

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The prevalence of heart failure (HF) is expected to increase by 46% from 2012 to 2030, and the number of patients suffering from HF will exceed >8 million people in 2030 in the United States.1) Acute HF (AHF) is characterized by the heart's inability to expel and/or adapt blood flow within physiological pressure levels and is a severe decompensated condition in which symptoms and signs of HF appear rapidly or slowly, and patients seek urgent medical attention.2) HF is a leading cause of hospitalization for subjects aged >65 years.2) Additionally, HF is associated with high mortality rates, frequent rehospitalization due to HF and all causes,1)3)4) physical dysfunction, and impairment of activities of daily living (ADL).5)6) The treatment for HF includes cardiac rehabilitation as one of the non-pharmacological treatments in addition to the pharmacological treatments. Exercise-based cardiac rehabilitation for patients with chronic HF (CHF) has been reported to improve exercise capacity,7)8) quality of life (QOL),7)8) autonomic function,9) endothelial function,10) depression,11) and cardiac function.8)12) In fact, HF management guidelines in various countries provide exercise-based cardiac rehabilitation with class I recommendations.2)13)14) However, much of the evidence is limited to CHF. In recent years, the effectiveness of rehabilitation interventions for AHF has been reported, and its safety has also been reported. According to the guidelines for rehabilitation in cardiovascular disease, the purposes of cardiac rehabilitation for patients with AHF are (1) to prevent the adverse effects of excessive bed rest (e.g., physical function decline, cognitive decline, delirium, pressure ulcer, pulmonary emboli) by early mobilization, and (2) to develop and implement a plan to ensure early and safe discharge and prevent rehospitalization.14) The initiation of cardiac rehabilitation in patients with AHF is extremely important not only to achieve early discharge from the hospital, but also to lead to continued participation in cardiac rehabilitation after discharge. Therefore, this review will focus on recent findings regarding the effectiveness of rehabilitation and exercise therapy for patients with AHF. Moreover, in recently reported randomized controlled trials (RCTs) examining the effects of exercise therapy in patients with AHF, physical function was set as the primary outcome. Therefore, we will also briefly discuss the implications of physical function in patients with HF.
Go to : 
PHYSICAL FUNCTION MEASURES IN PATIENTS WITH HEART FAILURE
The physical function includes skeletal muscle strength and skeletal muscle function. The physical function decline can lead to loss of independence, need for hospitalization or long-term nursing-home care, and early death. At the same time, physical function is an essential measure of the effectiveness of cardiac rehabilitation interventions. In a meta-analysis of 22,598 HF patients that included 44 longitudinal observational cohort studies, HF patients with low physical function were associated with a high risk of hospitalization and death.15) A recently-reported RCT examining the effects of exercise therapy in patients with AHF has also included physical function as a study outcome.16) Therefore, we will briefly discuss physical function measurements commonly performed in daily practice.
Six-minute walk test
The 6-minute walk test (6MWT) is an objective quantitative method for assessing functional and/or exercise capacity in patients with HF. The 6MWT is a simple test in which participants are asked to walk back and forth down a 30-meter corridor at their chosen pace for 6 minutes and measure the distance.17) A cutoff value of 400 m is considered to screen for mobility limitation,18) and a cutoff value of 300 m is widely used for increased risk of mortality in patients with HF.19)20)21) Minimal clinically important difference (MCID) is the amount of change in the rating scale by which the effectiveness of the treatment can be judged to have been achieved, and if the amount of change due to treatment exceeds the MCID, it can be determined that a meaningful change has occurred.22) MCID values at 6-minute walk distance (6MWD) are considered to be 20 to 30 m,23)24) and if the baseline 6MWD exceeds 450 m, it is difficult to obtain improvement.25) Cardiopulmonary exercise testing (CPX) is the gold standard for assessing exercise tolerance,26) but it is time-consuming, expensive, and requires specialized equipment and personnel. Therefore, 6MWT is widely used as an alternative indicator in clinical practice. Exercise tolerance as assessed by 6MWT is highly correlated with peak VO2 obtained by CPX27) and reflects the prognosis, severity, and QOL of patients with HF.27)28)29)30)31)
Gait speed
Gait speed, measured as the time required to walk a short distance at a comfortable or maximal pace, is a commonly used test to screen for sarcopenia and frailty.5)32) Gait speed is a reliable test that requires little space or time.33) Gait speed is generally measured with a 5-meter acceleration path, a 10-meter measurement path, and a 5-meter deceleration path, for a total of 20 m, and can also be measured in a 4-meter path.33) A meta-analysis of 34,485 older adults that included 9 cohort studies reported hazard ratio (HR) for survival per 0.1 m/s faster gait speed was 0.88 (95% confidence interval [CI], 0.87–0.90; p<0.001),34) and gait speed is a useful prognostic indicator. While many cutoff values for gait speed to predict death, hospitalization, and falling have been reported (e.g., 0.7, 0.8, 1.0 m/s),32)35)36)37) the cutoff for slowness in sarcopenia and frailty is 1.0 m/s.38)39) Several studies have shown that a single measure of gait speed outperformed other multicomponent frailty scales in predicting outcomes.40)41) Gait speed is an independent predictor of prognosis in patients with HF and improves risk stratification in older patients with HF evaluated using the Cardiac and Comorbid Conditions HF score.42) Moreover, gait speed is useful in predicting patients at high risk of developing HF.43)44) In general, usual gait speed is often used in routine practice, but maximal gait speed and subjective gait speed are also important as a prognostic predictor.45)46)
Short Physical Performance Battery
The Short Physical Performance Battery (SPPB) provides a valuable and indirect measure of muscle functional capacity.47) The SPPB is an objective tool for evaluating the lower extremity physical performance status.48)49) The SPPB consists of 3 tests:
▪ Balance (feet together, semi tandem, and tandem for 10 seconds each)
▪ Gait speed (4 m)
▪ Standing up and sitting on a chair five times
Each test is scored from 0 (worst performance) to 4 (best performance), and the total score ranges from 0 to 12 points (Figure 1).48) The SPPB is a valuable instrument capable of classifying frailty and/or pre-frailty.50) In general, SPPB of 0 to 6 is classified as frail, SPPB of 7 to 9 as pre-frail, and SPPB of 10 to 12 as robust.51) A low SPPB score (0 to 6) is associated with an increased risk of all-cause death and HF readmission in older patients hospitalized for AHF.52)
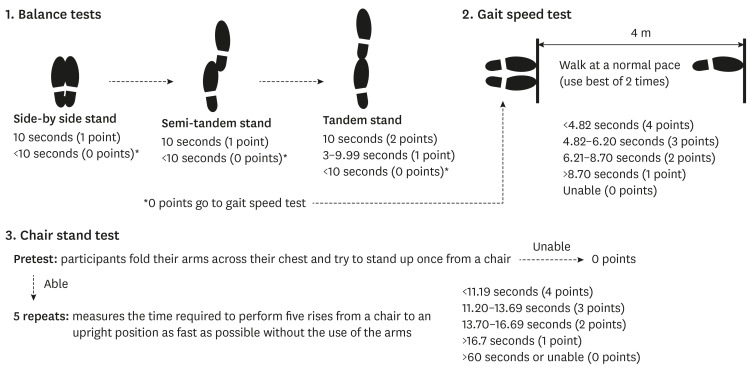 | Figure 1Short Physical Performance Battery.Figure was created based on https://www.nia.nih.gov/research/labs/leps/short-physical-performance-battery-sppb.
|
Lower extremity muscle strength
Lower extremity muscle strength, especially the quadriceps muscle, is a strong determinant of gait and exercise tolerance53)54) and is directly related to independence in ADL in older adults.55) Moreover, quadriceps isometric strength (QIS) is a useful prediction of exercise capacity and is associated with mortality in patients with coronary artery disease.56)57) Metabolic equivalents (METs) are units of exercise or physical activity intensity, with a resting sitting position of 1 METs. For example, 5 METs, 7 METs, and 10 METs reflect the most light-to-moderate, moderate-to-high, and high-to-vigorous intensity; household, occupational, and sports activities, respectively (Figure 2),58) and are indicators of return to society and work. The QIS cutoff values for predicting exercise capacity in patients with coronary artery disease were 5 METs: 45% body weight (BW), 7 METs: 50% BW, and 10 METs: 60% BW, respectively.56)58) Furthermore, QIS is a prognostic factor in patients with HF and has the complementary predictive ability of HF risk score and gait speed in patients with HF.59)
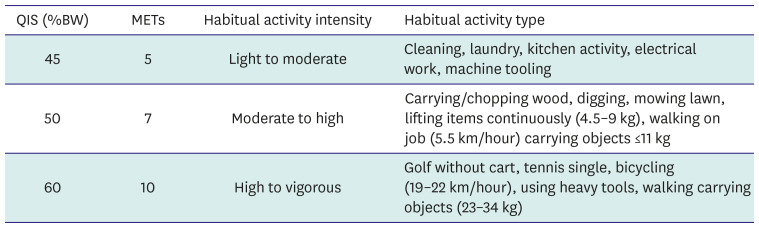 | Figure 2Association between quadriceps isometric strength and levels of exercise capacity and habitual activities.Figure was created based on a report by Kamiya et al.56) Ainsworth et al.58) presents a complete list showing the relationship between the different QIS/METs categories.
BW = body weight; MET = metabolic equivalent; QIS = quadriceps isometric strength.
|
Go to :
CARDIAC REHABILITATION IN PATIENTS WITH CHRONIC HEART FAILURE
Cardiac rehabilitation is a disease management program for patients with cardiovascular disease and is a non-pharmacological treatment essential to prevent rehospitalization due to exacerbation of HF, which is the goal of treatment for patients with HF. Cardiac rehabilitation consists of not only exercise therapy but also a multidisciplinary intervention. The components of cardiac rehabilitation include: the traditional 1) medical evaluation of the patient’s condition and severity, 2) exercise prescription and exercise training based on the medical evaluation, 3) improvement of coronary risk factors and patient education, 4) counseling regarding psychosocial factors and return to work,60) and a new component 5) disease management.14) The background for the emphasis on disease management is due to the aging of HF patients, the increasing number of HF patients with frailty and cognitive dysfunction,1)5) and the increasing number of readmissions due to inadequate management after discharge.1) The disease management program is an intervention by a multidisciplinary medical team that includes: 1) provision of standard medical care based on medical guidelines, 2) thorough self-management (self-care) through patient education, lifestyle guidance, and motivation, and 3) early detection of worsening disease through telephone and in-home monitoring. These interventions have been reported to reduce rehospitalization for HF and improve prognosis.61)62)
Exercise programs in patients with CHF consist of aerobic and resistance exercises, including a pre-exercise warm-up and post-exercise cool-down. The frequency of aerobic training exercise is aimed at 3 to 5 times per week.14)63) The intensity of aerobic training exercise can be prescribed based on peak VO2 percentage, heart rate reserve (HRR), or subjective exercise intensity. Specifically, in patients with HF for whom CPX has been measured, aerobic training exercise prescribes at 1) 30–50% of HRR, 2) 40–60% of peak VO2, and 3) HR at anaerobic threshold (AT) level, and if CPX is difficult, aerobic training exercise is prescribed at a target level of 11–13 Borg scale as subjective exercise intensity.14)63)64) In general, the rate of perceived exertion of less than 12 by the Borg scale corresponds to less than 40% of HRR, 12–13 to 40–59%, and 14–17 to 60–89%.65) The time of aerobic training exercise is recommended to start at around 5 to 10 minutes and gradually increase to 20 to 30 minutes per day.14) The types of aerobic training exercise include walking, bicycle ergometers, and treadmills. The optimal intensity of resistance training depends on whether the goal is to improve muscle strength or endurance. If the primary goal is to improve endurance, low-intensity training (30% to 40% of maximal strength, 10 to 25 repetitions) should be performed 2 to 3 days per week. If the primary goal is to improve muscle strength, training should be performed at a high intensity (40% to 60% of maximal strength), with a low number of repetitions (8 to 15) and performed 2 to 3 days per week.63)66)67)
The benefits of cardiac rehabilitation in patients with CHF are well documented. A recent systematic review and meta-analysis of exercise-based rehabilitation for patients with HF in 44 trials showed a reduction of 30% in all-cause rehospitalization rates, a reduction of 41% in HF rehospitalization rates, and an improvement in QOL as assessed by the Minnesota Living With HF Questionnaire (average improvement of 7.1 points).7) Also, in a multicenter retrospective cohort study of 3,277 Asian patients with CHF, a multidisciplinary cardiac rehabilitation intervention was associated with a lower risk of long-term all-cause mortality and HF rehospitalization.68)
Despite the obvious benefits of cardiac rehabilitation in patients with CHF, there are issues that need to be resolved. A nationwide survey on multidisciplinary treatment and cardiac rehabilitation of patients with CHF in Japan highlighted the low participation rate of cardiac rehabilitation among patients with CHF. Of the 51,323 patients with HF, 60% did not receive inpatient and outpatient cardiac rehabilitation, 33% received rehabilitation only during hospitalization, and only 7% received inpatient and outpatient rehabilitation.69) In addition, participation and adherence to cardiac rehabilitation are lower among women.70) Nevertheless, cardiac rehabilitation reduced all-cause mortality and hospitalization rates in women (HR, 0.74; 95% CI, 0.59–0.92) but not in men (HR, 0.99; 95% CI, 0.86–1.13),70) suggesting that women may benefit more from cardiac rehabilitation. However, evidence for cardiac rehabilitation in women is scarce.71) In summary, participation in cardiac rehabilitation is very low among patients with CHF, especially among women who are more likely to benefit. There is a need for novel ideas to increase participation rates in cardiac rehabilitation. Further research is also needed to identify populations that would benefit more from cardiac rehabilitation.
Go to :
EXERCISE THERAPY FOR PATIENTS WITH ACUTE HEART FAILURE
The Rehabilitation Therapy in Older Acute Heart Failure Patients (REHAB-HF) trial results, a multicenter, randomized, single-blind, controlled trial examining the effects of exercise therapy on older patients hospitalized for acute decompensated HF (ADHF), were reported in 2021.16) This trial examined the effects of a progressive, individualized rehabilitation intervention on four domains of physical function (strength, balance, mobility, and endurance) in 349 older patients (mean age 72.7 years, 97% of patients were frail or pre-frail) hospitalized for ADHF. The intervention was initiated during or early after hospitalization for HF and continued for 36 outpatient sessions after discharge. In contrast, the control group was allowed conventional rehabilitation interventions. The primary outcome was the score on the SPPB at three months. The secondary outcome was the rate of all-cause rehospitalization for six months. Additional outcomes included 6MWD and the Kansas City Cardiomyopathy Questionnaire (KCCQ) score. As a result, the least-squares mean (±standard error) score on the SPPB at three months was 8.3±0.2 in the intervention group and 6.9±0.2 in the control group (mean between-group difference, 1.5; 95% CI, 0.9–2.0; p<0.001). A noteworthy aspect of the effects of the intervention is that the intervention-related benefits observed in this study exceeded the MCID values reported to date. The mean difference in SPPB scores between groups (1.5 points) was greater than the previously reported MCID (1.0 points).72) The effects of the intervention on the secondary outcomes, 6MWD (34 m) and KCCQ score (7.1 points), were also greater than the MCID reported (20 to 30 m and 5 points, respectively).23)24)73) On the other hand, the effectiveness of the intervention on all-cause rehospitalization for six months after discharge could not reach the statistical significance.
This trial has received a great deal of attention as a study that has demonstrated the effectiveness of exercise-based rehabilitation for older ADHF patients with frail. Physical frailty was defined as “a clinical syndrome of increased vulnerability resulting from age associated decline in reserve and function across multiple physiologic systems such that the ability to cope with everyday acute stress is compromised” by Fried et al.74) In the REHAB-HF trial, 97% of patients with ADHF had pre-frail or frail using the Fried criteria. On the other hand, the prevalence of frail reported in the community dwelling older adults range from 4.0 to 59.1%, and the overall weighted prevalence of frailty was 10.7%.75)
This trial addresses an important evidence gap in physical rehabilitation of patients with HF reported to date. In many previous trials, patients who had been hospitalized within the previous six weeks were excluded. This is because the risk of clinical events is highest during this period. On the other hand, in this trial, rehabilitation interventions were performed as early as feasible. Additionally, patients in the previous study were relatively young and failed to address any comorbidities.76) The REHAB-HF trial, on the other hand, reported that the benefits of acute-phase rehabilitation were consistently observed in subgroups classified by age, gender, race, body mass index, ejection fraction (EF), New York Heart Association (NYHA) functional class, and various comorbidities including atrial fibrillation, diabetes mellitus, and chronic kidney disease. Furthermore, the adherence to the exercise intervention in this trial was 76±3%, which seems to be an impressive result. In the Heart Failure: A Controlled Trial Investigating Outcomes of Exercise Training (HF-ACTION), a clinical trial of exercise training for patients with HF, full adherence to exercise was about 30%.77)
The exercise intervention protocols in this trial are attracting much attention. Initially, the patient’s physical function was evaluated in 4 categories: “strength: rise from a chair without hand support,” “balance: static standing balance,” “endurance: continuous walking,” and “mobility: gait speed,” each of which was divided into 4 levels. Then, a rehabilitation program was implemented across four domains of physical function based on functional performance level in each domain and was progressed as patients improved in function. The amount of time spent in each domain during the session was tailored to the participant’s physical function impairments. For example, a participant with poor balance and functional mobility spent more time performing balance and mobility exercises early in the intervention. In contrast, a participant with only modest impairments in balance and functional mobility at baseline spent most of the session performing endurance and strengthening exercises. This exercise intervention protocol was set up to gradually progress in small increments from session to session. The traditional and widely practiced cardiac rehabilitation has been an aerobic exercise-based program. However, this special, progressive program confirmed the importance of following the frequency, intensity, time, type, volume, and progression (FITT-VP) principles of exercise prescription,78) even in patients with AHF.
Go to :
EARLY REHABILITATION OF PATIENTS WITH ACUTE HEART FAILURE
The current definition of early mobilization refers to physical exercise performed within 2–5 days of critical illness or injury.79) Muscle loss due to immobility begins within 48–72 hours of surgery, new onset of disease, or acute exacerbation.80)81)82) Up to a 40% loss in skeletal muscle strength has been reported to occur within the first week of immobilization, with a daily strength decline rate of 1.0–5.5%.83)84) Therefore, it can be interpreted that early rehabilitation is advisable to begin within 48 hours of new-onset of disease, surgery, or acute exacerbation. In fact, the effectiveness of rehabilitation interventions within 48 hours has been reported in numerous studies.85)86)87)88) A meta-analysis examining the effect of early mobilization, which included 15 RCTs with a total of 1941 critically ill patients, found that early mobilization significantly reduced the incidence of intensive care unit (ICU)-acquired weakness, shortened the length of ICU and length of hospital stays, and improved the Medical Research Council score and Barthel Index score at hospital discharge.89) In addition, early mobilization also decreased complications such as deep vein thrombosis, ventilator-associated pneumonia, and pressure sores.89)
In a nationwide inpatient database, the effectiveness of acute-phase initiation of rehabilitation for patients with AHF has been reported. We reported the impact of acute-phase initiation of rehabilitation on short-term clinical outcomes and improvement of ADL in patients with AHF.85)86) Acute-phase initiation of rehabilitation was defined as an intervention within 2 or 3 days of admission, and propensity score matching was used to determine its effectiveness. As a result, 14.8% of patients received acute-phase initiation of rehabilitation (intervention within 2 days of admission). After propensity score matching, median length (interquartile range) of hospital stay (16 [11–25] days vs. 17 [11–27] days, p<0.001) was shorter and in-hospital mortality (5.4% vs. 6.9%, p<0.001) and 30-day readmission rate due to HF (5.9% vs. 6.4%, p=0.001) were lower in patients with the acute-phase initiation of rehabilitation. Moreover, acute-phase initiation of rehabilitation was associated with improvement of ADL.86) The frequency of adverse events attributable to early mobilization in older adults with acute cardiovascular disease was very low at 0.2%.90) Therefore, initiation of rehabilitation intervention within 48–72 hours of admission, depending on appropriate risk management and management status of the condition, should be recommended to ensure favorable, at least short-term clinical outcomes.
The results of several RCT trials examining the benefit of early rehabilitation during hospitalization in patients with AHF have been reported and are shown in Table 1. Although the number of RCTs was limited, the primary outcome was improvement in physical function. As a result, the early rehabilitation intervention group showed improvement in 6MWD, SPPB, QIS, and ADL compared to the control group.91)92)93)94) The change in amino-terminal pro-B-type natriuretic peptide (NT-proBNP) was examined in only one trial, and while NT-proBNP was significantly reduced, there was no difference between the intervention and control groups.91) There is a lack of evidence to determine the effect of early rehabilitation on clinical outcomes in patients with AHF. Especially, the impact on left ventricular EF, HF-related rehospitalization, and all-cause mortality is of critical importance. Moreover, many studies have focused on short-term outcomes, but the long-term effects of early rehabilitation intervention in patients with AHF have not been fully examined. Further evidence is needed to clarify the effects of early rehabilitation in patients with AHF.
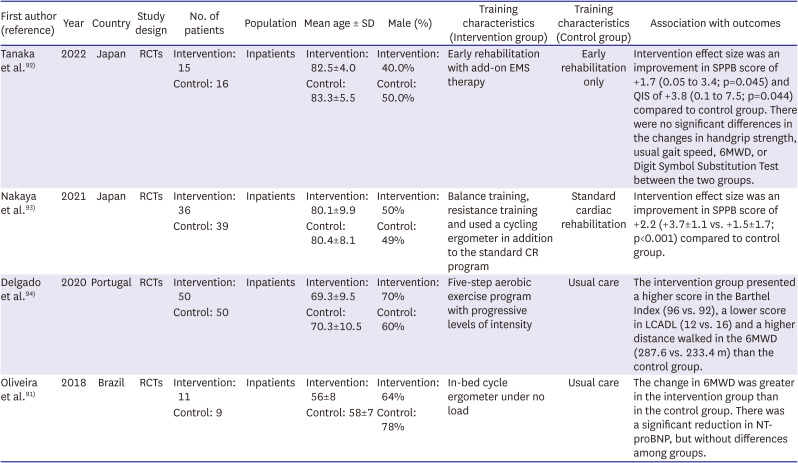
Table 1
Randomized controlled trial examining the effects of early rehabilitation during hospitalization in patients with acute heart failure
| First author (reference) | Year | Country | Study design | No. of patients | Population | Mean age ± SD | Male (%) | Training characteristics (Intervention group) | Training characteristics (Control group) | Association with outcomes |
|---|---|---|---|---|---|---|---|---|---|---|
| Tanaka et al. 92) | 2022 | Japan | RCTs | Intervention: 15 | Inpatients | Intervention: 82.5±4.0 | Intervention: 40.0% | Early rehabilitation with add-on EMS therapy | Early rehabilitation only | Intervention effect size was an improvement in SPPB score of +1.7 (0.05 to 3.4; p=0.045) and QIS of +3.8 (0.1 to 7.5; p=0.044) compared to control group. There were no significant differences in the changes in handgrip strength, usual gait speed, 6MWD, or Digit Symbol Substitution Test between the two groups. |
| Control: 16 | Control: 83.3±5.5 | Control: 50.0% | ||||||||
| Nakaya et al. 93) | 2021 | Japan | RCTs | Intervention: 36 | Inpatients | Intervention: 80.1±9.9 | Intervention: 50% | Balance training, resistance training and used a cycling ergometer in addition to the standard CR program | Standard cardiac rehabilitation | Intervention effect size was an improvement in SPPB score of +2.2 (+3.7±1.1 vs. +1.5±1.7; p<0.001) compared to control group. |
| Control: 39 | Control: 80.4±8.1 | Control: 49% | ||||||||
| Delgado et al. 94) | 2020 | Portugal | RCTs | Intervention: 50 | Inpatients | Intervention: 69.3±9.5 | Intervention: 70% | Five-step aerobic exercise program with progressive levels of intensity | Usual care | The intervention group presented a higher score in the Barthel Index (96 vs. 92), a lower score in LCADL (12 vs. 16) and a higher distance walked in the 6MWD (287.6 vs. 233.4 m) than the control group. |
| Control: 50 | Control: 70.3±10.5 | Control: 60% | ||||||||
| Oliveira et al. 91) | 2018 | Brazil | RCTs | Intervention: 11 | Inpatients | Intervention: 56±8 | Intervention: 64% | In-bed cycle ergometer under no load | Usual care | The change in 6MWD was greater in the intervention group than in the control group. There was a significant reduction in NT-proBNP, but without differences among groups. |
| Control: 9 | Control: 58±7 | Control: 78% |
6MWD = 6-minute walk test; CR = cardiac rehabilitation; EMS = electrical muscle stimulation; LCADL = London Chest Activity of Daily Living; NT-proBNP = amino-terminal pro-B-type natriuretic peptide; QIS = quadriceps isometric strength; RCT = randomized controlled trial; SD = standard deviation; SPPB = Short Physical Performance Battery.
![]()
Go to :
REHABILITATION INTERVENTIONS FOR PATIENTS WITH SEVERE ACUTE HEART FAILURE
In a nationwide inpatient database, 13.4% of patients hospitalized for AHF who underwent early rehabilitation (initiation of rehabilitation within 2 days of admission) received intravenous inotropic drugs.85) The results indicate that it is common to encounter patients who are on inotropic drugs when intervening in rehabilitation from the acute phase. Guidelines for rehabilitation in cardiovascular disease recommend rehabilitation such as low-intensity resistance training under close supervision for hemodynamically stable HF patients receiving intravenous inotropic drugs.14) Recently published practical recommendations indicate that patients who do not require life support equipment and do not have untreated life-threatening arrhythmias or hemodynamic instability, etc., are recognized as indications for exercise therapy.14)66)67) Early rehabilitation has been useful in improving short-term outcomes in patients hospitalized for AHF with NYHA class IV.85) In patients receiving intravenous inotropic drugs, it has been reported that exercise therapy can be safely administered by adjusting the exercise load, leading to improved exercise tolerance and respiratory muscle strength.95) However, there is insufficient evidence regarding the effectiveness of rehabilitation and criteria for initiation of rehabilitation in AHF patients receiving intravenous inotropic drugs, and further large studies are needed to investigate this issue.
Go to :
NEW OPTIONS FOR REHABILITATION INTERVENTION FOR PATIENTS WITH ACUTE HEART FAILURE
The REHAB-HF trial reported that 97% of older patients hospitalized for ADHF were frail or pre-frail,5) and the FRAGILE-HF cohort study reported that 56.2%, 66.3%, and 37.2% of older patients hospitalized for decompensation of HF had physical frailty, social frailty, and cognitive dysfunction, respectively.96) These results highlighted the requirement of additional passive rehabilitation programs. In particular, older patients with frailty are prone to prolonged periods of inactivity and loss of skeletal muscle.81)97) The ACTIVE-EMS trial is a multi-center, randomized, controlled trial examining the safety and impact on physical function of electrical muscle stimulation (EMS) therapy as an add-on to traditional early rehabilitation for older patients with frailty hospitalized for AHF.92) This trial randomized patients to early rehabilitation with add-on EMS therapy (EMS group) or early rehabilitation only (control group). As a result, the EMS group had a significantly greater improvement in QIS (5.9±7.0% BW vs. 0.8±3.3% BW) and SPPB (4 [2 to 5] vs. 2 [−1 to 3]) compared to the control group. Moreover, there were no adverse events during EMS periods. Other RCTs have also reported on the usefulness of EMS for patients with advanced HF. EMS therapy during hospitalization showed a significant increase in 6MWD, improved QOL, and reduced dose of dobutamine compared to controls in patients hospitalized with advanced HF.98)99) Therefore, add-on approaches, such as EMS therapy, may be helpful in older patients with AHF.
Malnutrition in patients hospitalized for AHF has received increasing attention. In the FRAGILE-HF cohort study, 42.4% of older patients hospitalized for decompensation of HF had malnutrition as defined by the Global Leadership Initiative on Malnutrition (GLIM) criteria.100) Moreover, malnutrition was associated with increased all-cause mortality, even after adjustment for the Meta-analysis Global Group in Chronic Heart Failure (MAGGIC) risk score and BNP (HR, 1.57; 95% CI, 1.09–2.27).100) The GLIM criteria are a tool for diagnosing malnutrition proposed by the GLIM consensus paper.101) The GLIM criteria consist of three phenotypic and two etiologic components for diagnosing malnutrition; at least one criterion from each component must be satisfied to diagnose malnutrition (Figure 3).101) In addition, malnutrition is associated with low physical function in patients with cardiovascular disease, including HF.102) Hence, malnutrition in patients with AHF is frequently observed and early nutritional support may be important to maximize the benefits of early rehabilitation in patients with AHF. Although it remains under-reported, combining early nutritional therapy with early exercise in patients with critical illness holds promise as an intervention that can lead to a favorable outcome.103) Therefore, RCT trials are needed to determine whether early nutritional support in addition to early rehabilitation improves prognosis and functional outcome compared to early rehabilitation alone in patients with AHF.
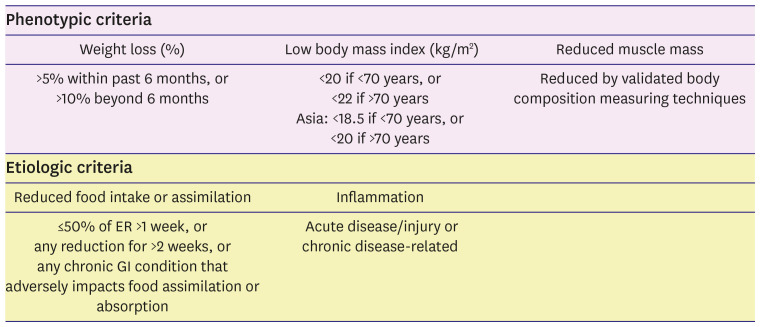 | Figure 3Global Leadership Initiative on Malnutrition criteria for the diagnosis of malnutrition.Figure was created based on a report by Cederholm et al.101)
ER = energy requirements; GI = gastrointestinal.
|
Go to :
REHABILITATION FOR PATIENTS WITH HEART FAILURE WITH PRESERVED EJECTION FRACTION
In a sub-analysis in the REHAB-HF trial, the effect of exercise therapy was compared between HF with preserved EF (HFpEF) and HF with reduced EF (HFrEF).104) The percentages of HFpEF and HFrEF were 53% and 47%, respectively. Patients with HFpEF were more women and frail, had a lower physical function and QOL, and depression was more common compared to patients with HFrEF. There was no interaction effect of exercise therapy on the improvement of physical function, but the effect size appeared nominally larger in patients with HFpEF. Moreover, there was no significant difference in all-cause rehospitalizations or HF hospitalizations, but the effect size was larger in patients with HFpEF than in patients with HFrEF. Furthermore, in the HFpEF group, the intervention was associated with a nominally lower death rate compared to the HFrEF group.
A multicenter, retrospective study conducted in Japan examined the impact of outpatient multidisciplinary cardiac rehabilitation on long-term prognosis in patients with HFpEF. After propensity score matching, participation in outpatient cardiac rehabilitation was associated with a favorable long-term prognosis.68)
These results suggest that patients with HFpEF have worse baseline characteristics in various aspects than HFrEF and may benefit more from rehabilitation interventions.
Go to :
CONCLUSION
The evidence on the effectiveness of rehabilitation for patients with AHF is accumulating. The most important thing is that appropriate intervention methods are being proposed for patients with AHF who are aged and have frailty. Given these considerations, implementing a strategic rehabilitation program from the acute phase has the more beneficial effect on clinical outcomes than traditional rehabilitation interventions alone. Further clinical research is needed to identify an optimal acute-phase rehabilitation regimen for patients with AHF.
Go to :
 XML Download
XML Download