44–1.10; p=0.123). However, the adjusted risk of all-cause death in women was lower than in men (0.4 vs. 0.4 per 100 person-years, adjusted HR, 0.53; 95% CI, 0.30–0.96; p=0.034). Other individual outcomes such as cardiovascular death, stroke, SE or bleeding did not show any difference (Supplementary Table 5).
DISCUSSION
The main findings in our multicenter-prospective study are as follows; 1) In the contemporary AF cohort with anticoagulation therapy using DOACs (81%) and VKA (19%), women with intermediate to high risk of stroke were older, but there was no difference of stroke risk based on CHADS2-VA score between the sexes. 2) SSE, as a primary endpoint and major bleeding, as a safety endpoint did not differ between the sexes. 3) Women had a lower adjusted all-cause mortality rate than men but there was no difference in cardiovascular death rate.
Among the possible sex-based differences in the contemporary use of mainly DOACs, and relatively small number of VKA with concomitant antiplatelet therapy in AF, the biggest concern is whether women still have more increased risk of mortality and cardiovascular events than men.6) Women with AF treated with VKA had a higher risk of SSE than men.8)9) It was probably due to women’s tendency to spend less time in the therapeutic range of VKA.17)18) Moreover, AF is diagnosed and treated at a relatively old age in women,19) and multi-morbidity was prevalent in old age patients despite of anticoagulation therapy.20) However, with more DOAC treatment, SSE rates were known to be comparable between women and men. Furthermore, women exhibited a significantly lower major bleeding risk with the preferred use of DOACs over VKA than with the use of VKA only.10)11)21) Previous studies on biological sex-based differences in adverse clinical outcomes related to AF revealed minor heterogeneity. Although several studies have compared the effect of VKA and DOACs, nothing is known regarding the effect of sex on clinical outcomes, such as current anticoagulation patterns in a contemporary AF patient cohort using DOACs. It might be meaningful that our study shows that women no longer have a higher stroke risk compared to men in contemporary cohort mainly using DOACs.
DOACs are safer than VKA showing decreased risk of intracranial hemorrhage.10)11) The proportion of patients who use VKA has steadily decreased with the introduction of DOACs.22) At the end of 2018, there was a trend of increase in the usage of DOACs, with more than 60% of all patients on anticoagulants using DOACs.23) In a recent study based on the data from the CODE-AF registry 2018, among patients with an intermediate to high risk of stroke, women were taking anticoagulants at higher rates compared with men, and the use of DOACs was more prevalent in women.19) This is consistent with the findings of this study. According to our study, when divided into DOAC treatment group and VKA treatment group, it was found that the primary endpoint was not different between sexes in both of the DOAC and VKA groups. Women’s all cause of death risk was significantly lower than men’s in DOAC group but not in VKA group. Therefore, it was thought that the decrease in the adverse clinical outcomes among women receiving anticoagulation therapy in AF might be related to the favorable outcome of contemporary treatment mainly using DOACs.
It is relatively common to treat patients with AF with DAT or TAT. Following the recent guidelines, patients with AF who underwent percutaneous coronary intervention were recommended TAT in the short-term, DAT for one year, and then single OAC after percutaneous coronary intervention.3)24) Previous studies revealed that patients with DAT or TAT in AF experienced high major bleeding than those with warfarin single therapy.25)26) Our study showed men had a higher usage of DAT in patients with intermediate to high risk of stroke. However, men did not show a higher bleeding risk than women.
There are limitations to this study. This is a transverse observational study. Medication use, including anticoagulants, was mostly studied using prescription data completed within the first few months after enrollment; thus, long-term medication compliance is a concern. Moreover, Korean patients were only included in this study, and the results cannot be generalized to other populations. This study is inevitable of referral bias because all patients were recruited from the tertiary centers alone, and patient data before referral was unknown. Finally, the incidence rate of clinical outcomes of this study was much lower than in previous studies.27) There are several possible reasons; First, our study included only patients with intermediate to high risk of stroke who received anticoagulation therapy so that stroke events or stroke-related mortality could be quite lower compared to other studies including both non-anticoagulated and anticoagulated patients. Second, there was a trend that clinical adverse outcomes of AF decreased continuously,1) and our study may also reflect this trend like other latest studies of AF. As shown in recent AF cohort, it seems that risk of stroke is low for the high usage of OACs therapy. The Global Anticoagulant Registry in the FIELD-Atrial Fibrillation (GARFIELD-AF) showed low SSE rate (1.2%) with high frequency of OACs therapy (60.8%).28) GLORIA-AF trial showed considerably low from 0.60 to 0.82 with high usage of OACs (79.7%).29) Finally, treatment with DOACs was typically known to reduce the bleeding risk. Our study included a contemporary AF cohort that used a higher proportion of DOACs (79% in men, 85% in women), which may reflect well the advantage of DOACs.
Conclusively, in a contemporary AF cohort using DOACs in 81% of patients who were at intermediate to high risk of stroke, women were older and showed a higher risk of stroke compared to men. However, the incidence and risk of SSE did not differ between the sexes. Additionally, women exhibited a lower incidence and risk of all-cause mortality than men, significantly. Considering that women use DOACs more than men, the use of DOACs for managing AF does not appear to be a risk factor for adverse clinical events in females.
 XML Download
XML Download