

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Contrast-associated acute kidney injury (CA-AKI) is defined as deterioration in the kidney function that is associated with administration of contrast medium. CA-AKI is a common cause of hospital-acquired AKI and is associated with prolonged hospital stay and increased morbidity and mortality.1)2)3) The reported incidence of CA-AKI ranges from <1% to >50% depending on comorbidities, type of procedures, and definition of CA-AKI.3)4)5) Diagnostic and interventional cardiac procedures that require intravascular contrast are increasingly used in the elderly who are most susceptible to CA-AKI due to comorbidities that are common in advanced age, including chronic kidney disease (CKD).
The same risk factors for CA-AKI also predict the presence of complex coronary artery disease, and unfortunately due to risk aversion by patients or operators to avoid CA-AKI and the need for renal replacement therapy, diagnostic angiography and percutaneous coronary interventions (PCIs) are significantly underutilized in patients with CKD – i.e., indicating the so called concept of “renalism,” the hesitation to perform clinically indicated procedures due to the risk of inducing AKI and the need for renal replacement therapy.6) Reducing the dependance of operators on contrast usage in patients at risk of CA-AKI is key in improving the results of PCI, as typically many of these interventions must be performed in calcific vessels and in complex anatomical subsets like bifurcation lesions, left main or chronic coronary occlusions.
In this thematic review, we provide a brief overview on pre-procedural assessment of the risk for CA-AKI and strategies for prevention and management of CA-AKI that is precipitated by interventional cardiac procedures.
CONTRAST-ASSOCIATED ACUTE KIDNEY INJURY – DEFINITION AND RISK FACTORS
It is not always possible to attribute contrast-induced nephropathy as the definite cause of AKI in patients who undergo cardiovascular procedures during which contrast media are used7) as other factors such as hemodynamic instability and atheroembolism may also play a role. The Kidney Disease Improving Global Outcomes (KDIGO) initiative defines CA-AKI if one of the following occurs within 48 hours after intravascular administration of contrast: 1) absolute increase in serum creatinine (Cr) ≥0.3 mg/dL (≥26.4 μmol/L), 2) relative increase in Cr ≥50% (≥1.5 times baseline), or 3) urinary volume <0.5 mL/kg/h for ≥6 h.7) The decline in kidney function usually occurs 2–3 days after exposure to contrast and returns to the baseline level within 1–2 weeks.8) Nevertheless, other definitions for AKI after contrast administration have also been used in studies.9)10) Therefore, the incidence of CA-AKI reported in the clinical studies should be interpreted while considering the specific definition used.
The risk factors for CA-AKI include baseline CKD, diabetes, volume depletion and age.11) Contrast agents can affect kidney function through several mechanisms. In patients with pre-existing CKD, the cytotoxicity of contrast agents on renal tubular and vascular endothelial cells may play a role as contrast agents worsen renal hypoperfusion and hypoxia.12) In volume depleted patients, the kidneys might primarily be impacted by rheological effects of contrast media, which perturb tubular dynamics and renal hemodynamics.12) Oxidative stress and endothelial dysfunction are also associated with an increased risk of CA-AKI.12)
Additionally, type, volume, route of contrast, and repetitive contrast administration within a short period of time (24–72 hours) increase the risk of CA-AKI.12) Contrast volume is a risk factor for CA-AKI, especially during coronary angiography.13) Although there is no specific safe threshold for contrast volume, the European Society of Urogenital Radiology (ESUR) guideline suggests limiting the ratio of contrast dose (in grams of iodine) over absolute estimated glomerular filtration rate (eGFR) (in mL/min) to <1.1 or the ratio contrast of contrast volume (in mL) over eGFR (in mL/min/1.73 m2) to <3.0 when using a contrast medium concentration of 350 mg/mL for intraarterial administration.8) Ultra-low contrast volume, defined as contrast volume equalling or less than the patient’s estimated Cr clearance and applied in 9857 patients undergoing PCI was associated with a significant reduction in AKI, particularly in high-risk patients.14)
PREVENTION AND MANAGEMENT OF CONTRAST-ASSOCIATED ACUTE KIDNEY INJURY
Several risk scores integrating clinical and procedural variables have been proposed that integrate clinical and procedural variables.11)15)16) These risk scoring systems have been tested for their ability to predict CA-AKI, procedure-related mortality, and major adverse clinical events in patients undergoing angiography or PCI, nevertheless further validations are warranted before these risk scores could be routinely used in clinical practice.
Baseline CKD is a key risk factor for CA-AKI that increases the likelihood of CA-AKI and its impact on major adverse outcomes. In a post-hoc analysis of the Assessment of Dual AntiPlatelet Therapy With Drug Eluting Stents (ADAPT-DES) registry that included 7,287 participants who underwent PCI, 6.5% of patients developed CA-AKI, which was associated with significantly higher risk of adverse clinical outcomes, including all-cause and cardiovascular mortality, during a median follow-up of 2 years.17) While patients without CKD who developed CA-AKI post-PCI had higher rates of adverse outcomes compared with patients who did not, the relative risk was highest in the group with CA-AKI that complicated pre-existing CKD. Compared with the CA-AKI–/CKD– group, the CA-AKI+/CKD– (1.83 [1.33–2.52]), CA-AKI–/CKD+ (1.56 [1.15–2.13]), CA-AKI+/CKD+ (3.29 [1.92–5.67]), and maintenance dialysis (2.67 [1.65–4.31]) groups were at higher risk of net adverse clinical events (all-cause mortality, myocardial infarction, definite/probable stent thrombosis, or major bleeding).17)
Withholding medications which may potentially increase the risk of CA-AKI in theory may be useful to decrease this risk.8) However, there is inconclusive evidence for impact of medications such as angiotensin converting enzyme inhibitors/angiotensin receptor blockers and is not recommended in the current guidelines.8)18)
It is firmly established that intravenous volume repletion (or “hydration” as more commonly used and which we will use herein) reduces the incidence of CA-AKI. By expanding plasma volume, hydration decreases contrast concentration and increases kidney blood flow and tubular urine flow, which reduce contrast retention and thereby its direct toxic effect on the tubules.8)
The POSEIDON (Prevention of Contrast Renal Injury with Different Hydration Strategies) trial compared left ventricular end-diastolic pressure (LVEDP)-guided hydration with standard hydration in 396 patients undergoing cardiac catheterization.19) All patients received a bolus infusion of normal saline (3 mL/kg) for one hour prior to the procedure. During and for four hours after the procedure, the LVEDP-guided group received normal saline at a rate of 1.5 to 5 mL/kg/h, depending on the LVEDP, and the control group at 1.5 mL/kg/h. The total hydration volume was higher in the LVEDP-guided group (mean volume, 1,727 mL versus 812 mL, p<0.001), with significantly lower rate of CA-AKI (6.7% vs. 16.3%, p=0.005). The odds of CA-AKI decreased by 9% for every additional 100 mL of normal saline administered (odds ratio, 0.91; 95% confidence interval [CI], 0.89–0.94; p=0.01). The 30-day composite endpoint of major adverse events was numerically lower in the LVEDP-guided hydration arm (1.0% vs. 4%, p=0.11). Need for dialysis at 6 months was similar (0.5% vs. 2.0%, p=0.37). Intravenous hydration had to be terminated due to shortness of breath in three patients in each arm, and two patients required administration of an intravenous diuretic. It should be noted that the mean baseline serum Cr was 1.4 mg/dL with a mean eGFR of 47.5 mL/min. While the benefits of intravenous hydration can probably be extrapolated to more advanced stages of CKD (stages 4 and 5), further studies are needed to establish whether hydration alone would have a similar impact on the rates of CA-AKI in this higher risk group of patients.
MINIMIZING CONTRAST VOLUME: ULTRA-LOW CONTRAST ANGIOGRAPHY AND ZERO CONTRAST PERCUTANEOUS CORONARY INTERVENTION
Minimizing the contrast volume and using the least nephrotoxic contrast are paramount in angiography and PCI, and multiple exposure especially within a short period of time (24–72 hours) can increase the risk of CA-AKI8) and should be avoided.
We have described the technical details of “ultra-low” contrast angiography (Figures 1 and 2) in which, in addition to LVEDP-guided intraprocedural hydration, the contrast volume is restricted to a maximum volume that is determined by a contrast volume/eGFR ratio <1.21) Contrast volume/eGFR is a validated measure of systemic exposure to radiocontrast, with contrast volume/eGFR >1 exponentially increasing the risk of CA-AKI in late-stage CKD.22) During ultra-low contrast angiography, injection of heparinized saline to coronary arteries to induce repolarization changes on ECG monitoring or placement of a workhorse coronary guidewire (rather than “test” contrast injections) is used to confirm catheter engagement. Meticulous techniques are used to minimize the contrast administered in a limited number of angiographic projections (Figures 2 and 3), both in native CAD21) and graft conduits.23) When angiographically ambiguous lesions are present, adjunctive tests such as coronary physiology are used to further assess the lesion severity without using additional contrast (Figure 4). In a single-center, non-randomized, and propensity-matched observational cohort, ultra-low contrast angiography reduced the risk of CA-AKI and need for renal replacement therapy compared with standard angiography in late-stage CKD during a 24-month follow-up period.24)
Figure 1
Pathway for ultra-low contrast angiography and ultra-low or zero-contrast percutaneous intervention.
ACS = acute coronary syndrome; AP = antero-posterior; CA-AKI = contrast-associated acute kidney injury; CCS = chronic coronary syndrome; CV = contrast volume; DES = drug-eluting stent; DM = diabetes mellitus; EKG = electrocardiogram; GFR = glomerular filtration rate; LAO = left anterior oblique; LCA = left coronary artery; LVEDP = left ventricular end-diastolic pressure; MAX = Medial dissection, Apposition, eXpansion; MLD = Morphology, Length, Diameter ; PCI = percutaneous coronary intervention.

Figure 2
Ultra-low contrast angiography in a patient with advanced chronic kidney disease (stage 5, estimated glomerular filtration rate 13 mL/min). (A) Radial access is avoided so that the radial artery is preserved for access for hemodialysis in the near future. Femoral access is performed using a combination of ultrasound to mark the common femoral bifurcation, a hemostat to mark the mid-femoral head using the micropuncture kit to gain access. (B) The left ventricular end diastolic pressure is measured to guide intravenous hydration. (C) Intracoronary injection of 10 mL of 0.9% heparinized normal saline. If the catheter is engaged, transient EKG changes will occur. Single view, low-magnification, non-panned angiograms of the right (LAO-cranial), circumflex (AP-caudal), and left anterior descending coronary arteries (AP-cranial) are obtained. Total contrast volume was 9.6 mL.
AP = antero-posterior; LAO = left anterior oblique.

Figure 3
Ultra-low contrast angiography with adjunctive coronary physiology to resolve diagnostic ambiguity. (A) A patient with advanced chronic kidney disease (stage 5, estimated glomerular filtration rate 8 mL/min) undergoes ultra-low contrast angiography with contrast dilution, which suggests an ambiguous lesion in the proximal circumflex coronary artery (arrow). (B-C) Invasive coronary physiology is performed, without contrast-guidance, which excludes significant ischemia, with resting full-cycle ratio of 0.94.
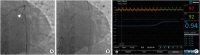
Figure 4
Zero contrast percutaneous coronary intervention in a patient with advanced chronic kidney disease. (A) A road map from a previously performed ultralow contrast angiogram of the RCA with 3 mL contrast in the AP cranial view is projected. (B) Spot iFR of the distal vessel confirms significant ischemia (iFR 0.67). (C) Co-registration of iFR pullback with the angiographic silhouette of the guidewire reveals a focal flow-limiting stenosis in the mid RCA segment, while confirming that the proximal lesion (A*) is non-ischemic. (D) A reference segment distal to the lesion is identified manually and marked with cine angiography. (E) By co-registering the intravascular ultrasound system pullback with the guidewire, reference vessel measurements are performed at the distal reference segment, revealing a mean distal vessel size of 3.1 mm. (F) Following the same approach, a proximal, disease-free segment is identified, the length of lesion measured from the distal reference to this segment (yellow line) is 33.7 mm and mean proximal vessel size is 3.7 mm. (G-I) The stent is then deployed using co-registration, which may be automated (G), or manual (H), where the distal stent marker is aligned to the intravascular ultrasound transducer and a 3.0 mm by 33 mm drug eluting stent is deployed. (J) Using the advanced fluoroscopic device detection, the distal segment of stent is post-dilated pre-emptively with a 3.0 mm non-compliant balloon while avoiding the distal edge of the stent, and (K) the proximal segment of the stent with a 3.5 mm non-compliant balloon. (L) Stent expansion is assessed by measuring the manually identified minimal stent area (7.2 mm2) and comparing it with (M) the distal reference area (7.1 mm2), confirming >100% expansion. The distal and proximal stent edge were free of dissection (not shown). (N) A final spot iFR measurement confirms resolution of ischemia with pullback (O) confirming no need for further intra-stent optimization.
AP = antero-posterior; iFR = instantaneous flow ratio; RCA = right coronary artery.

Ultra-low or “zero contrast” PCI21) is a strategy for PCI using minimal or no contrast in late-stage CKD, where the procedure is guided entirely by using intravascular imaging and physiology. In chronic coronary syndromes this is done using previously performed ultra-low contrast angiography (Figure 1), however in acute coronary syndromes this approach may not be possible. Staging the procedure allows for reduction in the total contrast exposure, recovery of kidney function, and discussion of the risks and benefits of zero contrast PCI with the patient. During zero contrast PCI, prior diagnostic angiograms are displayed and used as a roadmap for guide catheter engagement and guidewires advancement, whose tips are looped whenever possible to decrease the chances of distal vessel perforation.
Use of several guidewires is recommended to generate a metallic silhouette or skeleton of the target vessel and its branches (Figure 4). The procedure is then guided by intravascular physiology and imaging (ultrasound21) or optical coherence tomography with saline flush25)). Co-registration of physiology and intracoronary imaging pullback with the wire silhouette allows contrast-free localization of flow-limiting stenoses, identifying vessel segments that require plaque preparation, selecting stent landing zones and choosing stent size and length. After stent implantation, the same approach can be followed to verify the results of PCI or to guide optimization, also with the use of stent enhancement tools, all without the need for contrast injection (Figure 4). Pre-specified criteria indicating procedural complications or suboptimal results are devised to guide the use of contrast to perform angiography during zero-contrast procedures, if indicated (Figure 1).21)
A valuable digital tool in performing ultra-low contrast PCI, particularly during acute coronary syndromes, is dynamic coronary road-mapping (Philips, Amsterdam, The Netherlands). The system generates dynamic templates of the coronary vessels which are subsequently displayed over the fluoroscopy, allowing wiring and positioning of PCI devices without additional contrast injections (Figure 5). The value of dynamic coronary road-mapping to spare contrast and to increase the safety of PCI is currently being tested in a randomized trial (NCT04085614)
Figure 5
Techniques to increase safety of ultra-low or zero contrast percutaneous coronary intervention. (A) Baseline coronary angiogram. (B) Workhorse guide wires are bent at the tip with exaggerated curves to promote knuckling of the wire (white circles) and protect against distal wire perforation. (C) Dynamic coronary roadmap, a real-time, motion-compensated navigation system, can help prevent inadvertent wire passage into small vessels, which may track along the same course as the target vessel.

An initial report in 35 patients with eGFR 16±8 mL/min/1.73m2 supported the feasibility and safety of zero contrast PCI, resulting in preserved post-procedural kidney function in all patients and no need for renal replacement therapy.21) A prospective, single-center, propensity matched comparison with standard angiography alone showed that combined ultra-low contrast angiography and zero-contrast PCI was associated with significant reduction in the rates of renal replacement therapy within a 12-month follow-up period (hazard ratio, 0.40; 95% CI, 0.21–0.75; p=0.0032).26) Given the frequent presence of severe calcification, atherectomy may be needed during the zero contrast PCI to modify the fibrocalcific plaques and optimize PCI results.27) The recent advent of intravascular lithotripsy, which is a balloon catheter-based technique, may simplify calcific plaque modification as part of zero contrast PCI.28) The feasibility of zero contrast PCI has also been shown in complex lesions (such as chronic total occlusions29) and high-risk PCI with hemodynamic support30) or in vein grafts31)). Randomized studies are warranted to further establish the role of ultra-low contrast angiography and zero contrast PCI as part of the invasive management strategy for coronary artery disease in late-stage CKD.
CONCLUSIONS
Patients at the risk of CA-AKI should be carefully assessed before cardiovascular procedures that involve using contrast media. Patients with multiple risk factors, especially those with baseline CKD, heart failure, and diabetes are at a particularly high risk of CA-AKI. Various risk scores have been proposed and tested but their routine use is hampered by inadequate validation.
At present, intravenous hydration is the only evidence-based strategy for prevention of CA-AKI and normal saline is the preferred solution. Since patients with advanced CKD, particularly those in stage 5 CKD who are not on maintenance dialysis, may have fluid retention, intravenous hydration is best initiated during the procedure after the LVEDP is measured.
Principles of ultra-low contrast angiography and staged zero contrast PCI have been described and widely adopted by interventional cardiologists. Interventionalists ought to learn the techniques, in particular the use of intravascular imaging, to perform PCI safely and effectively in patients with advanced CKD without compromising the residual kidney function.
 XML Download
XML Download