

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Coronavirus disease 2019 (COVID-19) is caused by severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2). Its severity spectrum in children and adolescents ranges from asymptomatic to life-threatening. There have been rare cases of COVID-19-related pediatric deaths or long-term pulmonary complications.1234
Postinfectious bronchiolitis obliterans (PIBO) is a chronic, irreversible, obstructive lung disease following severe lower respiratory-tract injury, especially during early childhood.56 SARS-CoV-2 can cause severe lower respiratory-tract inflammation. Therefore, PIBO is possible after COVID-19. There are a few reports of pediatric PIBO, with most patients being < 3 years old.789 However, there are no reports of pediatric PIBO developing after COVID-19 in the Korean population. Here, we report the case of a 10-year-old boy who developed PIBO after recovering from SARS-CoV-2-related pneumonia.
CASE DESCRIPTION
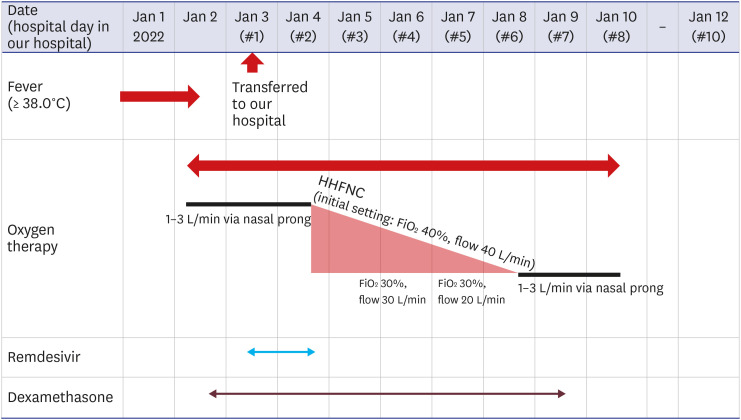
On January 3, 2022, a 10-year-old boy with COVID-19 was referred to our hospital. Approximately 1 month before his COVID-19 diagnosis, he was treated at a local hospital for respiratory symptoms of cough, sputum, and rhinorrhea, without dyspnea. At that time, rapid antigen SARS-CoV-2 testing, reverse transcriptase polymerase chain reaction (RT-PCR) for Mycoplasma pneumoniae (MP), and RT-PCR for multiplex respiratory virus (adenovirus, coronavirus NL63/229E/OC43, human metapneumovirus, human rhinovirus A–C, influenza A/B, parainfluenza 1–3, respiratory syncytial virus, boca virus) were performed; no respiratory pathogens were detected. On December 29, 2021, he developed a fever of 38°C. Although he had no close contact with anyone with COVID-19, on January 1, 2022, he was diagnosed with COVID-19 through an RT-PCR assay of an upper-respiratory-tract sample. From the day after diagnosis, the fever subsided. However, he developed dyspnea and started receiving oxygen therapy. His condition worsened, and he was transferred to our hospital on January 3, 2022. Fig. 1 shows the timeline of the clinical course and treatment. The initial vital signs at our hospital were: heart rate, 92/min; blood pressure, 117/78 mmHg; respiratory rate (RR), 22/min; oxygen saturation, 93% (oxygen, 1 L/min via nasal prong); and body temperature, 36.5°C. He exhibited intercostal retractions but crackling and wheezing were not definite on auscultation. The initial laboratory results were 1) white blood cell count, 4,490/μL (19.2% lymphocytes); 2) hemoglobin, 14.7 g/dL; 3) platelet count, 213,000/μL; 4) C-reactive protein, 3.30 mg/dL (range, 0–0.5); 5) D-dimer, 1.29 μg/mL (range, 0–0.5); and 6) interleukin (IL)-6, 10.6 pg/mL (range, 0–7.0). Cardiac biomarkers were normal. Venous blood gas analysis results were 1) pH, 7.431; 2) pCO2, 34.1 mmHg; 3) pO2, 70.0 mmHg; and 4) O2 saturation, 94.7%.
Fig. 1
Timeline of clinical course and treatment.
HHFNC = humidified high flow nasal cannula, FiO2 = fraction of inspired oxygen.
The patient was born healthy without oxygen demand to a 33-year-old mother at 35 weeks through cesarean delivery, with a birth weight of 1,850 g (6th percentile) and a monozygotic twin brother weighing 2,050 g (15th percentile). Perinatally, he had no specific respiratory disease, e.g., bronchopulmonary dysplasia or respiratory distress syndrome. He was previously healthy except for allergic rhinitis and had no specific medical history of other allergies, including recurrent wheeze and asthma. He never before had severe pneumonia requiring oxygen therapy. However, he was obese (body mass index [BMI], 30.13, 99.9th percentile; body weight, 66 kg, 99.7th percentile; height, 148 cm, 80.2th percentile). To determine the cause of obesity, thyroid-stimulating hormone, free thyroxine, insulin, adrenocorticotropic hormone, hemoglobin A1c, and lipid profile tests were performed, producing no specific findings. Two days after his diagnosis, his brother was also diagnosed with COVID-19. His brother was also previously healthy but obese (BMI, 27.2, 99.5th percentile; body weight, 62 kg, 99.2th percentile; height, 151 cm, 90.6th percentile). Table 1 compares the medical history and clinical symptoms post COVID-19 between the patient and his brother.
Table 1
Comparison between the patient and his twin brother
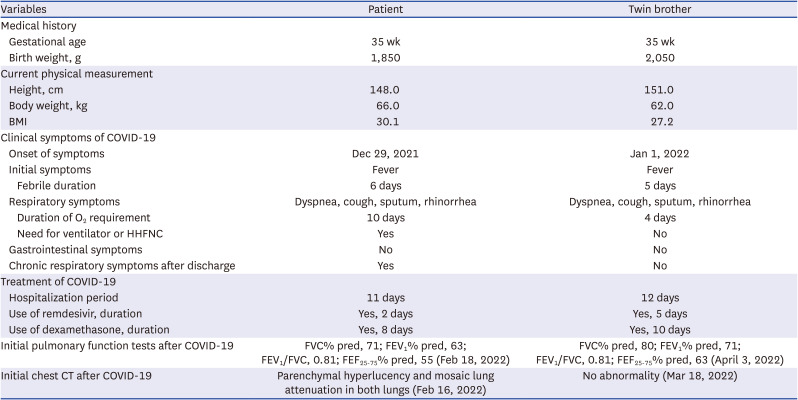
Fig. 2 presents serial chest radiographs of the patient. The initial chest posteroanterior view showed bilateral patchy, confluent, ground-glass opacity and consolidation in the mid to lower lung zones (Fig. 2A). Remdesivir (1st day, 200 mg; 2nd day, 100 mg) and dexamethasone (6 mg, once a day) were administered intravenously on the 1st day of hospitalization. However, humidified high flow nasal cannula (HHFNC) oxygen therapy (FiO2, 40%; flow, 40 L/min) was started from hospital day (HD) 2 owing to dyspnea worsening. On HD 3, remdesivir was discontinued because his heart rate decreased to 60/min, 6 hours after the second dose. From HD 4, oxygen saturation was maintained at > 96% and his RR at 21–30/min; subsequently, HHFNC flow was gradually reduced. Radiographic findings worsened until HD 3; then, gradual improvement was observed on serial follow-up radiographs (Fig. 2B and C). Oxygen supplementation was stopped on HD 8, and dyspnea at rest improved. He was discharged on HD 10 (Fig. 1).
Fig. 2
Serial chest radiographs. (A) HD 1: Chest PA on January 3, 2022, showed bilateral patchy, confluent, ground-glass opacity and consolidation in the mid to lower lung zones. (B) HD 3: Chest AP on January 5, 2022, showed increased extent of the diffuse bilateral opacities and consolidation in the left lower lung field. (C) HD 8: Chest AP on January 10, 2022, showed decreased bilateral opacities and consolidation. (D) At the outpatient clinic: Chest PA on January 27, 2022, showed radiographic improvement.
HD = hospital day, AP = anteroposterior, PA = posteroanterior.
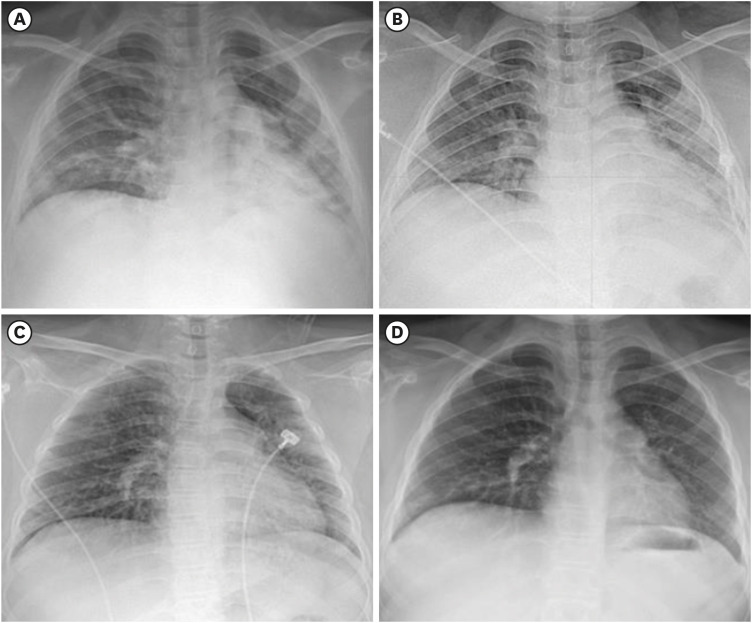
However, exertional dyspnea after discharge persisted, and chest radiography at the outpatient clinic showed no abnormalities (Fig. 2D). On February 18, 2022, 5 weeks post-discharge, pulmonary function tests were performed, yielding the following results: predicted forced vital capacity (FVC)%pred, 71%; forced expiratory volume in 1 second (FEV1%pred), 63%; FEV1/FVC, 0.81; and forced expiratory flow (FEF25-75%pred), 55% (Fig. 3). Chest tomography showed multifocal areas of parenchymal hyperlucency and mosaic attenuation in both lungs (Fig. 4). To detect other unidentified co-infections or etiologies, multiplex respiratory virus PCR (adenovirus, coronavirus HKU1/NL63/229E/OC43, human metapneumovirus, human rhinovirus, influenza A/B, parainfluenza 1–4, respiratory syncytial virus, Bordetella pertussis, Chlamydophila pneumoniae, MP) and mycoplasma antibody tests were performed, revealing no other infections. Therefore, we concluded that the patient had developed PIBO secondary to the SARS-COV-2 infection.
Fig. 3
Pulmonary function test at the time of PIBO diagnosis.
PIBO = postinfectious bronchiolitis obliterans, FVC = forced vital capacity, FEV1 = forced expiratory volume in 1 second, FEF = forced expiratory flow, PEF = peak expiratory flow, FET = forced expiratory time, FIVC = forced inspiratory vital capacity, FIV = forced inspiratory vital, MVV = maximum voluntary ventilation, ECode = error code, Vol Extrap = volume extrapolating, BTPS = body temperature and pressure saturated, pred = predicted.
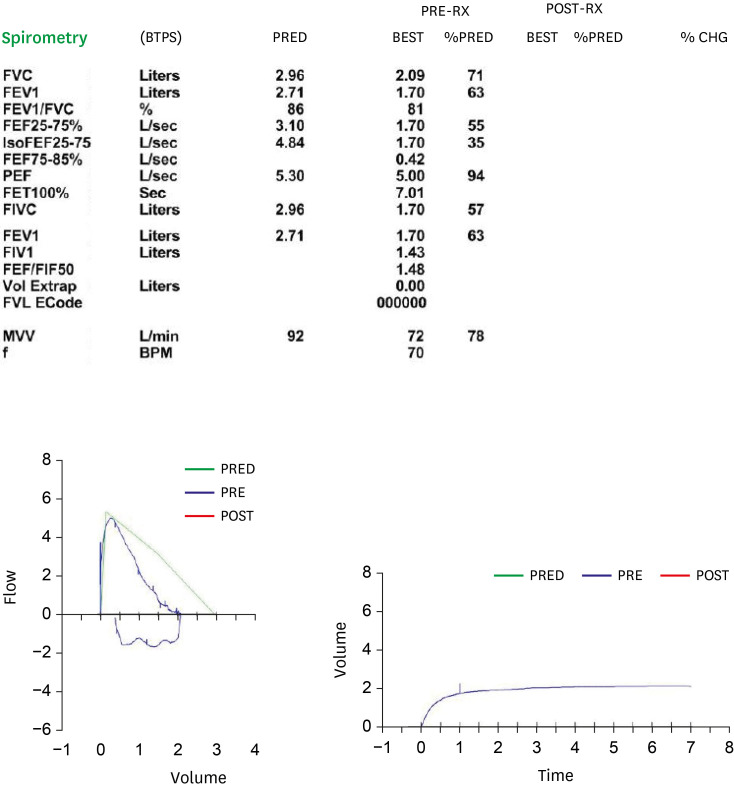
Fig. 4
Chest CT images at the time of postinfectious bronchiolitis obliterans diagnosis. Axial high-resolution CT images captured on February 18, 2022, showed parenchymal hyperlucency and mosaic attenuation in both lungs.
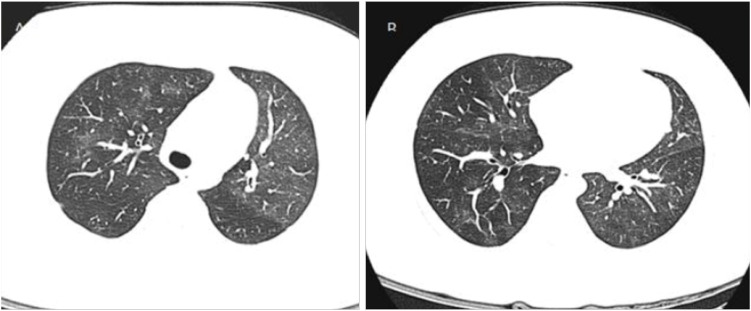
CT = computed tomography.
We treated this patient with three cycles of methylprednisolone pulse therapy (1,000 mg/day for 3 days, every 4 weeks).10 After treatment, dyspnea improved and spirometry showed improvement from FVC%pred 71% to 86%, FEV1%pred 63% to 72%, and FEF25-75%pred 55% to 68% with good prognosis.
DISCUSSION
Children and adolescents with COVID-19 are usually asymptomatic or have mild symptoms.11112 However, a few children with risk factors experience severe and permanent lung complications.1234 Here, PIBO developed after COVID-19 in a 10-year-old South Korean boy who was previously healthy, without history of asthma. However, he had a high BMI (30.13), history of late preterm birth (35 weeks), and was small for gestational age (1,850 g, 6th percentile). His twin brother, who was concurrently diagnosed with COVID-19 and was previously healthy, with a lower BMI and higher birth weight, experienced no post-COVID-19 respiratory complications (Table 1).
Reportedly, children with underlying medical conditions, e.g., neurologic conditions, congenital heart disease, diabetes mellitus, chronic pulmonary diseases, prematurity, or obesity, are at higher risk of severe COVID-19.131415 In a large multicenter cohort study with hospitalized children, obesity was an independent risk factor for critical illness in COVID-19.16 Several mechanisms have been suggested to explain the link between obesity and severe COVID-19. First, obesity reduces lung function, leading to increased respiratory energy consumption.17 Second, patients with obesity exhibit higher expression of angiotensin-converting enzyme 2 receptors, which are SARS-CoV-2 entry receptors.1718 Third, obesity is characterized by upregulated pro-inflammatory cytokines, e.g., tumor necrosis factor-α, IL-2, or IL-6.19 Elevated inflammatory-marker levels, including of IL-6, at admission were associated with severe pediatric COVID-19.20 Our patient also had elevated IL-6 levels at admission. Additionally, in a large population-based cohort study with adults, higher BMI was associated with higher risk of severe COVID-19.21 Here, a 10-year-old child with a higher BMI than his twin brother’s had higher oxygen demand and longer oxygen-supply demand duration due to COVID-19. These findings suggest that higher BMI may be associated with more severe COVID-19 in prepubertal children, as observed in adults.
Our patient had history of preterm birth and lower birth weight than his twin brother (Table 1). Reportedly, premature birth is related to the risk of severe COVID-19. However, it is unclear whether birth weight is related to severe COVID-19 independent of prematurity. A prospective cohort study showed that low birth weight was an independent risk factor for severe COVID-19 in non-elderly adults.22 Our case suggests that low birth weight may be associated with severe COVID-19 in children, as observed in adults.
Several studies have investigated risk factors for PIBO. A case-control study with children < 3 years old showed that adenovirus presence and need for mechanical ventilation were independently associated with increased PIBO risk.5 Furthermore, retrospective studies of children with MP pneumonia showed that poor response to MP pneumonia treatment and higher serum lactate dehydrogenase levels were risk factors for PIBO.2324 However, no study has reported that obesity is an independent risk factor for PIBO. Upregulated pro-inflammatory cytokines, e.g., tumor necrosis factor-α, IL-2, or IL-6, in obesity may contribute to PIBO development, and further studies are needed in the future.19
Severe viral infections, including adenovirus, influenza, parainfluenza, measles, respiratory syncytial virus, and varicella can cause PIBO, especially during the first 3 years of life.56 Coronaviruses, e.g., Middle East respiratory syndrome coronavirus (MERS-CoV), SARS-CoV, and SARS-CoV-2, can also involve the lower respiratory tract, inducing subepithelial inflammation.25262728 Further, several reports have shown that MERS-CoV can cause PIBO.28 In a few cases, PIBO developed after recovery from SARS-CoV-2-related pneumonia in children789; most patients were < 3 years old. Notably, our patient was a school-age child. To our knowledge, there have been no reported pediatric cases of PIBO developing after COVID-19 in the Korean population.
SARS-CoV-2 variant testing was not performed in our patient, but the SARS-CoV-2 B.1.617.2 (Delta) variant was prevalent in the community when he was diagnosed with COVID-19.29 Therefore, we assumed that he was infected with the Delta variant. The severe COVID-19 pneumonia incidence may decrease with the dominance of the SARS-CoV-2 B.1.1.529 (Omicron) variant, which mainly causes upper respiratory-tract infections.3031 However, COVID-19 severity according to the SARS-CoV-2 variant in children with risk factors should be investigated further. Moreover, this patient received only two doses of remdesivir, because of bradycardia occurrence, and intravenous dexamethasone (6 mg/day) for 8 days. Because our patient received shorter remdesivir treatment than his twin brother, it is necessary to investigate whether remdesivir contributed to the long-term COVID-19 complications. Moreover, further research is required for appropriate steroid duration, dose, and regimens to prevent COVID-19 lung complications.
There is potential risk of respiratory virus transmission during lung function testing. International societies, e.g., the European Respiratory Society and Italian Respiratory Society recommend that spirometry should be delayed for 30 days after SARS-COV-2 infection.32 Although spirometry was mostly normal for children with long-term respiratory symptoms after severe SARS-CoV-2 infection, as in this case, PIBO may occur in children with risk factors.33 Therefore, spirometry testing should be considered early in children with severe COVID-19 who have risk factors for respiratory complications.
We have reported a child with PIBO developed after severe COVID-19, and obesity and low birth weight may be considered risk factors in this case. Therefore, careful observation is necessary in children with persistent post-COVID-19 respiratory symptoms, especially in those with these risk factors. Further research is needed to clarify the pediatric risk factors for developing post-COVID-19 PIBO.
 XML Download
XML Download