

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The clinical benefits of β-blockers for reducing adverse cardiovascular events have been reported in previous randomized trials in patients with acute myocardial infarction (AMI) or heart failure (HF) with systolic dysfunction.1) In contrast, the general notion that β-blockers are cardioprotective for patients with chronic coronary artery disease (CAD) is mainly based on the extrapolation of evidence from studies in patients with myocardial infarction (MI)2)3)4) or HF.5)6) To date, although several observational studies have evaluated the outcome benefits of β-blockers in chronic CAD, they have only shown conflicting results.3)7)8)9) One of the important limitations of the previous studies was that patient groups had been categorized according to β-blocker use at a single time point, mostly at discharge or after coronary revascularization, which did not reflect temporal variations in β-blocker therapy. In addition, it has not been fully assessed whether there is a dose-dependent effect of β-blockers on clinical outcomes in patients with chronic CAD.
Thus, we aimed to clearly reveal the impact of β-blocker therapy on outcomes in patients with chronic CAD after percutaneous coronary intervention (PCI), and in pre-specified subgroups with previous MI and/or revascularization, or congestive heart failure (CHF) and/or left ventricular (LV) dysfunction. In addition, we aimed to investigate the dose-dependent effects of β-blocker therapy in the study population. To this end, we meticulously gathered medical records on the prescription and dose of β-blockers for each patient, throughout the follow-up period.
METHODS
Ethical statement
This study protocol complied with the Declaration of Helsinki 2013, and was reviewed and approved by the Institutional Review Board (IRB) of the Seoul National University Hospital (H-1707-143-872). The study was waived for informed consent by the IRB.
Data source and study population
The study population was obtained from the Grand Drug-Eluting Stent (Grand-DES) registry (NCT03507205), a patient-level pooled registry comprising 5 multicenter prospective DES registries hosted by Seoul National University Hospital. A total of 17,286 patients who underwent PCI with DES implantation were enrolled from 55 participating centers in Korea.
To overcome the limitations of previous studies that categorized patient groups according to β-blocker use at a single time point (usually at discharge or after index PCI), we reviewed each patient’s medical records for β-blockers, including prescription doses and types, at 3-month intervals after discharge. We excluded patients without available data on β-blocker use (n=5,799), those with non-continuous prescription of β-blockers (n=1,722), and those with acute coronary syndrome, including MI or unstable angina, at initial presentation (n=6,690). Non-continuous β-blocker users were defined as those who had not been prescribed β-blockers at any point during the 3-month time intervals of the follow-up period. We did not excluded patents on β-blocker therapy whose specific β-blocker product might have changed during the follow-up period because we purposed to evaluate the prognostic effect of the β-blockers as a class effect but not as per specific product. Finally, a total of 3,075 patients with chronic CAD were included (Figure 1). Baseline characteristics, including age, sex, and cardiovascular risk factors, were acquired from the registry. Additionally, coronary angiography data, including coronary lesion characteristics and procedure information, and medication records were also acquired.

Figure 1
Study flow.
A total of 17,286 patients with CAD who had undergone PCI were screened for inclusion from the Grand-DES multi-center registry. We excluded patients whose prescription records of β-blockers were not available and those with non-continuous use of β-blockers during the follow-up period. Finally, a total of 3,075 patients with chronic CAD were included. After propensity score matching, a total of 1,170 pairs of patients were finally derived.
CAD = coronary artery disease; DES = drug-eluting stent; PCI = percutaneous coronary intervention; PS = propensity score.
![]()
Dose and type of β-blockers
Based on the β-blocker prescription records, which included the daily frequency (times per day) and amount administered (milligram per administration), the daily dose of β-blockers was calculated by multiplying these 2 factors. The daily dose was then translated into a percentage (%) of the full dose targeted by previous randomized trials: metoprolol 200 mg/day,10) carvedilol 50 mg/day,1) propranolol 160 mg/day,11) bisoprolol 10 mg/day,12) atenolol 100 mg/day,13) nebivolol 10 mg/day,14) betaxolol 40 mg/day,15) and bevantolol 200 mg/day.16) Afterwards, each translated % value during the entire follow-up period was averaged. Finally, patients were grouped into three dose categories based on the mean values of β-blocker doses as “low-dose” (<25% of full dose), “medium-dose” (≥25% to <50% of full dose), and “high-dose” (≥50% of full dose) β-blocker groups, as used in previous studies.17)18)19) Patients were also categorized into two groups according to the vasodilating property of β-blockers: “vasodilating β-blockers” (carvedilol, nebivolol, betaxolol, and bevantolol) and “conventional β-blockers” (bisoprolol, metoprolol, atenolol, and propranolol).
Statistical analysis
We defined the primary outcome as a composite endpoint of all-cause death and MI. The individual clinical outcomes (all-cause death, cardiac death, and MI) were included as secondary outcomes. Cardiac death was defined as death resulting from AMI, HF, sudden cardiac death, and other cardiovascular causes. Patients were longitudinally followed from the date of discharge to that of an outcome event or the end of follow-up, whichever came first. The clinical outcomes were reported by researchers at each participating center and monitored by Seoul National University Hospital. We employed propensity score (PS) matching technique for balancing baseline characteristics between the patients with β-blockers and no β-blockers. In brief, the PS for β-blocker therapy was calculated using an ordinary logistic regression based on covariates from the baseline characteristics.20) We considered the maximum absolute standardized difference of 0.1 (10%) as a negligible difference in the covariates among the matched population.21) After PS matching, a total of 1,170 pairs of patients were finally derived (Figure 1), with well-balanced baseline features (Supplementary Figure 1).
We applied the Cox proportional-hazard regression model to estimate the hazard ratios (HRs) for each clinical outcome according to β-blocker therapy. Kaplan-Meier curves were used to plot the time-to-event distribution of the clinical outcomes, with differences in the event-free rate examined using the log-rank test. We performed subgroup analysis for primary outcome and all-cause death to inspect whether the effect of β-blockers differs with old age (≤70 years), sex, presence of clinical risk factors, type of DES implanted, and duration of dual antiplatelet therapy. Particularly, we evaluated the differential effect of β-blockers in patients with previous MI and/or revascularization, and in those with CHF and/or LV systolic dysfunction at initial echocardiography (ejection fraction <40%), because these groups have been considered to benefit from β-blocker therapy.2)3)4)5)6)
We further evaluated the associations of the different doses and types of β-blockers with clinical outcomes. Patients with β-blockers from the matched population were further classified according to the different dose categories and types of β-blockers. To analyze the effect of different types of β-blockers, we excluded patients whose β-blockers had been changed to the opposite class (i.e., from vasodilating to conventional, or vice versa) during follow-up (n=139). The HRs for each clinical outcome were then estimated after multivariate adjustment for the baseline characteristics.
All probability values were two-sided, and p values <0.05 were considered statistically significant. R version 3.4.3 (R Development Core Team, Vienna, Austria) was used for statistical analyses.
RESULTS
Baseline characteristics
Table 1 summarizes the baseline characteristics of the crude and PS matched population according to β-blocker therapy. A total of 1,636 (53.2%) patients received β-blockers after PCI. Compared with the no β-blocker group, the β-blocker group showed a higher prevalence of previous MI and/or revascularization (18.6% vs. 24.4%, p<0.001), hypertension (62.5% vs. 71.0%, p<0.001), and multivessel coronary disease (58.3% vs. 64.7%, p<0.001). After PS matching, the significant differences in the baseline characteristic were disappeared.
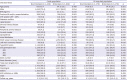
Table 1
Baseline characteristics of study population
Values are given as mean±standard deviation, median (interquartile range) or numbers (percentages), unless otherwise indicated.
ACE = angiotensin-converting enzyme; ARB = angiotensin II receptor blocker; BES = Biolimus A9 eluting coronary stent; BP = blood pressure; BMI = body mass index; CCB = calcium channel blocker; CHF = congestive heart failure; DES = drug-eluting stent; EES = Everolimus eluting coronary stent; LVEF = left ventricular ejection fraction; MI = myocardial infarction; ZES = Zotarolimus eluting coronary stent.
![]()
Clinical outcomes associated with β-blocker therapy
During the median follow-up of 3.1 (3.0–3.1) years, 134 (5.7%) primary outcome, 119 (5.1%) deaths and 21 (0.9%) MI occurred among the matched population. The β-blocker group was not associated with better clinical outcomes compared with no β-blocker group, regarding primary outcome (5.4% vs. 6.1%, HR, 0.88; 95% confidence interval [CI], 0.63–1.24), all-cause death (4.6% vs. 5.6%, HR, 0.82; 95% CI, 0.57–1.18), cardiac death (3.3% vs. 3.0%, HR, 1.11; 95% CI, 0.70–1.76), and MI (1.1% vs. 0.8%, HR, 1.33; 95% CI, 0.56–3.15) (Table 2, Figure 2, and Supplementary Figure 2).
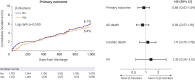

Figure 2
Clinical outcomes according to β-blocker therapy in matched population.
Among the matched population, the β-blocker group was not associated with better clinical outcomes in primary outcome, all-cause death, cardiac death, and MI compared with the no β-blocker group.
CI = confidence interval; HR = hazard ratio; MI = myocardial infarction.
![]()
Table 2
Event numbers and cumulative incidence of the study outcomes at 3-year in crude and matched population
![]()
On the subgroup analysis, there was no significant difference in primary outcome associated with β-blocker therapy across the various subgroups (Figure 3). For all-cause death, β-blockers showed a lower event risk in patients with previous MI and/or revascularization (HR, 0.38; 95% CI, 0.14–0.99) but not in those without it (HR, 0.91; 95% CI, 0.60–1.39) (p for interaction=0.045).

Figure 3
Subgroup analysis for primary outcome and all-cause death associated with β-blocker therapy.
There was no significant difference in primary outcome associated with β-blocker therapy across the various subgroups. β-blockers were associated with a lower risk of all-cause death in patients with previous MI and/or revascularization.
BES = Biolimus A9 eluting coronary stent; CHF = congestive heart failure; CI = confidence interval; DAPT = dual antiplatelet therapy; DES = drug-eluting stent; EES = Everolimus eluting coronary stent; HR = hazard ratio; LVEF = left ventricular ejection fraction; MI = myocardial infarction; ZES = Zotarolimus eluting coronary stent.
![]()
The effect of different doses and types of β-blocker therapy on clinical outcomes
After stratifying the patients according to mean β-blocker doses during follow-up, 407 (34.5%), 533 (45.6%), and 230 (19.7%) patients were allocated to the low-, medium-, and high-dose β-blocker groups, respectively (Supplementary Table 1). Patients in the high-dose β-blocker group showed higher prevalence of previous MI and/or revascularization (28.7%) than the other dose groups (21.2% and 20.6% in the medium- and low-dose groups, respectively). There was a dose-dependent tendency of lower risk of mortality with higher β-blockers doses, although the result was not statistically significant (Figure 4). To focus on the outcome effect of high-dose β-blockers, we additionally performed a sensitivity analysis comparing the clinical outcomes between patients with high-dose β-blockers and rest of the patients. As a results, no significant difference was observed associated with high-dose β-blockers (Supplementary Figure 3).
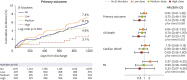
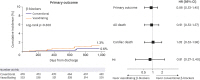
Figure 4
Clinical outcomes according to different doses of β-blockers.
After dose stratification, there was a dose-dependent tendency of lower risk of mortality with higher β-blockers doses, although the result was not statistically significant.
CI = confidence interval; HR = hazard ratio; MI = myocardial infarction.
![]()
When β-blockers were classified according to their vasodilating property, 553 (53.6%) patients received vasodilating β-blockers (Supplementary Table 2). Carvedilol and bisoprolol accounted for the most frequent type of vasodilating and conventional β-blockers, respectively. Vasodilating β-blockers was not associated with better clinical outcomes than conventional β-blockers (Figure 5). These results were consistent in patients with or without previous MI and/or revascularization or CHF and/or LV dysfunction (Supplementary Table 3).
DISCUSSION
The main findings of the current study are as follows: (1) β-blockers were not associated with better clinical outcomes in patients with chronic CAD undergoing PCI; (2) In subgroup of patients with previous MI and/or revascularization, β-blockers were associated with a lower risk of all-cause mortality; (3) No significant associations were found for the clinical outcomes with different doses and types of β-blockers.
β-blockers have long been considered one of the modalities for optimal medical therapy in patients with chronic CAD. However, the concept that β-blockers are beneficial for clinical outcomes in chronic CAD has mostly been extrapolated from evidence demonstrating the benefits of β-blockers in patients with AMI2)3)4) or HF with ventricular dysfunction.1)5)6) Several registry-based observational studies have evaluated the association between β-blocker therapy and clinical outcomes in patients with chronic CAD; however, the results are largely controversial.3)7)8)9) β-blockers have been associated with a significant reduction in mortality or cardiovascular events in chronic CAD patients with recent MI or HF.7)22) However, β-blocker therapy did not reduce cardiovascular mortality or morbidity in patients without prior MI or HF.3)8) Thus, in the current guidelines, β-blockers are mainly indicated for angina/ischemia relief in patients with chronic CAD, and are recommended for event prevention in patients with previous MI or HF.23) In line with the previous evidence, our study showed that the mortality benefit of β-blockers was found in subgroup of patients with previous MI and/or revascularization. It is noteworthy that previous studies categorized patient groups based on β-blocker use at a single time point, mostly at discharge, or on a few prescription records obtained after coronary revascularization. Therefore, the β-blocker group could include the patients with early termination of β-blocker therapy, resulting in potentially mixed findings. In the current study, we meticulously reviewed the medical records for β-blocker usage in each patient at 3-month intervals after discharge. Thus, we believe that our study could draw more conclusive findings regarding the effects of β-blocker therapy on chronic CAD patients undergoing PCI.
Current guidelines on chronic CAD suggest that the dose of β-blockers be adjusted to limit the heart rate to 55–60 beats per minute at rest.23) However, this recommendation lacks evidence and is solely based on registry data showing a positive correlation between heart rate and sudden death or mortality in the general population or patients with suspected or proven CAD.24) Theoretically, the dose of β-blockers adopted in pivotal randomized controlled trials should be fully targeted. However, as mentioned above, the potential benefits of β-blockers were extrapolated from the data analyzed in patients with AMI or HF. Furthermore, because of the inherent side effects of β-blockers, such as adverse hemodynamic or metabolic effects,25)26) substantially lower doses of β-blockers than the full target doses are widely adopted in real-world practice.27) Therefore, uncovering the dose effects of β-blockers is an interesting topic to be pursued in the field of cardiology. In this regard, some previous registry-based studies have shown no association between higher doses of β-blockers and better outcomes in patients with MI or chronic CAD.4)17) However, these studies relied solely on baseline β-blocker doses and did not consider their temporal changes. To overcome this critical limitation, we meticulously gathered the prescription data for β-blockers tri-monthly in each patient after discharge. In our previous study, we analyzed the impact of the β-blocker dose in patients with AMI after PCI.19) We found that medium-dose β-blockers were significantly associated with a lower risk of cardiac death compared to high- and low-dose β-blockers. We hypothesized that medium-dose β-blockers were just appropriate to avoid side effects of β-blockers, while maintaining their beneficial effects in patients with AMI, in whom hemodynamics could be potentially unstable. In the current study, however, such trend was not observed in patients with chronic CAD. The data showed a trend of dose-dependent reduction in mortality, although it was not statistically significant. One could surmise that the benefit of β-blocker therapy could be maximized with relatively low risk of side effects in chronic CAD contrast to AMI. Further large-sized randomized trials are warranted to confirm the dose-dependent effects of β-blockers on long-term clinical outcomes in chronic CAD.
β-blockers are not all the same and can be classified according to their vasodilating properties.27) Conventional β-blockers such as metoprolol, bisoprolol, or atenolol elevate central blood pressure and induce metabolic derangement,28) whereas vasodilating β-blockers such as carvedilol and nebivolol do not. These differences may explain the inferiority of atenolol to other antihypertensive agents with respect to outcome prevention, and the superiority of carvedilol to metoprolol in reducing adverse cardiovascular events in patients with chronic HF.5) In our previous study, we found that vasodilating β-blockers were associated with a lower risk of cardiac death compared to conventional β-blockers in patients with AMI or acute coronary syndrome.19)27)29) However, we observed that the clinical benefits of vasodilating β-blockers were not demonstrated in chronic CAD patients. We speculate that the adverse impact of conventional β-blockers on central blood pressure and metabolic derangement would be more prominent in patients with AMI than in chronic CAD patients.
The current study had some limitations. First, despite PS matching and multivariable adjustment, unmeasured confounders could exist between the patient groups because of the inherent nature of the registry data. Second, there could be some limitations in pooling the five different multicenter DES registries constituting the Grand-DES registry at the patient level. However, as the five registries were designed to share similar structures and were all hosted by Seoul National University Hospital, the confounding effect would be negligible. Third, data regarding clinical reasons in patients not receiving β-blockers were not available in the current database. Therefore, we could not provide the actual proportion of patients contraindicated to β-blockers in no treatment group. Fourth, we did not exclude patients in the main analysis whose β-blocker type had been changed during follow-up, which might have affected the clinical outcomes in β-blocker group. Fifth, the outcome data regarding the clinical symptoms were not available in the current database. Therefore, we could not analyze the anti-anginal effect of β-blockers in patients with chronic CAD after PCI. Finally, we excluded those patients whose prescription records of β-blockers were not available after PCI, which could induce a potential bias in the study results.
Overall, β-blocker therapy was not associated with better clinical outcomes in patients with chronic CAD who underwent PCI, regardless of prescribed doses and types of β-blockers. Limited mortality benefit of β-blockers may exist for patients with previous MI and/or revascularization.
 XML Download
XML Download