

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Atrial fibrillation (AF), the most common sustained arrhythmia among the general population,1)2)3)4) increases the risk of morbidity and mortality resulting from stroke, heart failure, and cognitive dysfunction, even among patients undergoing optimal anticoagulation and rate control therapy.5)6)7)8)9)10) Rhythm control, using antiarrhythmic drugs, electrical cardioversion, and AF ablation together with adequate rate control, is known to improve symptoms and quality of life in patients with symptomatic AF.11)12)13) No indication has been established for rhythm control therapy apart from improving AF-associated symptoms.1)12)13) Previous trials of rhythm control as compared with rate control in the 2000s, including the Atrial Fibrillation Follow-up Investigation of Sinus Rhythm Management (AFFIRM) and the RAte Control vs. Electrical Cardioversion for Persistent Atrial Fibrillation (RACE) trials, showed no significant differences between the treatment strategies in regard to mortality and cardiovascular outcomes.14)15)16)17) However, there were important treatment-related factors associated with mortality during rhythm control therapy at that time, such as the safety of rhythm control and the continuation of anticoagulation. Dronedarone reduced the composite outcome of death and cardiovascular hospitalizations compared with placebo for patients with AF and additional risk factors for death.18) In the previous 20 years, AF catheter ablation has been developed, and the Catheter Ablation vs. Antiarrhythmic Drug Therapy for Atrial Fibrillation (CABANA) trial confirmed the safety of AF ablation among contemporary AF patients with stroke risk.19) In AF patients with heart failure with reduced ejection fraction (HFrEF), AF catheter ablation improved outcomes compared with drug therapy combining rate control and antiarrhythmic drug therapy.20) Furthermore, long-term anticoagulation is generally maintained in contemporary patients with stroke risk after restoring the sinus rhythm using ablation.12)
The recently published Early Treatment of Atrial Fibrillation for Stroke Prevention Trial (EAST-AFNET 4) demonstrated that rhythm control therapy reduced the risk of a composite of death from cardiovascular causes, stroke, hospitalization owing to worsening heart failure, or acute coronary syndrome by 21% among patients recently diagnosed with AF (within 1 year after diagnosis).21) Here, we summarize the evidence supporting the use of rhythm control treatment among patients with AF, suggest the potential implications for indications, and shed light on clinical evidence gaps.
EFFICACY AND SAFETY OF RHYTHM CONTROL
Antiarrhythmic drug therapy
Table 1 summarizes the effects of rhythm control with contemporarily used antiarrhythmic drugs or catheter ablation on cardiovascular outcomes. There have been historical safety concerns of antiarrhythmic drug treatment.14)15) Amiodarone was associated with adverse outcomes among patients at high risk in non-randomized studies.22) Recent randomized trials found that the complication rates of drug treatment were similar to those of ablation therapy.19)23)24)25) In AF patients with heart failure, the risk of safety outcomes was similar between patients receiving amiodarone and rate control therapy.17) In the recent EAST-AFNET 4, there were no differences in the number of hospital stays and the risk of safety outcomes between the treatment strategies of rate control and rhythm control, which attenuates historical safety concerns.21) In the trial, 92% of rhythm-controlled patients underwent antiarrhythmic drug therapy initially, which replicated clinical practice patterns.
Table 1
Effects of contemporary rhythm control treatments compared to rate control in randomized controlled trials

| Variables | AF-CHF17) (2008) | ATHENA18) (2009) | Flec-SL26) (2012) | CTSN27) (2016) | EAST-AFNET 421) (2020) |
|---|---|---|---|---|---|
| Number of patients | 1,376 | 4,628 | 635 | 523 | 2,789 |
| Female sex (%) | 18 | 47 | 44 | 24.3 | 46.2 |
| Mean age (years) | 67 | 72 | 64 | 69 | 70 |
| Inclusion | Symptomatic HF (NYHA II–IV), LVEF <36% | AF and >70 years with one comorbidity or >75 years | Patients undergoing cardioversion | New-onset AF after cardiac surgery | Recent-onset AF (≤1 year before enrollment) with CV conditions (approximately ≥2 of CHA2DS2-VASc) |
| Type of AF | >2/3 persistent | NA | Persistent | Postoperative (persisted for more than 1 hour or recurrent AF within 7 days after surgery) | Persistent: 26.0% |
| Duration between AF diagnosis and enrolment (years) | <1 | NA | 2.3 | NA | 0.1 |
| Intervention for rhythm control | Amiodarone | Dronedarone | Flecainide for 4 weeks or 6 months | Amiodarone | Antiarrhythmic drugs or AF ablation |
| Comparator therapy | Rate control | Placebo | No antiarrhythmic drug treatment | Rhythm control | Usual care |
| Primary endpoint | CV death | CV hospitalization or death | Time to persistent AF or death | Days of hospitalization | A composite of CV death, stroke, hospitalization with worsening HF or ACS |
| SR maintenance | Amiodarone: 70% vs. Control: 30% at 2 years visit | Median time to first AF recurrence: 737 days (dronedarone) vs. 498 days (control) | Flecainide: 60% vs. Control: 40% at 6 months | Amiodarone: 97.9% vs. Control: 93.8% at 2 months | Rhythm control: 82.1% vs. Control: 60.5% at 2 years |
| Outcomes | No difference in mortality or QoL | Lower mortality and less hospitalizations in patients randomized to dronedarone | Lower mortality and recurrent AF at 4 weeks in patients randomized to flecainide | No difference in the numbers of days of hospitalization | Lower risk of the primary composite outcome in patients randomized to early rhythm control |
Dronedarone reduced cardiovascular deaths and cardiovascular hospitalizations compared to placebo.18) Flecainide reduced recurrent AF and all-cause death compared with no treatment following successful cardioversion in patients with persistent AF.26) By contrast, amiodarone failed to reduce death from cardiovascular causes in comparison with rate control for AF patients with HFrEF.17) Among patients with new-onset AF after cardiac surgery, amiodarone did not show a net clinical benefit over rate control.27)
Atrial fibrillation ablation therapy
Previous trials published more than a decade ago showed that AF ablation was better at maintaining sinus rhythm than antiarrhythmic drug treatment.28)29) A meta-analysis including 19 studies analyzing rhythm outcomes of at least 3 years after ablation revealed that the recurrence rate after a single procedure was approximately 47%.30) With multiple procedures, approximately 80% of patients were free from recurrent AF.30) In 20–50% of patients undergoing de novo AF ablation, redo ablation was performed.31) Dinshaw et al. reported that up to 90% and 60% of patients with paroxysmal and persistent AF undergoing ablation remained free from clinically relevant AF recurrences.32)
The CABANA trial confirmed the better efficacy of ablation therapy than antiarrhythmic drug treatment, although the primary composite outcome of death, disabling stroke, serious bleeding, or cardiac arrest did not differ with event rates of 8.0% and 9.2% in the ablation and drug therapy groups, respectively (p=0.30). The risk of AF recurrence was lower in the ablation group than in the antiarrhythmic drug group (hazard ratio [HR], 0.52; 95% confidence interval [CI], 0.45–0.60).19) A greater improvement in quality of life was observed in the ablation group than in the antiarrhythmic drug group.11) Rhythm control therapy was generally safe with low rates of complication in both treatment groups among the elderly study population (mean age: 68 years) of the CABANA trial. Periprocedural complications occurred in 4.8% of patients randomized to ablation, including tamponades (0.8%), hematomas (2.3%), and pseudoaneurysms (1.1%). In the arrhythmic drug therapy group, 0.8% and 1.6% of the patients experienced proarrhythmia and thyroid disorders, respectively.
The Early Aggressive Invasive Intervention for Atrial Fibrillation (EARLY-AF) and Cryoballoon Catheter Ablation in Antiarrhythmic Drug Naive Paroxysmal Atrial Fibrillation (STOP AF First) trials randomized 303 and 203 participants with symptomatic, untreated AF to early cryoballoon ablation or antiarrhythmic drug treatment, respectively.24)25) At 1-year follow-up with an implantable cardiac monitor in the EARLY-AF trial, the recurrence rates of atrial tachyarrhythmia were 42.9% and 67.8% in patients assigned to undergo ablation or to receive antiarrhythmic drugs, respectively.25) In the STOP AF First trial, 74.6% and 45.0% of the ablation and drug therapy groups were free from recurrence of atrial tachyarrhythmia.24) These results suggest that cryoballoon ablation as initial therapy provided a better efficacy of rhythm control than drug therapy among patients with paroxysmal AF.
Atrial fibrillation ablation therapy in patients with heart failure
Restoring and maintaining sinus rhythm has been used to improve the outcomes of AF patients with heart failure. However, use of antiarrhythmic drug therapy or the presence of sinus rhythm is not associated with better clinical outcomes for AF patients with HFrEF in large randomized controlled trials.17)33)34) Relatively small-sized trials reported that AF ablation improved left ventricular systolic function, exercise performance, and brain natriuretic peptide levels in AF patients with HFrEF.35)36)37)38)39)
The Catheter Ablation for Atrial Fibrillation with Heart Failure (CASTLE-AF) trial compared AF ablation with medical therapy, including antiarrhythmic drug treatment and rate control in AF patients with HFrEF (left ventricular ejection fraction [LVEF] <35%).20) Approximately one-third of the patients in the medical therapy group were on antiarrhythmic drug treatments at their final follow-up. Catheter ablation reduced the risk of a composite outcome of all-cause death or hospitalization owing to worsening heart failure by 48%. Twenty-two percent of patients assigned to medical therapy had sinus rhythm at 60 months. In contrast, 63% of the patients in the ablation group had sinus rhythm. These findings are consistent with the findings from a recent study analyzing routine patient data from the Korean National Health Insurance Service (NHIS) database.40) The beneficial association of AF ablation with hard clinical outcomes is consistently observed in the post-hoc analysis of the CABANA trial that included 778 (35%) participants in the New York Heart Association (NYHA) class at least II.41) However, most patients did not have a reduced LVEF. Only 9.3% of the patients for whom the ejection fraction was available had an ejection fraction of <40%. A sub-study of the CASTLE-AF trial reported that lower NYHA classes (I and II) were associated with more favorable clinical outcomes after ablation when compared with higher NYHA classes.42) The benefit of catheter ablation was consistently observed independent of LVEF (<20% vs. 20–34%). These results suggest that catheter ablation might be helpful in the early stages of heart failure symptoms irrespective of LVEF. Further investigations are needed regarding the selection of adequate heart failure patients for AF ablation and the clinical outcomes after AF ablation in patients with heart failure with a preserved ejection fraction.
OPTIMAL TIMING OF RHYTHM CONTROL FOR CARDIOVASCULAR BENEFIT
Early rhythm control and adverse cardiovascular outcomes in atrial fibrillation
AF itself causes adverse electrical and structural atrial remodeling, contributing to the progressive nature of arrhythmia.43) Such AF-related atrial remodeling develops within a few weeks of AF.44)45) Conceptually, early intervention to prevent the remodeling associated with AF might reduce the risk of adverse cardiovascular events. The recently published EAST-AFNET 4 aimed to test the hypothesis that rhythm control therapy initiated early after the AF diagnosis could reduce the risk of adverse events compared with the current practice of delayed rhythm control.46) Two thousand two hundred ninety-six patients with early AF (defined as AF diagnosed ≤1 year before enrollment) and underlying cardiovascular conditions (approximately a congestive heart failure, hypertension, age, diabetes mellitus, prior ischemic stroke or transient ischemic attack or thromboembolism, vascular disease, age, sex category [CHA2DS2-VASc] score ≥2) were enrolled at the 36 median days after AF diagnosis. Patients randomized to the early rhythm control were treated with antiarrhythmic medications (87%) or AF ablation (8%) at initials, and 19% of those patients underwent AF ablation at the 2-year follow-up. The primary outcome was a composite of cardiovascular death, stroke, hospitalization owing to worsening heart failure, or acute coronary syndrome. After the 5.1 years of median follow-up, early rhythm control treatment reduced the risk of the primary composite outcome by 21% compared with usual care (95% CI, 0.66–0.94).21) The absolute reduction of adverse cardiovascular outcomes was 1.1 per 100 patient-years. Among the individual outcomes of the composite outcome, early rhythm control reduced the risks of death from cardiovascular causes (HR, 0.72; 95% CI, 0.52–0.98) and stroke (HR, 0.65; 95% CI, 0.44–0.97).
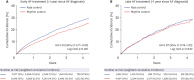
It is unclear whether the benefit of early rhythm control can be generalized to those in whom rhythm control is performed later after the AF diagnosis. Kim et al.47) investigated whether the results of rhythm control treatments depended on the duration between AF diagnosis and treatment initiation using a nationwide claim-based cohort comprising 22,635 AF adults on anticoagulant therapy in routine clinical practice. Among patients undergoing early AF treatment which was initiated within 1 year after diagnosis, compared with rate control, rhythm control was related to a 19% reduced risk of the primary composite end-point (absolute reduction 1.8 per 100 patient-years) (Figure 1A). However, this beneficial association was not observed in those who had AF for more than 1 year (Figure 1B).
Figure 1
Weighted cumulative incidence curves for individual components of the primary composite outcome in (A) early and (B) late atrial fibrillation treatments. Figure courtesy of Kim et al.47)
AF = atrial fibrillation; CI = confidence interval; HR = hazard ratio.
Safety of rhythm control according to the timing of treatment initiation
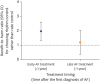
Rhythm control may be related to clinically significant serious adverse events (SAEs), and concerns regarding SAEs can serve as a barrier for performing rhythm control. Data on the prognostic effect of rhythm control therapy are heterogeneous, without a clear signal for either benefit or harm.31) Kim et al.47) exploited a predictive model to determine the benefit-to-harm ratio of rhythm control compared to rate control. The benefit-to-harm ratio of rhythm control compared with rate control was over one within 1 year after AF diagnosis, suggesting that patients with early rhythm control would benefit than harm (Figure 2A). The benefit-to-harm ratio was decreased to under one when initiating rhythm control treatment later (Figure 2B).48)
Figure 2
Benefit-to-harm ratios of rhythm control compared with rate control according treatment timing. The ratios >1 indicate positive net benefit. Figure courtesy of Kim et al.47)
AF = atrial fibrillation; CI = confidence interval.
Optimal treatment timing for better cardiovascular outcomes
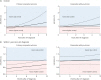
Kim et al.47) explored questions about the optimal timing for initiating rhythm control in overall periods beyond the enrollment criteria of EAST-AFNET 4. There was a linearly increasing relationship between rhythm control and worse cardiovascular outcomes with later timing of treatment initiation compared with rate control (Figure 3). Rhythm control was associated with a lower risk of the primary composite outcome when initiated earlier timing after AF diagnosis compared to rate control whereas the HR exceeded one between the treatment timing at 1 and 2 years after AF diagnosis (Figure 3A). Within 1 year since the diagnosis of AF, more earlier treatment timing of rhythm control showed a more favorable outcome relative to rate control (Figure 3B). In contrast, the risk of safety outcomes was not different between the rhythm and rate control treatments, regardless of the treatment timing (Figure 3A and B).
Figure 3
Relation between treatment timing and risk of clinical outcomes for rhythm control or rate control in (A) overall period and (B) within 1 year after the first diagnosis of AF. Figure courtesy of Kim et al.47)
The x-axis shows the timing of treatment initiation since the first diagnosis of AF; the y-axis, HRs associated with rhythm control compared with rate control. The black horizontal lines indicate HR=1, which corresponds to an equal risk of outcomes in patients treated with rhythm and rate control. Dashed black lines show the 95% CI.
AF = atrial fibrillation; CI = confidence interval; HR = hazard ratio.
Early rhythm control and individual outcomes
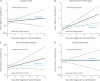
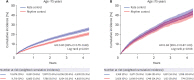
Conceptually, a reduced AF burden may reduce the risk of AF-related adverse cardiovascular outcomes including stroke, heart failure, and myocardial infarction.49)50) However, how early rhythm control should be initiated and for which outcomes we benefit from early rhythm control are unknown. Kim et al.47) recently reported that early rhythm control may reduce the risks of stroke and hospitalization due to heart failure compared with rate control using the Korean NHIS database. They further investigated comparative efficacy of rhythm control versus rate control for reducing individual adverse outcomes stratified by the treatment timing.48) Compared with rate control, rhythm control initiated within 1 year of AF diagnosis decreased the risk of stroke (Figure 4A). The HRs of stroke for rhythm control initiated at selected timings after AF diagnosis were as follows: HR 0.76 at 6 months, HR 0.78 at 1 year, HR 1.00 at 5 years. This result is consistent with that of a post-hoc study of the Placebo-controlled, Double-blind, Parallel Arm Trial to Assess the Efficacy of Dronedarone 400 mg BID for the Prevention of Cardiovascular Hospitalization or Death from any Cause in Patients with AF/Atrial Flutter (ATHENA) trial, which demonstrated that dronedarone treatment reduced the risk of ischemic and hemorrhagic stroke compared with placebo.18) Two observational studies revealed that rhythm control with antiarrhythmic drugs or catheter ablation was associated with a lower risk of stroke/transient ischemic attack compared with rate control.50)51) The rhythm control performed within 6 months of AF diagnosis was associated with a reduced risk of hospitalization due to heart failure: HR 0.84 at 6 months, HR 0.96 at 1 year, HR 2.88 at 5 years (Figure 4B). There were no differences in the risks of myocardial infarction and death from cardiovascular causes between the strategies of rhythm and rate control, irrespective of the treatment timing (Figure 4C and D).
Figure 4
Relation between treatment timing and risk of ischemic stroke (A), hospitalization owing to heart failure (B), acute myocardial infarction (C), and cardiovascular death (D) for rhythm control or rate control. Figure courtesy of Kim et al.48)
The x-axis shows the timing of treatment initiation since the first diagnosis of atrial fibrillation; the y axis, HRs associated with rhythm control compared with rate control. The skyblue horizontal dotted lines indicate HR=1, which corresponds to an equal risk of outcomes in patients treated with rhythm and rate control. Dashed black lines show the 95% CI.
CI = confidence interval; HR = hazard ratio.
OPTIMAL PATIENT SELECTION FOR EARLY RHYTHM CONTROL
Age and the effects of rhythm control
Whether the beneficial effects of early rhythm control can be generalized to older adults is unclear. A subgroup analysis of the AFFIRM trial showed a reduction in mortality associated with rate control than rhythm among those aged between 65 and 80 years.15) Shariff et al.52) performed a propensity score-matched study of the AFFIRM trial participants aged 70–80 years to investigate the comparative effect of rate versus rhythm control strategies on outcomes. They suggested that rate controlled patients were at lower risks of mortality and hospitalization than those with rhythm control among septuagenarians with AF.52) Although there is no specific age discrimination determining the treatment options of rhythm or rate control, including cardioversion and AF catheter ablation in the current guidelines,12)53) age is an independent predictor of procedure-related complications, AF recurrence, adverse cardiac outcomes in patients undergoing ablation procedures.54)55)56)
Kim et al.57) studied whether the benefits from early rhythm control differed with age. There was a linear decrease of the protective effects of early rhythm control over rate control on adverse cardiovascular outcomes with age (Figure 5). A significant interaction between age and early rhythm control was observed at 75 years (p=0.045). Compared with rate control, early rhythm control was associated with a 20% reduced risk of the composite outcome of death from cardiovascular causes, stroke, heart failure-related admission, or myocardial infarction in patients aged <75 years (Figure 6A) but not in patients aged ≥75 years (Figure 6B). This result suggests that early initiation of rhythm control can be adopted preferentially, especially in patients with AF aged <75 years.
Figure 5
Relationship between age at treatment initiation and the risk of the primary composite outcome in early rhythm control and rate control groups. Figure courtesy of Kim et al.57)
The x-axis shows the age at treatment initiation and the y-axis shows HRs associated with rhythm control when compared with rate control. The purple horizontal line indicates HR=1, which corresponds to an equal risk of outcomes in patients treated with rhythm control and rate control. The dashed black lines indicate the 95% CI.
CI = confidence interval; HR = hazard ratio.
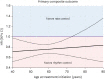
Figure 6
Weighted cumulative incidence curves for the primary composite outcome in patients aged <75 years (A) and ≥75 years (B) who were recently (within 1 year) diagnosed with atrial fibrillation. Figure courtesy of Kim et al.57)
CI = confidence interval; HR = hazard ratio.
The association between the effects of rhythm control and the CHA2DS2-VASc score
The EAST-AFNET 4 included patients with early AF and a CHA2DS2-VASc score of approximately ≥2. We compared the effect of early rhythm control on adverse cardiovascular outcomes between eligible and ineligible patients (CHA2DS2-VASc approximately 0–1) for EAST-AFNET 4 using a nationwide claim database of routine clinical practice to investigate whether the results can be generalized for patients with low stroke risk. Of the included 54,216 participants, 69.3% were eligible for the EAST-AFNET 4 trial (median age: 70 years, median CHA2DS2-VASc: 4), among whom early rhythm control reduced the risk of the primary composite outcome than rate control (HR, 0.86; 95% CI, 0.81–0.92). Among the patients with low risk (30.7%) who failed to meet the inclusion criteria (median age: 54 years, median CHA2DS2-VASc: 1), early rhythm control was consistently associated with a reduced risk of the primary composite outcome (HR, 0.80; 95% CI, 0.66–0.97) (Unpublished data). In routine clinical practice, the beneficial association between early rhythm control and cardiovascular complications was consistent among low-risk patients, regardless of trial eligibility.
The association between the effects of rhythm control and frailty
Frailty is a state of vulnerability defined as an age-associated decline in physiological reserve and function across multiple organ systems, leading to an increasing hazard of adverse outcomes, especially in the elderly.58)59) Frailty is important for estimating risks and aiding diagnosis and care planning in older patients.60) However, it is unclear whether the results of the rate versus rhythm control trials can be generalized for frail elderly adults. We evaluated whether frailty affected the outcomes of early rhythm control in older patients. Although the beneficial association between early rhythm control and cardiovascular outcomes was attenuated with increasing frailty, early rhythm control showed consistent trends toward a lower risk of adverse cardiovascular outcomes without an increased risk of safety outcomes across the different frailty groups (Unpublished data).
The association between the effects of rhythm control and symptom status
In current guidelines, rhythm control therapy is restrictively recommended only among patients with symptomatic AF. In the EAST-AFNET 4, 30% of the patients were asymptomatic at enrollment.21) A similar proportion has been observed in other trials and registries, such as the AFFIRM trial and Global Anticoagulant Registry in the FIELD-Atrial Fibrillation (GARFIELD-AF) and Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF) registries.15)61)62) Recently, Willems et al.63) showed that the benefit of early rhythm control was consistently observed regardless of symptom status in the participants of the EAST-AFNET.
RHYTHM CONTROL AND PREVENTION OF DEMENTIA
Data on the efficacy of various treatments for preventing cognitive decline among patients with AF are unclear. In patients with incident AF, oral anticoagulant use was associated with a 39% lower incidence of dementia.9) Interestingly, Kim et al. reported that compared with warfarin users, direct oral anticoagulant users were at a 22% lower risk of dementia.10) Integrated AF management controlling risk factors was also shown to be associated with a lower risk of dementia.64)65)66)67)
Association of a rhythm control strategy and dementia risk
The effect of rhythm control treatment for AF on cognitive outcomes has been unclear.67)68) A sub-analysis of the AFFIRM trial reported no difference in cognitive function between treatment strategies of rate or rhythm control.69) However, several observational investigations have suggested that AF ablation may improve cognitive function and reduce dementia risk.70)71)72)73)
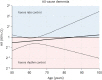
Recently, Kim et al.74) compared subsequent dementia risk between rhythm control (antiarrhythmic drugs or ablation) and rate control treatment using a Korean nationwide cohort including 41,135 AF participants on anticoagulant therapy. Rhythm control was associated with a 14% lower risk of all-cause dementia, irrespective of overt stroke (absolute reduction 4.0 per 1,000 patient-years) (Figure 7). The beneficial effect of rhythm control on the risk of dementia decreased linearly with increasing age (Figure 8). Performing rhythm control in patients aged under 80 years showed a reduced dementia risk compared with rate control. The protective association between rhythm control and dementia risk was also pronounced in those without heart failure and those with lower CHA2DS2-VASc scores. These results suggest that rhythm control in those with fewer risk factors may help minimize the risk of dementia.
Figure 7
Weighted cumulative incidence curves for all-cause dementia in (A) overall and (B) after censoring stroke. Figure courtesy of Kim et al.74)
CI = confidence interval; sHR = subdistribution hazard ratio.
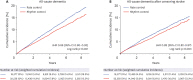
Figure 8
Relation between age at treatment initiation and risk of dementia for rhythm control or rate control. Figure courtesy of Kim et al.74)
The x-axis shows the age at the time of treatment initiation; the y-axis, HR associated with rhythm control compared with rate control. The purple horizontal line indicates HR=1, which corresponds to an equal risk of outcomes in patients treated with rhythm and rate control. Dashed black lines show the 95% CI.
CI = confidence interval; HR = hazard ratio.
CONCLUSIONS
The safety of rhythm control treatment has been confirmed in recent randomized trials, including CASTLE-AF, CABANA, and EAST-AFNET 4 and observational studies. Initiating rhythm control early after AF diagnosis was shown to reduce the risk of adverse cardiovascular events compared with rate control; however, this effect of rhythm control was not shown among patients who had AF for more than 1 year. Within 1 year after AF diagnosis, performing rhythm control as early as possible might result in more favorable outcomes, especially in reducing the risks of stroke and hospitalization owing to heart failure. The favorable effects of rhythm control versus rate control were observed irrespective of the estimated stroke risk, frailty, or the symptoms of AF and were more prominent in younger age groups. Furthermore, rhythm control might help prevent dementia incidence compared to rate control, especially for younger AF patients with fewer risk factors. Therefore, rhythm control should be considered at the earliest stage and at a younger age, regardless of the existence of AF-related symptoms.
 XML Download
XML Download